You might also like
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Result, Discussion, Conclussion PlotDocument12 pagesResult, Discussion, Conclussion Plotnidya yunazNo ratings yet
- Minimum Clinically Important Improvement For The Incremental Shuttle Walking TestDocument4 pagesMinimum Clinically Important Improvement For The Incremental Shuttle Walking TestmavhelllinaNo ratings yet
- Tele RehabilitationDocument6 pagesTele Rehabilitationnidya yunazNo ratings yet
- Importance of Functional Capacity Assessment and Physical Exercise During and After Hospitalization in COVID-19 Patients Revisiting Pulmonary RehabilitationDocument3 pagesImportance of Functional Capacity Assessment and Physical Exercise During and After Hospitalization in COVID-19 Patients Revisiting Pulmonary RehabilitationIn House Training DialisisNo ratings yet
- Piquet 2021Document8 pagesPiquet 2021Manuel Amade OvalleNo ratings yet
- Preoperative PhysiotherapyDocument15 pagesPreoperative PhysiotherapysstavrosNo ratings yet
- Ankle Sprain CPR For ManipulationDocument13 pagesAnkle Sprain CPR For ManipulationChaim MalineNo ratings yet
- Pulmonary Rehabilitation in Patients With Interstitial Lung Diseases - Correlates of SuccessDocument1 pagePulmonary Rehabilitation in Patients With Interstitial Lung Diseases - Correlates of Successdr. Amori Amar LakcandraNo ratings yet
- IntervalexercisetrialAnnals2006 PDFDocument12 pagesIntervalexercisetrialAnnals2006 PDFrunmenNo ratings yet
- Jpts 27 2053Document4 pagesJpts 27 2053Julenda CintarinovaNo ratings yet
- Colorful Simple Science Class Education PresentationDocument13 pagesColorful Simple Science Class Education PresentationNi Luh Putu Winda AlpiniawatiNo ratings yet
- Effects of Inspiratory Muscle Training Using An Electronic Device On Patients Undergoing Cardiac Surgery: A Randomized Controlled TrialDocument9 pagesEffects of Inspiratory Muscle Training Using An Electronic Device On Patients Undergoing Cardiac Surgery: A Randomized Controlled TrialDaniel Lago BorgesNo ratings yet
- Respiratory Muscle Endurance Training With Normocapnic Hyperpnoea For Patients With Chronic Spinal Cord Injury: A Pilot Short-Term Randomized Controlled TrialDocument5 pagesRespiratory Muscle Endurance Training With Normocapnic Hyperpnoea For Patients With Chronic Spinal Cord Injury: A Pilot Short-Term Randomized Controlled TrialMarscha MaryuanaNo ratings yet
- Aerobic Training On Dyspnea Chest Wall CopdDocument8 pagesAerobic Training On Dyspnea Chest Wall CopdBunga Mitra MampuNo ratings yet
- Research Article Telerehabilitation Using Fitness Application in Patients With Severe Cystic Fibrosis Awaiting Lung Transplant: A Pilot StudyDocument7 pagesResearch Article Telerehabilitation Using Fitness Application in Patients With Severe Cystic Fibrosis Awaiting Lung Transplant: A Pilot StudyBayu PrabuNo ratings yet
- Pulmonary Rehabilitation & Exercise in CovidDocument4 pagesPulmonary Rehabilitation & Exercise in CovidsukiyantoNo ratings yet
- Jurnal 3Document4 pagesJurnal 3tri windartiNo ratings yet
- Tugas Farid PpokDocument9 pagesTugas Farid PpokUmmi AzizahNo ratings yet
- Rehabilitation - Extraction DataDocument58 pagesRehabilitation - Extraction DatamadrasahNo ratings yet
- Early Experiences of Rehabilitation For Individuals Post Covid To ImproveDocument4 pagesEarly Experiences of Rehabilitation For Individuals Post Covid To ImproveNaretta KhoirunnisakNo ratings yet
- Jurnal Pre-Eksperimental PDFDocument10 pagesJurnal Pre-Eksperimental PDFNica AuliaNo ratings yet
- Physiotherapy in Critically Ill Patients: ReviewDocument6 pagesPhysiotherapy in Critically Ill Patients: ReviewDaniela OrtizNo ratings yet
- Dronkers Et Al 2008 Prevention of Pulmonary Complications After Upper Abdominal Surgery by Preoperative IntensiveDocument9 pagesDronkers Et Al 2008 Prevention of Pulmonary Complications After Upper Abdominal Surgery by Preoperative Intensivechiendy.yNo ratings yet
- Anal EmergDocument1 pageAnal Emergwiki yabirNo ratings yet
- SMJ 63 105Document6 pagesSMJ 63 105OWL ANASNo ratings yet
- Pulmonary Rehabilitation in Recovering CovidDocument7 pagesPulmonary Rehabilitation in Recovering CovidsukiyantoNo ratings yet
- Weaning Ventilatorio en GB y MiasteniaDocument4 pagesWeaning Ventilatorio en GB y MiasteniaJorgeNo ratings yet
- Remote Exercise Testing For Respiratory Disease During Covid 19Document18 pagesRemote Exercise Testing For Respiratory Disease During Covid 19Chelsea Shannen Marie CarreonNo ratings yet
- Thoracic Surgery 2015 PDFDocument4 pagesThoracic Surgery 2015 PDFDevi SiswaniNo ratings yet
- Garnacho Montero2005Document6 pagesGarnacho Montero2005EviNo ratings yet
- Rehabilitation For post-COVID-19 Condition Through ADocument11 pagesRehabilitation For post-COVID-19 Condition Through Aelieser toding mendilaNo ratings yet
- Effect of TENS On PADDocument12 pagesEffect of TENS On PADAyesha SmcNo ratings yet
- Effects of Early Exercise Rehabilitation On Functional Recovery in Patients With Severe SepsisDocument9 pagesEffects of Early Exercise Rehabilitation On Functional Recovery in Patients With Severe SepsisRodrigoSachiFreitasNo ratings yet
- Telerehab InterventionDocument12 pagesTelerehab InterventionNelson LoboNo ratings yet
- Articulo NeumoniaDocument7 pagesArticulo NeumoniaHarby Noguera HerreraNo ratings yet
- Bjsports 2022 106681.fullDocument44 pagesBjsports 2022 106681.fullThiago SartiNo ratings yet
- PIIS0954611121003565Document8 pagesPIIS0954611121003565Maria Luiza YamamotoNo ratings yet
- Swallowing Rehabilitation Following Spinal Injury A Case SeriesDocument12 pagesSwallowing Rehabilitation Following Spinal Injury A Case SeriesniekoNo ratings yet
- TMI - Capacidade Funcional Após Artéria Coronária de Cirurgia de Revascularização em Pacientes de Alto RiscoDocument6 pagesTMI - Capacidade Funcional Após Artéria Coronária de Cirurgia de Revascularização em Pacientes de Alto Risco56zw8rqq6jNo ratings yet
- MainDocument6 pagesMainnisalazarvNo ratings yet
- Selective Dorsal Rhizotomy For The Treatment of Severe Spastic Cerebral Palsy - Efficacy and Therapeutic Durability in GMFCS Grade IV and V ChildrenDocument11 pagesSelective Dorsal Rhizotomy For The Treatment of Severe Spastic Cerebral Palsy - Efficacy and Therapeutic Durability in GMFCS Grade IV and V ChildrenAlvaro Perez HenriquezNo ratings yet
- Acta Physiologica - 2021 - PostersDocument11 pagesActa Physiologica - 2021 - PostersHamza SaidiNo ratings yet
- Artros Cadera Programa de EjercDocument11 pagesArtros Cadera Programa de EjercgeorginaNo ratings yet
- 1 s2.0 S2451865421000442 MainDocument4 pages1 s2.0 S2451865421000442 Maindewa anggaNo ratings yet
- Stroke InfarkDocument9 pagesStroke InfarkNadia Mrz Mattew MuseNo ratings yet
- Bernocchi-2018-Home-based Telerehabilitation IDocument7 pagesBernocchi-2018-Home-based Telerehabilitation IJonathanNo ratings yet
- AC - TelefisioterapiaDocument3 pagesAC - TelefisioterapiaPRehabilita Centro de Fisioterapia y FitnessNo ratings yet
- tmp7403 TMPDocument2 pagestmp7403 TMPFrontiersNo ratings yet
- Bijender Sindhu, DR - Manoj Sharma, DR - Raj K Biraynia. Comparison of Clinic and Home Based Exercise Programs After Total Knee Arthroplasty A Pilot StudyDocument12 pagesBijender Sindhu, DR - Manoj Sharma, DR - Raj K Biraynia. Comparison of Clinic and Home Based Exercise Programs After Total Knee Arthroplasty A Pilot StudyDr. Krishna N. SharmaNo ratings yet
- Clinical Respiratory J - 2018 - Beaumont - Effects of Inspiratory Muscle Training in COPD Patients A Systematic Review andDocument11 pagesClinical Respiratory J - 2018 - Beaumont - Effects of Inspiratory Muscle Training in COPD Patients A Systematic Review andAlejandra Castro BelloNo ratings yet
- Large Scale Implementation of A Respiratory Therapist WESLEY ELYDocument8 pagesLarge Scale Implementation of A Respiratory Therapist WESLEY ELYKinesio FernandezNo ratings yet
- Original Article Correlation Between FEV1 Percentage Predicted and 6 Minute Walk Distance in Patients of Chronic Obstructive Pulmonary DiseaseDocument5 pagesOriginal Article Correlation Between FEV1 Percentage Predicted and 6 Minute Walk Distance in Patients of Chronic Obstructive Pulmonary DiseaseSri HariNo ratings yet
- Efectos Extrapulmonares en CovidDocument7 pagesEfectos Extrapulmonares en Covidjonny rualesNo ratings yet
- Factors Associated With Recovery of Activities of Daily Living in Elderly Pneumonia PatientsDocument8 pagesFactors Associated With Recovery of Activities of Daily Living in Elderly Pneumonia PatientsAffuadiNo ratings yet
- Research Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailureDocument7 pagesResearch Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailurewiwiNo ratings yet
- Care of The Hospitalized Patient With Acute Exacerbation of CopdDocument25 pagesCare of The Hospitalized Patient With Acute Exacerbation of CopdmiallyannaNo ratings yet
- Can Vestibular Rehabilitation Exercises Help Patients With Concussion? A Systematic Review of Ef Ficacy, Prescription and Progression PatternsDocument12 pagesCan Vestibular Rehabilitation Exercises Help Patients With Concussion? A Systematic Review of Ef Ficacy, Prescription and Progression PatternsJuan Pedro BarrientosNo ratings yet
- Home BasedDocument10 pagesHome BasedMaría Camila Zuluaga AriasNo ratings yet
- Physiotherapy and Weaning From Prolonged Mechanical VentilationDocument9 pagesPhysiotherapy and Weaning From Prolonged Mechanical VentilationdanielNo ratings yet
- Telerehab InterventionDocument12 pagesTelerehab InterventionNelson LoboNo ratings yet
- Telerehab in Covid and CopdDocument13 pagesTelerehab in Covid and CopdNelson LoboNo ratings yet
- Pakistan DyspneaDocument7 pagesPakistan DyspneaNelson LoboNo ratings yet
- Tele DiabDocument10 pagesTele DiabNelson LoboNo ratings yet
- All India Institute of Physical Medicine and Rehabilitation, MumbaiDocument2 pagesAll India Institute of Physical Medicine and Rehabilitation, MumbaiNelson LoboNo ratings yet
- COVID-19 Pandemic in India: Present Scenario and A Steep Climb AheadDocument4 pagesCOVID-19 Pandemic in India: Present Scenario and A Steep Climb AheadSafikul HossainNo ratings yet
- Quality of Life of COVID 19 Patients After Discharge: Systematic ReviewDocument12 pagesQuality of Life of COVID 19 Patients After Discharge: Systematic ReviewNelson LoboNo ratings yet
- Upper Limb NeuropathiesDocument36 pagesUpper Limb NeuropathiesNelson LoboNo ratings yet
- Details of Exam and Instructions To StudentsDocument2 pagesDetails of Exam and Instructions To StudentsNelson LoboNo ratings yet
- Student Undertaking - MPT Entrance ExaminationDocument2 pagesStudent Undertaking - MPT Entrance ExaminationNelson LoboNo ratings yet
- By - Aishwarya PoreDocument38 pagesBy - Aishwarya PoreNelson LoboNo ratings yet
- Pneumonitis: - Nelson LoboDocument14 pagesPneumonitis: - Nelson LoboNelson LoboNo ratings yet
- BronchiectasisDocument7 pagesBronchiectasisNelson LoboNo ratings yet
- Revise Anatomy in 15 Days K Raviraj VD AgrawalDocument9 pagesRevise Anatomy in 15 Days K Raviraj VD AgrawalNelson LoboNo ratings yet
- Research Questionnaire: Direction: Put A Check Under The Column That Best Suit Your ExperienceDocument2 pagesResearch Questionnaire: Direction: Put A Check Under The Column That Best Suit Your ExperienceChloie Marie RosalejosNo ratings yet
- Report Minor Project Ucs1173Document8 pagesReport Minor Project Ucs1173Nurul IffahNo ratings yet
- Physical Education and Health 1: Aerobic, Muscle-And Bone Strength ActivitiesDocument19 pagesPhysical Education and Health 1: Aerobic, Muscle-And Bone Strength ActivitiesPia Alexie NollanNo ratings yet
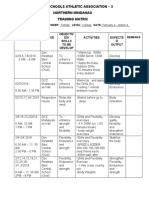
- Private Schools Athletic Association - X Northern Mindanao Training MatrixDocument2 pagesPrivate Schools Athletic Association - X Northern Mindanao Training MatrixNica Ilano100% (1)
- How To Double Your Vertical Jump For BasketballDocument10 pagesHow To Double Your Vertical Jump For BasketballReaper UnseenNo ratings yet
- Collecting Subjective Data: Health AssessmentDocument83 pagesCollecting Subjective Data: Health AssessmentChriscell Gipanao Eustaquio100% (1)
- Respiratory Physiology & NeurobiologyDocument14 pagesRespiratory Physiology & NeurobiologyRaul DoctoNo ratings yet
- Fittp and Red Flags TabulationDocument3 pagesFittp and Red Flags Tabulationchca.obero.swuNo ratings yet
- PT 1 Activity Sheet - Stress Management-3-1-2Document7 pagesPT 1 Activity Sheet - Stress Management-3-1-2Andrei AlcantaraNo ratings yet
- Ffects of Tabata Training During Physical EducationDocument11 pagesFfects of Tabata Training During Physical EducationNursahanizaNo ratings yet
- Health Effects of Cigarette Smoking Vanessa BenningDocument4 pagesHealth Effects of Cigarette Smoking Vanessa Benningapi-489132887No ratings yet
- Physiotherapy and Mental HealthDocument27 pagesPhysiotherapy and Mental Healthlilz_rodriguesNo ratings yet
- Building A Community ParkDocument10 pagesBuilding A Community Parkanon_611253013No ratings yet
- Happy/sad Music Affects How We See Neutral Faces:: Affects Our Brains and BodiesDocument8 pagesHappy/sad Music Affects How We See Neutral Faces:: Affects Our Brains and BodiesStefan ChrisnawanNo ratings yet
- 7 Habits To Keep Your Mind Active With AgeDocument11 pages7 Habits To Keep Your Mind Active With AgeOscar Giovanni Linares TrivinoNo ratings yet
- Effectiveness of Proprioceptive Training and Aerobic Exercise On Balance in Diabetic Peripheral NeuropathyDocument6 pagesEffectiveness of Proprioceptive Training and Aerobic Exercise On Balance in Diabetic Peripheral Neuropathyzamren kafelaNo ratings yet
- Fit Father Calorie Calculator - 2019Document8 pagesFit Father Calorie Calculator - 2019Andres Aravena0% (1)
- Activity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020Document10 pagesActivity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020RJ TacataNo ratings yet
- Sport and Physical Education Dissertation IdeasDocument6 pagesSport and Physical Education Dissertation IdeasPaySomeoneToWriteAPaperForMeCanada100% (1)
- Answers To Frequently Asked Questions On: Gabriel "Venom" Wilson Created by The Members of AbcbodybuildingDocument26 pagesAnswers To Frequently Asked Questions On: Gabriel "Venom" Wilson Created by The Members of AbcbodybuildingPedro HenriqueNo ratings yet
- 4x4 WorkoutDocument4 pages4x4 WorkoutMEIBNo ratings yet
- Paul Chek - How To Eat, Move and Be Healthy-C.H.E.K. Institute (2017)Document253 pagesPaul Chek - How To Eat, Move and Be Healthy-C.H.E.K. Institute (2017)shyaambablou86% (7)
- WNL - 10 Biggest Myths in Fitness-UpperDocument4 pagesWNL - 10 Biggest Myths in Fitness-UpperRosa OSNo ratings yet
- Talwalkars Fitness Solutions PVT LTDDocument47 pagesTalwalkars Fitness Solutions PVT LTDrahul19081986No ratings yet
- 5 Simple Ways To End Anxiety and Panic AttacksDocument9 pages5 Simple Ways To End Anxiety and Panic AttacksNasseh WachemNo ratings yet
- Training Distance Runners: by Todd Thorson Ipswich SchoolDocument36 pagesTraining Distance Runners: by Todd Thorson Ipswich SchoolYared TegegneNo ratings yet
- THE FILIPINO PYRAMID ACTIVITY - Grade VIDocument8 pagesTHE FILIPINO PYRAMID ACTIVITY - Grade VIRoger Salvador100% (3)
- Lesson 1: Understanding The Aerobics Exercise: College of Human KineticsDocument7 pagesLesson 1: Understanding The Aerobics Exercise: College of Human KineticsCamille CarengNo ratings yet
- What Is The Need of Diet Control in DiabetesDocument13 pagesWhat Is The Need of Diet Control in DiabetesPabhat KumarNo ratings yet
- 3RD Quater Lesson PlanDocument10 pages3RD Quater Lesson PlanRomy Renz SanoNo ratings yet