You might also like
- Research ArticleDocument6 pagesResearch ArticleCostin VrabieNo ratings yet
- The Adenoidal-Nasopharyngeal Ratio (A-N Ratio) - Its Validity in Selecting Children For AdenoidectomyDocument6 pagesThe Adenoidal-Nasopharyngeal Ratio (A-N Ratio) - Its Validity in Selecting Children For AdenoidectomyHana MitayaniNo ratings yet
- Adenoid Hypertrophy: A Correlation of Radiographic Parameters To Postoperative Adenoid VolumeDocument8 pagesAdenoid Hypertrophy: A Correlation of Radiographic Parameters To Postoperative Adenoid VolumeIJAR JOURNALNo ratings yet
- Angular Relationship Between Frankfort Horizontal Plane and Sella-Nasion Plane in Nepalese Orthodontic Patients: A Cephalometric StudyDocument4 pagesAngular Relationship Between Frankfort Horizontal Plane and Sella-Nasion Plane in Nepalese Orthodontic Patients: A Cephalometric StudysnehaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument5 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- C Craniocevical CT AJNR 07Document5 pagesC Craniocevical CT AJNR 07higorgbNo ratings yet
- X-Rays in The Evaluation of Adenoid Hypertrophy: It'S Role in The Endoscopic EraDocument3 pagesX-Rays in The Evaluation of Adenoid Hypertrophy: It'S Role in The Endoscopic EraDr.M.H. PatelNo ratings yet
- Una Propuesta de Distancia Esquelética Lineal para Predecir La Dimensión Vertical Oclusal Un Estudio CefalométricoDocument4 pagesUna Propuesta de Distancia Esquelética Lineal para Predecir La Dimensión Vertical Oclusal Un Estudio CefalométricoSamuel Flores CalderonNo ratings yet
- Description of The Sagittal Jaw Relation in CephalometricDocument7 pagesDescription of The Sagittal Jaw Relation in CephalometricBs PhuocNo ratings yet
- Relation Between Sagittal Position of The Mandible and Pharyngeal Airway Volume in Adults Using Cone Beam Computed TomographyDocument9 pagesRelation Between Sagittal Position of The Mandible and Pharyngeal Airway Volume in Adults Using Cone Beam Computed TomographyIJAR JOURNALNo ratings yet
- 339-Article Text-462-1-10-20190429Document3 pages339-Article Text-462-1-10-20190429emanNo ratings yet
- SILVER IndexDocument6 pagesSILVER IndexvistamaniacNo ratings yet
- Periapical Radiolucencies As Evaluated by Bisecting-Angle An PDFDocument9 pagesPeriapical Radiolucencies As Evaluated by Bisecting-Angle An PDFDiverse AnunturiNo ratings yet
- Maxillofacial Esthetics:: Anthropometrics of The Maxillofacial RegionDocument15 pagesMaxillofacial Esthetics:: Anthropometrics of The Maxillofacial RegionReem AltameemiNo ratings yet
- Lam 2001 Espacio Subar.Document5 pagesLam 2001 Espacio Subar.Jimmy Pino CoricazaNo ratings yet
- The Value of The Occipitomental Waters V PDFDocument5 pagesThe Value of The Occipitomental Waters V PDFItank Ichsan AmsNo ratings yet
- Key Factors in The Subjective and Objective Assessment of Conjunctival ErythemaDocument5 pagesKey Factors in The Subjective and Objective Assessment of Conjunctival ErythemaJack FruitNo ratings yet
- MBE Down SyndromeDocument7 pagesMBE Down SyndromeMaría Camila Villarreal AlejoNo ratings yet
- 44 QuestionsDocument9 pages44 QuestionsElla GolikNo ratings yet
- Pone 0090412Document6 pagesPone 0090412Ratih Kusuma DewiNo ratings yet
- Detection of The Mandibular Canal and The Mental Foramen in Panoramic Radiographs: Intraexaminer AgreementDocument5 pagesDetection of The Mandibular Canal and The Mental Foramen in Panoramic Radiographs: Intraexaminer AgreementDragos CiongaruNo ratings yet
- Measurement of Angle KappaDocument5 pagesMeasurement of Angle Kappapason1988100% (1)
- Atlas c1Document5 pagesAtlas c1davorribicicNo ratings yet
- Equiterio 2021Document6 pagesEquiterio 2021ppdsretinaNo ratings yet
- Brereton 2019Document9 pagesBrereton 2019juan pablo aguirreNo ratings yet
- Clinical Score Adenoid Hypertrophy PDFDocument7 pagesClinical Score Adenoid Hypertrophy PDFjoniindahsariNo ratings yet
- Agreement Between Panoramic and Intra-Oral Radiography in The Assessment of Marginal Bone HeightDocument6 pagesAgreement Between Panoramic and Intra-Oral Radiography in The Assessment of Marginal Bone HeightDorin N. GheorgheNo ratings yet
- Cus Normograms 2008 Indian StudyDocument7 pagesCus Normograms 2008 Indian StudySatvik BansalNo ratings yet
- WJ 6 CD9 WN KWZP SR FCxymr KVRDocument6 pagesWJ 6 CD9 WN KWZP SR FCxymr KVRaaliagaqNo ratings yet
- 1548-1336 (2004) 030 0002:daocai 2.0.co 2Document5 pages1548-1336 (2004) 030 0002:daocai 2.0.co 2Dragos CiongaruNo ratings yet
- 2013 - BoghaniDocument11 pages2013 - Boghanialejandra gonzalezNo ratings yet
- Cephalometric Evaluation of Adenoids An Analysis of Current Methods and A Proposal of A New Assessment ToolDocument8 pagesCephalometric Evaluation of Adenoids An Analysis of Current Methods and A Proposal of A New Assessment ToolDr.Prakher SainiNo ratings yet
- CefalometriaDocument8 pagesCefalometriaMartin ValdezNo ratings yet
- Cephalometrics For Orthognathic SurgeryDocument11 pagesCephalometrics For Orthognathic SurgeryGowri ShankarNo ratings yet
- Comparison of Common Hard Tissue Cephalometric Measurements Between Computed Tomography 3D Reconstruction and Conventional 2D Cephalometric ImagesDocument6 pagesComparison of Common Hard Tissue Cephalometric Measurements Between Computed Tomography 3D Reconstruction and Conventional 2D Cephalometric ImagesAndré Louiz FerreiraNo ratings yet
- Admin, 5Document6 pagesAdmin, 5emanNo ratings yet
- Radiotherapy and OncologyDocument8 pagesRadiotherapy and OncologyÁgnes ZongorNo ratings yet
- DX de Neumotorax Por RX Torax Vs USG Chest 2011Document8 pagesDX de Neumotorax Por RX Torax Vs USG Chest 2011Karla Rosales MoralesNo ratings yet
- A Modified Steiners Analysis That Does Not RequirDocument8 pagesA Modified Steiners Analysis That Does Not RequirKanchit SuwanswadNo ratings yet
- Branski2002 PDFDocument6 pagesBranski2002 PDFlakjdlkaNo ratings yet
- Correlation Between Objective and Subjective Assessment of Nasal PatencyDocument7 pagesCorrelation Between Objective and Subjective Assessment of Nasal PatencyJulita MelisaNo ratings yet
- The Denture Frame Analysis: An Additional Diagnostic ToolDocument9 pagesThe Denture Frame Analysis: An Additional Diagnostic ToolMirek SzNo ratings yet
- An Evaluation of Condyle Position in Centric RelationDocument4 pagesAn Evaluation of Condyle Position in Centric RelationAlejandra LorancaNo ratings yet
- A Plane of Orientation With An Extracranial AnteriorDocument5 pagesA Plane of Orientation With An Extracranial AnteriorkerolossalahNo ratings yet
- Of Mandibular Condylar Positi Ntal Occlusion Factors in An Somatic PopulationDocument7 pagesOf Mandibular Condylar Positi Ntal Occlusion Factors in An Somatic PopulationDanilo BorjaNo ratings yet
- A Beginners Guide To Lateral Cephalometric RadiographsDocument4 pagesA Beginners Guide To Lateral Cephalometric RadiographsClaudiaNo ratings yet
- Centrographic Analysis of 1-Phase Versus 2-Phase Treatment For Class II MalocclusionDocument6 pagesCentrographic Analysis of 1-Phase Versus 2-Phase Treatment For Class II MalocclusionnomanNo ratings yet
- Assessment of Sagittal Discrepancies of JawsDocument6 pagesAssessment of Sagittal Discrepancies of JawsFourthMolar.comNo ratings yet
- Nervo FacialDocument5 pagesNervo FacialCarlinhosdadeep DeepWebNo ratings yet
- Duncan Boyton 2003Document13 pagesDuncan Boyton 2003KN ThianNo ratings yet
- Value of Acoustic Rhinometry For Measuring Nasal Valve AreaDocument8 pagesValue of Acoustic Rhinometry For Measuring Nasal Valve AreaKishorePrabakaranKumarNo ratings yet
- E148 FullDocument4 pagesE148 FullFadel WidePutraNo ratings yet
- BiometryDocument7 pagesBiometrysandip shelakeNo ratings yet
- Lundstrom 1995Document10 pagesLundstrom 1995Magu LaraNo ratings yet
- Analysis of The Ear Pulse Oximeter Wavef PDFDocument10 pagesAnalysis of The Ear Pulse Oximeter Wavef PDFmuhammad lutfiNo ratings yet
- Computed Tomography Versus Nasal Endoscopy For The Measurement of The Internal Nasal Valve Angle in AsiansDocument5 pagesComputed Tomography Versus Nasal Endoscopy For The Measurement of The Internal Nasal Valve Angle in AsiansPutri HakimNo ratings yet
- (Doi 10.1043 - 0003-3219 (2006) 076 (0388 - VOPRFM) 2.0.CO 2)Document6 pages(Doi 10.1043 - 0003-3219 (2006) 076 (0388 - VOPRFM) 2.0.CO 2)Bulfendri DoniNo ratings yet
- Levitan2003 2Document9 pagesLevitan2003 2carlosNo ratings yet
- Diagnostic Utility of Optic Nerve Measurements With MRI in Patients With Optic Nerve AtrophyDocument4 pagesDiagnostic Utility of Optic Nerve Measurements With MRI in Patients With Optic Nerve AtrophyGarsa GarnolNo ratings yet
- Correlational ResearchDocument10 pagesCorrelational ResearchSari100% (1)
- Three Way Conference Template 2019Document4 pagesThree Way Conference Template 2019api-313701922No ratings yet
- Bacterial ClassificationDocument2 pagesBacterial ClassificationAndrew JavierNo ratings yet
- LoadRunner BasicsDocument74 pagesLoadRunner BasicsmadhugangulaNo ratings yet
- Given Values: Pressure Temperature Compressor Inlet 1.0325 Bar 300K Turbine Outlet 1.0325 Bar 815K Pressure Ratio 18.6Document3 pagesGiven Values: Pressure Temperature Compressor Inlet 1.0325 Bar 300K Turbine Outlet 1.0325 Bar 815K Pressure Ratio 18.6Walter BircherNo ratings yet
- Fatty Acid SynthesisDocument28 pagesFatty Acid Synthesishassanainshahi13No ratings yet
- Jain 2018Document10 pagesJain 2018Pablo Ignacio Contreras EstradaNo ratings yet
- Lerdge-Gcode List V3.0.5Document108 pagesLerdge-Gcode List V3.0.5osman perez vidalNo ratings yet
- Assigment Sheet Tast 2 Aina MardianaDocument10 pagesAssigment Sheet Tast 2 Aina MardianaAina MardianaNo ratings yet
- Dilution CalculationsDocument2 pagesDilution CalculationsDeden Putra BabakanNo ratings yet
- ReportDocument1 pageReportDrew DacanayNo ratings yet
- 33 KV Transmission Line Design Drawings PDFDocument265 pages33 KV Transmission Line Design Drawings PDFkapilsharma404No ratings yet
- Muhammad Ajmal Farooqi: Chemical EngineerDocument4 pagesMuhammad Ajmal Farooqi: Chemical EngineeromercomsatNo ratings yet
- EECS4421Z: Introduction To Robotics Sample Exam QuestionsDocument7 pagesEECS4421Z: Introduction To Robotics Sample Exam QuestionsMooeez BellaamineNo ratings yet
- Lista Ejercicios 3 PPEDocument25 pagesLista Ejercicios 3 PPEKarla HermorNo ratings yet
- Studyprotocol Open Access: Yue Yan, Yalin Zhan, Xian 'E Wang and Jianxia HouDocument7 pagesStudyprotocol Open Access: Yue Yan, Yalin Zhan, Xian 'E Wang and Jianxia HouGery KrismawanNo ratings yet
- Unit No 1Document64 pagesUnit No 1Aadil VahoraNo ratings yet
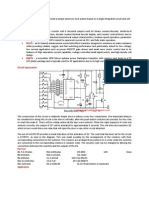
- Electronic Door LockDocument2 pagesElectronic Door LocktaindiNo ratings yet
- ANFISDocument19 pagesANFISShimaa Barakat100% (1)
- 638 - Servoregler Technical - ManualDocument123 pages638 - Servoregler Technical - ManualemfiNo ratings yet
- 3) Production SchedulingDocument26 pages3) Production SchedulingJhon Ace DuricoNo ratings yet
- 02a-2 V-Can2 Xlrteh4300g033850Document1 page02a-2 V-Can2 Xlrteh4300g033850Daniel PricopNo ratings yet
- Product Data Sheet: Control Unit Micrologic 5.0 A, For Masterpact NT/ NW, LSI ProtectionsDocument3 pagesProduct Data Sheet: Control Unit Micrologic 5.0 A, For Masterpact NT/ NW, LSI ProtectionsEvandro PavesiNo ratings yet
- EEMDocument17 pagesEEMSandaruwan සුජීවNo ratings yet
- 24 BitcoinDocument36 pages24 Bitcoind0c0ngthanhNo ratings yet
- IMMUNOHISTOCHEMDocument7 pagesIMMUNOHISTOCHEMJadys Merill DiezNo ratings yet
- Asme Se-165 2004Document25 pagesAsme Se-165 2004Kamalnath KpNo ratings yet
- Determinants of Profitability Performance: An Analysis of Class I Railroads in The United StatesDocument18 pagesDeterminants of Profitability Performance: An Analysis of Class I Railroads in The United StatesJayaniNo ratings yet
- DDP400 Open-Frame and U-Chassis :: ROAL Living EnergyDocument12 pagesDDP400 Open-Frame and U-Chassis :: ROAL Living EnergyroalscribdNo ratings yet
- Drill Pipe Drill StringDocument11 pagesDrill Pipe Drill StringRodrigoBernardo50% (2)