You might also like
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDocument9 pagesGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentSteven Junius Chandra100% (2)
- FDAR and 12 14Document4 pagesFDAR and 12 14Jay VillasotoNo ratings yet
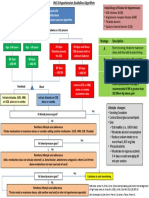
- Algoritma Terapi JNC 8 Hypertension GuidelineDocument3 pagesAlgoritma Terapi JNC 8 Hypertension GuidelineRhenty NarusNo ratings yet
- Problem-Free Diabetes: Controlling Diabetes With the Help of The Power of Your MetabolismFrom EverandProblem-Free Diabetes: Controlling Diabetes With the Help of The Power of Your MetabolismRating: 4.5 out of 5 stars4.5/5 (4)
- 2014-JNC-8-Hypertension WRDocument2 pages2014-JNC-8-Hypertension WRismailuntung0% (1)
- 2014 JNC 8 HypertensionDocument2 pages2014 JNC 8 Hypertensionaudreynabilaf100% (1)
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDocument2 pagesGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentLalu Ranova100% (1)
- 2 Algoritma HT JNC 8Document3 pages2 Algoritma HT JNC 8Nais Maghfiroh100% (1)
- 2 Algoritma HT JNC 8Document3 pages2 Algoritma HT JNC 8Nais MaghfirohNo ratings yet
- PDF JNC 8 Guidelines - CompressDocument2 pagesPDF JNC 8 Guidelines - Compressnaila inayatiNo ratings yet
- 2014 JNC 8 HypertensionDocument2 pages2014 JNC 8 HypertensionAhmad MuzakiNo ratings yet
- General Population Diabetes or CKD Present (No Diabetes or CKD)Document2 pagesGeneral Population Diabetes or CKD Present (No Diabetes or CKD)anon_324793200No ratings yet
- JNC 8 Hypertension Guideline AlgorithmDocument8 pagesJNC 8 Hypertension Guideline AlgorithmdeaNo ratings yet
- 2014 JNC 8 HypertensionDocument2 pages2014 JNC 8 HypertensionJane GreenNo ratings yet
- JNC8 HTNDocument2 pagesJNC8 HTNTaradifaNurInsi0% (1)
- 2014 JNC 8 HypertensionDocument2 pages2014 JNC 8 HypertensionEndy Garret BongartzNo ratings yet
- 27 JNC8 HTNGuidelines Book BookletDocument2 pages27 JNC8 HTNGuidelines Book BookletCitra Resmi DewantiNo ratings yet
- JNC8 HTNGuidelines Book BookletDocument2 pagesJNC8 HTNGuidelines Book BookletDestya SNNo ratings yet
- JNC 8 HypertensionDocument2 pagesJNC 8 HypertensionMuhammad LutfiNo ratings yet
- 2014 JNC 8 Hypertension - 221105 - 134757Document3 pages2014 JNC 8 Hypertension - 221105 - 134757Ei lessonNo ratings yet
- Algoritma Tatalaksana HTDocument2 pagesAlgoritma Tatalaksana HTUswatun Hasanah RINo ratings yet
- HTN AlgorhythmDocument2 pagesHTN AlgorhythmLottie EverettNo ratings yet
- 2014 JNC 8 HypertensionDocument3 pages2014 JNC 8 HypertensionFernandez-De Ala NicaNo ratings yet
- Algoritma JNC 8 (JNC 8 Figure)Document1 pageAlgoritma JNC 8 (JNC 8 Figure)anang7100% (1)
- Non-Pharmacological Treatment of HypertensionDocument25 pagesNon-Pharmacological Treatment of Hypertensionastrid abrahams0% (2)
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDocument1 pageGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentMuthia ArsilNo ratings yet
- DASH Diet for Beginners: The Ultimate Healthy Eating Solution and Weight Loss Program for Hypertension and Blood Pressure By Learning The Power of the DASH Diet!From EverandDASH Diet for Beginners: The Ultimate Healthy Eating Solution and Weight Loss Program for Hypertension and Blood Pressure By Learning The Power of the DASH Diet!No ratings yet
- DASH Diet Weight Loss Motivation: A Foolproof Healthy Eating Solution To Easing The Symptoms of Hypertension And High Blood PressureFrom EverandDASH Diet Weight Loss Motivation: A Foolproof Healthy Eating Solution To Easing The Symptoms of Hypertension And High Blood PressureNo ratings yet
- DASH Diet: The Dash diet for beginners, DASH recipes, and teaching you how to lose weight with DASH fast!From EverandDASH Diet: The Dash diet for beginners, DASH recipes, and teaching you how to lose weight with DASH fast!No ratings yet
- DASH Diet: A Complete Guide to the Dash Diet for Lowering Blood Pressure and Weight Loss, Including Tips, Recipes, and More!From EverandDASH Diet: A Complete Guide to the Dash Diet for Lowering Blood Pressure and Weight Loss, Including Tips, Recipes, and More!No ratings yet
- The Dash Diet: A Beginner's Guide - Tips, Recipes, 7-Day Meal Plan to Lower Blood Pressure, and Getting HealthyFrom EverandThe Dash Diet: A Beginner's Guide - Tips, Recipes, 7-Day Meal Plan to Lower Blood Pressure, and Getting HealthyNo ratings yet
- DASH Diet : The Ultimate DASH Diet Guide to Lose Weight, Lower Blood Pressure, and Stop Hypertension FastFrom EverandDASH Diet : The Ultimate DASH Diet Guide to Lose Weight, Lower Blood Pressure, and Stop Hypertension FastNo ratings yet
- The Chronic Disease of Obesity: How Sponge Syndrome Causes Repeated Weight GainFrom EverandThe Chronic Disease of Obesity: How Sponge Syndrome Causes Repeated Weight GainNo ratings yet
- DASH DIET COOKBOOK: Nourishing Recipes to Lower Blood Pressure, Boost Heart Health, and Achieve Long-Term Well-Being (2024 Guide)From EverandDASH DIET COOKBOOK: Nourishing Recipes to Lower Blood Pressure, Boost Heart Health, and Achieve Long-Term Well-Being (2024 Guide)No ratings yet
- Ketogenic Diet "Yes & No" Guide For BeginnersFrom EverandKetogenic Diet "Yes & No" Guide For BeginnersRating: 3 out of 5 stars3/5 (1)
- CBD oil for Weight-Loss?: Suppress Your Cravings & Satisfy Your Appetite! Start Losing Weight Within 30 Days! Includes Delicious Keto Fat Burning Recipes Curb Your Binge Eating Habits!From EverandCBD oil for Weight-Loss?: Suppress Your Cravings & Satisfy Your Appetite! Start Losing Weight Within 30 Days! Includes Delicious Keto Fat Burning Recipes Curb Your Binge Eating Habits!No ratings yet
- Dash Diet Cookbook: Easy and Healthy Dash Diet Recipes to Lower Your Blood Pressure. 7-Day Meal Plan and 7 Simple Rules for Weight LossFrom EverandDash Diet Cookbook: Easy and Healthy Dash Diet Recipes to Lower Your Blood Pressure. 7-Day Meal Plan and 7 Simple Rules for Weight LossNo ratings yet
- The Wonder of DASH Diet: The No-Fluff Guide to Lowering High Blood Pressure, Losing Weight Fast, & Improving Health with the DASH Diet - Delicious Recipes & Meal Plan IncludedFrom EverandThe Wonder of DASH Diet: The No-Fluff Guide to Lowering High Blood Pressure, Losing Weight Fast, & Improving Health with the DASH Diet - Delicious Recipes & Meal Plan IncludedNo ratings yet
- DASH Diet: The DASH Diet Guide with Delicious DASH Recipes for Weight LossFrom EverandDASH Diet: The DASH Diet Guide with Delicious DASH Recipes for Weight LossNo ratings yet
- 200 Low-Carb High-Fat Recipes: Easy Recipes to Jumpstart Your Low-Carb Weight LossFrom Everand200 Low-Carb High-Fat Recipes: Easy Recipes to Jumpstart Your Low-Carb Weight LossRating: 2 out of 5 stars2/5 (1)
- The Dash Diet: Lower Blood Pressure Lose Weight And Feel GreatFrom EverandThe Dash Diet: Lower Blood Pressure Lose Weight And Feel GreatNo ratings yet
- A Simple Guide to Hypertension and Heart DiseasesFrom EverandA Simple Guide to Hypertension and Heart DiseasesRating: 5 out of 5 stars5/5 (1)
- The DASH Diet for Beginners: Your Guide to Weight Loss and Healthy LivingFrom EverandThe DASH Diet for Beginners: Your Guide to Weight Loss and Healthy LivingNo ratings yet
- The Natural way to Beat Chronic Diabetes: Diabetes 101: Practical Tips to Manage Diabetes, Prediabetes and Boost Your WellbeingFrom EverandThe Natural way to Beat Chronic Diabetes: Diabetes 101: Practical Tips to Manage Diabetes, Prediabetes and Boost Your WellbeingNo ratings yet
- D Received Patient Sitting On Bed With Bottle # 1DDocument24 pagesD Received Patient Sitting On Bed With Bottle # 1DMai Love100% (5)
- GuidelinesDocument151 pagesGuidelinesM. A.V.No ratings yet
- Jurnal CTMDocument10 pagesJurnal CTMFahrul ComisterNo ratings yet
- Advances in Solid Dispersion Techniques For Enhancing Drug Solubility, Bioavailability and Controlled ReleaseDocument5 pagesAdvances in Solid Dispersion Techniques For Enhancing Drug Solubility, Bioavailability and Controlled ReleaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Herbals and BreastfeedingDocument8 pagesHerbals and BreastfeedingArshad SyahaliNo ratings yet
- Medical Inventory VITODocument4 pagesMedical Inventory VITOJagjit SinghNo ratings yet
- Young 2017 Cardiac Sarcoidosis TreatmentDocument15 pagesYoung 2017 Cardiac Sarcoidosis TreatmentJohan ArocaNo ratings yet
- NeurotransmittersDocument19 pagesNeurotransmittersSushmit KishoreNo ratings yet
- Career PortfolioDocument12 pagesCareer PortfolioNatasya Fariha ShafiiNo ratings yet
- Oklahoma Et Al v. Johnson & Johnson Et AlDocument42 pagesOklahoma Et Al v. Johnson & Johnson Et AlDoug MataconisNo ratings yet
- Kuliah Farmakologi - Farmakokinetik Dan Farmakodinamik Antivirus Dan Antiparasit Secara UmumDocument87 pagesKuliah Farmakologi - Farmakokinetik Dan Farmakodinamik Antivirus Dan Antiparasit Secara UmumGabriel AnindhitaNo ratings yet
- Review Shukla 2000 BunDocument9 pagesReview Shukla 2000 BunGeorgiana Cozma FrunzăNo ratings yet
- Neuroprotective Effects of Ginkgo Biloba ExtractDocument14 pagesNeuroprotective Effects of Ginkgo Biloba Extractcpt-n3moNo ratings yet
- Holidays Home Work Class 12Document2 pagesHolidays Home Work Class 12Mark TwainNo ratings yet
- Benefits of Vitamine B1 - Structure, Function and UseDocument4 pagesBenefits of Vitamine B1 - Structure, Function and UseCarl MacCordNo ratings yet
- Hypoglycemia: Manage Well, Live WellDocument4 pagesHypoglycemia: Manage Well, Live WellHashim Mushtasin RezaNo ratings yet
- Etiology of HypertensionDocument7 pagesEtiology of HypertensionAdelia Maharani DNo ratings yet
- Pharm Exam 4 ReviewDocument2 pagesPharm Exam 4 ReviewHwi GNDCNo ratings yet
- Jadavpur University: CollegeDocument22 pagesJadavpur University: CollegekuntaljuNo ratings yet
- Form Stock ObatDocument7 pagesForm Stock ObatSyarifahUniqueNo ratings yet
- Antiinflammatory Activity of Tenoxicam Gel On Carrageenaninduced Paw Oedema in RatsDocument4 pagesAntiinflammatory Activity of Tenoxicam Gel On Carrageenaninduced Paw Oedema in RatsRamling PatrakarNo ratings yet
- Therapeutic Classification of Drugs Based On The Philippine National Drug FormularyDocument25 pagesTherapeutic Classification of Drugs Based On The Philippine National Drug FormularyJelight Faith Salero GachoNo ratings yet
- Medicinal Chemistry: AnalgesicsDocument6 pagesMedicinal Chemistry: AnalgesicsAlishba MushtaqNo ratings yet
- Heartjnl 2019 314702 Inline Supplementary Material 2Document3 pagesHeartjnl 2019 314702 Inline Supplementary Material 2البكالوريوس المكثف فى التمريضNo ratings yet
- Naproxen Drug StudyDocument4 pagesNaproxen Drug StudyTimz GatdulaNo ratings yet
- Colocalisation of Neuropeptides, Nitric Oxide Synthase and Immunomarkers For Catecholamines in Nerve Fibres of The Adult Human Vas DeferensDocument9 pagesColocalisation of Neuropeptides, Nitric Oxide Synthase and Immunomarkers For Catecholamines in Nerve Fibres of The Adult Human Vas DeferensFlavia DinizNo ratings yet
- Dr. Vaibhav KulkarniDocument1 pageDr. Vaibhav KulkarniJake KNo ratings yet
- A History of Pharmacy in PicturesDocument41 pagesA History of Pharmacy in PicturesAnaNo ratings yet
- Kardex: 01-06-2021 Nicardipine Drip 10 MG + 90 CC PNSS Start at 15 Ugtts/minDocument2 pagesKardex: 01-06-2021 Nicardipine Drip 10 MG + 90 CC PNSS Start at 15 Ugtts/minRenea Joy ArruejoNo ratings yet