You might also like
- 7.1 Summary of ContributionsDocument10 pages7.1 Summary of ContributionsHussainNo ratings yet
- Telemedicine SystemsDocument25 pagesTelemedicine SystemsRohitash GuptaNo ratings yet
- Patient Monitoring System Project Report OriginalDocument84 pagesPatient Monitoring System Project Report OriginalAmar Dharmadhikari62% (13)
- Miniaturized Reveal LINQ Insertable Cardiac MonitoDocument7 pagesMiniaturized Reveal LINQ Insertable Cardiac MonitoLetícia JanuziNo ratings yet
- Efficacy and Feasibility of A Mobile Ecg Decision Support System - A Preliminary Conceptual ModelDocument8 pagesEfficacy and Feasibility of A Mobile Ecg Decision Support System - A Preliminary Conceptual ModelChandan PradhanNo ratings yet
- Research and Development of Smart Health Monitoring System: Department of E.C.E - S.V.I.T - Seminar ReportDocument33 pagesResearch and Development of Smart Health Monitoring System: Department of E.C.E - S.V.I.T - Seminar ReportVinay KumarNo ratings yet
- Multi-Parameter Measurement of ICU Patient Using GSM and Embedded TechnologyDocument5 pagesMulti-Parameter Measurement of ICU Patient Using GSM and Embedded TechnologyInternational Journal of Engineering Inventions (IJEI)No ratings yet
- Sensors 15 02181Document24 pagesSensors 15 02181Alice AmaratyaNo ratings yet
- Wavelet-Based ECG Steganography For Protecting Patient Confidential Information in Point-of-Care SystemsDocument9 pagesWavelet-Based ECG Steganography For Protecting Patient Confidential Information in Point-of-Care SystemsasasasasNo ratings yet
- Implementing An Electronic Observation and Early Warning Score Chart in The Emergency Department: A Feasibility StudyDocument6 pagesImplementing An Electronic Observation and Early Warning Score Chart in The Emergency Department: A Feasibility StudyHening Tirta KusumawardaniNo ratings yet
- Health Structure Monitoring and Tracking Using WSN: Mohaneesh Mitkari & Maruti LimkarDocument8 pagesHealth Structure Monitoring and Tracking Using WSN: Mohaneesh Mitkari & Maruti LimkarTJPRC PublicationsNo ratings yet
- Nursing Care of The Mechanically Ventilated Patient: What Does The Evidence Say? Part OneDocument11 pagesNursing Care of The Mechanically Ventilated Patient: What Does The Evidence Say? Part OneBahaa Ahmad AssoudNo ratings yet
- Arduino Based Human Health Care Monitori PDFDocument10 pagesArduino Based Human Health Care Monitori PDFAdriana OnticaNo ratings yet
- ECG Based Human Authentication: A Review: Meenakshi Nawal, G.N PurohitDocument8 pagesECG Based Human Authentication: A Review: Meenakshi Nawal, G.N PurohitPhạm Minh KhuêNo ratings yet
- A Tele-surveillance System for ECG ClassificationDocument6 pagesA Tele-surveillance System for ECG ClassificationKarthik SNo ratings yet
- Surgical Hot Telephone Clinic: A Safe Alternative To Face-To-Face Hot ClinicDocument10 pagesSurgical Hot Telephone Clinic: A Safe Alternative To Face-To-Face Hot ClinicIJAR JOURNALNo ratings yet
- Physiological Signal Monitoring SystemDocument5 pagesPhysiological Signal Monitoring SystemBira VekNo ratings yet
- GPS and GPRS Based Tele Monitoring System For Emergency Patient TransportationDocument8 pagesGPS and GPRS Based Tele Monitoring System For Emergency Patient TransportationRam ChandiranNo ratings yet
- 02.2.16 - Cama de FBGs FBG-based Smart Bed System For HealthcarDocument6 pages02.2.16 - Cama de FBGs FBG-based Smart Bed System For HealthcarRenan Costa LazaroNo ratings yet
- Interactive posture and health monitoring system for patientsDocument6 pagesInteractive posture and health monitoring system for patientsSowmya PNo ratings yet
- Design Open Source Remote ECG Service Under 40 CharactersDocument19 pagesDesign Open Source Remote ECG Service Under 40 Charactersmuhamad ilhamNo ratings yet
- Penn Tate: Wireless Sensor and Monitoring System For Intensive Care Unit (ICU) PatientsDocument1 pagePenn Tate: Wireless Sensor and Monitoring System For Intensive Care Unit (ICU) PatientsEMADNo ratings yet
- Using Wireless Networks For Enhanced Monitoring of PatientsDocument9 pagesUsing Wireless Networks For Enhanced Monitoring of PatientsPartho Kumar DuttaNo ratings yet
- Reliable Real-Time Clinical Monitoring Using Sensor Network TechnologyDocument5 pagesReliable Real-Time Clinical Monitoring Using Sensor Network TechnologydddemysNo ratings yet
- Research Article: Integration of 5G and Block-Chain Technologies in Smart Telemedicine Using IotDocument18 pagesResearch Article: Integration of 5G and Block-Chain Technologies in Smart Telemedicine Using IotBayu PrabuNo ratings yet
- Real-Time Heart Pulse Monitoring Technique Using WDocument9 pagesReal-Time Heart Pulse Monitoring Technique Using WAndreea IlieNo ratings yet
- TELECARDIOLOGYDocument11 pagesTELECARDIOLOGYNancy Prasad100% (1)
- UNIT 3 - Information Technology System Applicable in Nursing PracticeDocument85 pagesUNIT 3 - Information Technology System Applicable in Nursing PracticeRaquel MonsalveNo ratings yet
- The Integration of Wearable Devices in Cardiovascular TrialsDocument3 pagesThe Integration of Wearable Devices in Cardiovascular Trialsjaya sharmaNo ratings yet
- A Large-Scale Clinical Validation of An Integrated Monitoring System in The Emergency DepartmentDocument8 pagesA Large-Scale Clinical Validation of An Integrated Monitoring System in The Emergency DepartmentSudhakar SpartanNo ratings yet
- Endoscopic Axillary Lymph Node Retrieval For Breast Cancer PDF 1899863224702405Document6 pagesEndoscopic Axillary Lymph Node Retrieval For Breast Cancer PDF 1899863224702405MariajanNo ratings yet
- TelecardiologyDocument20 pagesTelecardiologyPushpavalli Mohan100% (1)
- Wireless Health Care MonitoringDocument6 pagesWireless Health Care Monitoringking philipNo ratings yet
- Ni RevDocument12 pagesNi RevJaslir MendozaNo ratings yet
- Embedded Based Real-Time Patient Monitoring SystemDocument5 pagesEmbedded Based Real-Time Patient Monitoring SystemTabithaDsouza50% (2)
- Design of Advanced Electronic Biomedical SystemsDocument11 pagesDesign of Advanced Electronic Biomedical SystemsIJAET JournalNo ratings yet
- Patient Health Management System Using E-Health Monitoring ArchitectureDocument7 pagesPatient Health Management System Using E-Health Monitoring Architecturejayesh tahasildarNo ratings yet
- A. Background of The StudyDocument4 pagesA. Background of The Studyyin0110yangNo ratings yet
- Real-time ECG and saline monitoring using ArduinoDocument5 pagesReal-time ECG and saline monitoring using ArduinostevebensonNo ratings yet
- Cardiac Design Labs Telemetric Patient Monitoring SystemDocument6 pagesCardiac Design Labs Telemetric Patient Monitoring SystemAkshay KaushikNo ratings yet
- Real-Time Remote Monitoring Cardiac Patients at Distance: Openecg Workshop 2004, Berlin, GermanyDocument3 pagesReal-Time Remote Monitoring Cardiac Patients at Distance: Openecg Workshop 2004, Berlin, GermanydawadhaliNo ratings yet
- Name:: 1. Ahmad Ardi Pratama 2. Muhammad Eri HDocument11 pagesName:: 1. Ahmad Ardi Pratama 2. Muhammad Eri HAhmad Ardi PratamaNo ratings yet
- Mechanical Complications After Central Venous Catheterisation in The Ultrasound-Guided Era: A Prospective Multicentre Cohort StudyDocument8 pagesMechanical Complications After Central Venous Catheterisation in The Ultrasound-Guided Era: A Prospective Multicentre Cohort StudyResidencia SSC ClínicaNo ratings yet
- Paper Su Case Study Medicina Lotti PontederaDocument2 pagesPaper Su Case Study Medicina Lotti PontederaronnyNo ratings yet
- Real-Time ECG Telemonitoring System Design With Mobile Phone PlatformDocument8 pagesReal-Time ECG Telemonitoring System Design With Mobile Phone PlatformkrajasekarantutiNo ratings yet
- Introduction To TelemedicineDocument25 pagesIntroduction To TelemedicineVaibhav SinhaNo ratings yet
- Low-Cost Central Monitor Based Personal Computer With Electrocardiogram and Heart Rate Parameters Via Wireless XBee ProDocument10 pagesLow-Cost Central Monitor Based Personal Computer With Electrocardiogram and Heart Rate Parameters Via Wireless XBee ProTELKOMNIKANo ratings yet
- Compressed Sensing Real-Time Energy-Eff Ecg Compression WBSN VandergheynstDocument11 pagesCompressed Sensing Real-Time Energy-Eff Ecg Compression WBSN VandergheynstAlex WongNo ratings yet
- Introduction to Telemedicine in 40 CharactersDocument26 pagesIntroduction to Telemedicine in 40 CharactersShane Bridges71% (7)
- Medical Electronics - SKP 174 197Document24 pagesMedical Electronics - SKP 174 197Mohammed Mian ANo ratings yet
- Survivable and Scalable Wireless Solution For E-Health and E-Emergency ApplicationsDocument5 pagesSurvivable and Scalable Wireless Solution For E-Health and E-Emergency ApplicationskeerthiNo ratings yet
- Paper 6Document7 pagesPaper 6RakeshconclaveNo ratings yet
- Internet of Things IoT Based Real Time VDocument22 pagesInternet of Things IoT Based Real Time VMd.Zesanul KabirNo ratings yet
- A Real Time Cardiac Arrhythmia Classification System With Wearable Sensor NetworksDocument27 pagesA Real Time Cardiac Arrhythmia Classification System With Wearable Sensor NetworksSubash S VersatileNo ratings yet
- A Wireless ECG Smart Sensor For Broad Application in Life Threatening Event DetectionDocument4 pagesA Wireless ECG Smart Sensor For Broad Application in Life Threatening Event DetectionDipin MutrejaNo ratings yet
- Deep Learning Algorithms for IoT-Assisted ECG MonitoringDocument9 pagesDeep Learning Algorithms for IoT-Assisted ECG MonitoringDaniel De MeloNo ratings yet
- Development of A Vital Sign Data Mining System For Chronic Patient MonitoringDocument6 pagesDevelopment of A Vital Sign Data Mining System For Chronic Patient MonitoringDanilo Rangel Arruda LeiteNo ratings yet
- Pulse Oximeter WirelessDocument6 pagesPulse Oximeter WirelessJeanCarlos Chavarría HughesNo ratings yet
- List of Marian ApparitionsDocument39 pagesList of Marian ApparitionsjonNo ratings yet
- Can The Dead RepentDocument6 pagesCan The Dead RepentjonNo ratings yet
- Sign of The CrossDocument18 pagesSign of The CrossjonNo ratings yet
- Accompanying Letter To Traditionis CustodesDocument11 pagesAccompanying Letter To Traditionis CustodesjonNo ratings yet
- 2021 Monstrance InfographicDocument1 page2021 Monstrance InfographicjonNo ratings yet
- Sara Blakely's Success Story: Starting Spanx with $5K and No ExperienceDocument4 pagesSara Blakely's Success Story: Starting Spanx with $5K and No ExperiencejonNo ratings yet
- Motu Proprio Traditionis CustodesDocument4 pagesMotu Proprio Traditionis CustodesjonNo ratings yet
- Warning and Various TopicsDocument32 pagesWarning and Various TopicsjonNo ratings yet
- Time Study Is The One Element in Scientific Management Beyond All Others Making Possible The Transfer of Skill From Management To Men ..Document15 pagesTime Study Is The One Element in Scientific Management Beyond All Others Making Possible The Transfer of Skill From Management To Men ..jonNo ratings yet
- Churchlifejournal - Nd.edu-Traditionis Custodes Was Never Merely About The LiturgyDocument14 pagesChurchlifejournal - Nd.edu-Traditionis Custodes Was Never Merely About The LiturgyjonNo ratings yet
- The Tale of Taylor and Gilbreth - How Lillian Gilbreth Resolved the Conflict Between Scientific Management PioneersDocument4 pagesThe Tale of Taylor and Gilbreth - How Lillian Gilbreth Resolved the Conflict Between Scientific Management PioneersjonNo ratings yet
- 04 - Civil Oil & GasDocument41 pages04 - Civil Oil & Gasjon100% (2)
- The Gilbreth NetworkDocument5 pagesThe Gilbreth NetworkjonNo ratings yet
- The Wellspring of Worship: Exploring the Connection Between Liturgy and LifeDocument35 pagesThe Wellspring of Worship: Exploring the Connection Between Liturgy and LifejonNo ratings yet
- Scientific ManagementDocument28 pagesScientific ManagementjonNo ratings yet
- History of Work OrganizationDocument20 pagesHistory of Work OrganizationjonNo ratings yet
- Lillian Moller GilbrethDocument7 pagesLillian Moller GilbrethjonNo ratings yet
- An Introduction To The Oil Industry - OPECDocument68 pagesAn Introduction To The Oil Industry - OPECTrần Hoàng ChươngNo ratings yet
- Frank Bunker Gilbreth - Britannica Online EncyclopediaDocument1 pageFrank Bunker Gilbreth - Britannica Online EncyclopediajonNo ratings yet
- Frank Bunker Gilbreth Sr. - WikipediaDocument4 pagesFrank Bunker Gilbreth Sr. - WikipediajonNo ratings yet
- The Wealth of Nations PDFDocument1,280 pagesThe Wealth of Nations PDFjonNo ratings yet
- "Pioneers of Industrial Engineering": Frank GilbrethDocument4 pages"Pioneers of Industrial Engineering": Frank GilbrethjonNo ratings yet
- 04 - Civil Oil & GasDocument41 pages04 - Civil Oil & Gasjon100% (2)
- Project Network Analysis TechniquesDocument22 pagesProject Network Analysis TechniquesjonNo ratings yet
- The Wealth of Nationz PDFDocument1,280 pagesThe Wealth of Nationz PDFjonNo ratings yet
- The Fall of The Philippines PDFDocument648 pagesThe Fall of The Philippines PDFjonNo ratings yet
- Ethics Dr. NicholasDocument28 pagesEthics Dr. Nicholasbuyinza NicholasNo ratings yet
- BULLDOZER - C52JSA-037 - Dozer Clearing of Existing Tracks in Jebel - 18-Mar-14Document6 pagesBULLDOZER - C52JSA-037 - Dozer Clearing of Existing Tracks in Jebel - 18-Mar-14hechame TamerhouletNo ratings yet
- Week10 Eth LMDocument8 pagesWeek10 Eth LMRenievave Torculas100% (2)
- Hazard InvestigationDocument2 pagesHazard InvestigationMichael KakulwaNo ratings yet
- 3 HOSPITAL ADMISSIONSDocument9 pages3 HOSPITAL ADMISSIONSVingky PakayaNo ratings yet
- Prueba 2Document188 pagesPrueba 2David LiNo ratings yet
- Nature of Conflict ExplainedDocument24 pagesNature of Conflict ExplainedJabrail AminNo ratings yet
- Aster RV Hospital BangloreDocument47 pagesAster RV Hospital BangloreAkhil Hb100% (1)
- Relationships Between Beliefs About Medications and AdherenceDocument8 pagesRelationships Between Beliefs About Medications and Adherencenoor cahayaNo ratings yet
- AL Ehsan Welfare Eye Hospital Volunteer ReportDocument21 pagesAL Ehsan Welfare Eye Hospital Volunteer ReportKaamla BajwaNo ratings yet
- CareHealth Policy 2020-21 Nihit FamilyDocument5 pagesCareHealth Policy 2020-21 Nihit FamilyJacob PruittNo ratings yet
- Firefighter Candidate Prep GuideDocument21 pagesFirefighter Candidate Prep GuideEric Levy100% (1)
- Balneological Use of Thermal WatersDocument10 pagesBalneological Use of Thermal WatersMary Carmen CarrascoNo ratings yet
- Chapter Quiz 1. MCNDocument4 pagesChapter Quiz 1. MCNAngie SaquingNo ratings yet
- Pembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyDocument11 pagesPembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyasdffdsaNo ratings yet
- "Nagsusuka Ang Anak Ko.": Nursing Care ProcessDocument2 pages"Nagsusuka Ang Anak Ko.": Nursing Care Processgeorgia50% (2)
- PCN Certification Services GuideDocument3 pagesPCN Certification Services Guidenarutothunderjet216No ratings yet
- Formfit: Digital Scale & Body AnalyzerDocument24 pagesFormfit: Digital Scale & Body Analyzerdon baileyNo ratings yet
- DC2020-0067 ICD-10 Code For COVID-19 (Previously Known As 2019-nCoV) (02-12-20)Document1 pageDC2020-0067 ICD-10 Code For COVID-19 (Previously Known As 2019-nCoV) (02-12-20)Leah Rose Figueroa ParasNo ratings yet
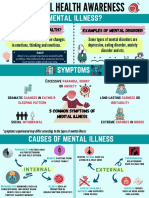
- Mental Health AwarenessDocument2 pagesMental Health Awarenessfarhatulhanimzulkifl100% (2)
- CEI Planet Winter 2021Document16 pagesCEI Planet Winter 2021CEINo ratings yet
- Case StudyDocument3 pagesCase StudyNovelyn B. PlaniaNo ratings yet
- Bonnie Patten Article - Self-RegulationDocument24 pagesBonnie Patten Article - Self-RegulationBill KeepNo ratings yet
- PHL Ad 17 01 Operationalguidance 2017 Eng Ops Manual Adolescent Health Development ProgramDocument111 pagesPHL Ad 17 01 Operationalguidance 2017 Eng Ops Manual Adolescent Health Development ProgramJoanne G Haw GetidaNo ratings yet
- Mapeh 10 Curriculum MapDocument9 pagesMapeh 10 Curriculum MapJoshua LamzonNo ratings yet
- Public Workshop #1 PresentationDocument28 pagesPublic Workshop #1 PresentationEllyn SantiagoNo ratings yet
- Healing Through LandscapeDocument28 pagesHealing Through LandscapeShinsha SaleemNo ratings yet
- CPS 2 ToxicologyDocument31 pagesCPS 2 ToxicologyNgọc Hà NguyễnNo ratings yet
- AnatomyDocument286 pagesAnatomyAbbyramy NNo ratings yet
- Poverty: The Worst Form of ViolenceDocument19 pagesPoverty: The Worst Form of Violencesraboni ahamedNo ratings yet