You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Completely Edentulous Mandible: Treatment Plans For Fixed RestorationsDocument15 pagesThe Completely Edentulous Mandible: Treatment Plans For Fixed Restorationswaf51No ratings yet
- Smt1 Optics Lens and Human EyeDocument2 pagesSmt1 Optics Lens and Human EyeRoan Tapia AntiquenoNo ratings yet
- 3DPrinted Materials For Permanent Restorations in IndirectDocument19 pages3DPrinted Materials For Permanent Restorations in Indirectwaf51No ratings yet
- Accuracy and Reliability of Intraoral Scanners: Are They The Better Option?Document9 pagesAccuracy and Reliability of Intraoral Scanners: Are They The Better Option?waf51No ratings yet
- 2016COIR DigitalvsconventionalimpressionDocument9 pages2016COIR Digitalvsconventionalimpressionwaf51No ratings yet
- 1 s2.0 S277255962200013X MainDocument10 pages1 s2.0 S277255962200013X Mainwaf51No ratings yet
- 1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2Document10 pages1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2waf51No ratings yet
- 65 - JPOR - 2019 - 356 EnciaDocument8 pages65 - JPOR - 2019 - 356 Enciawaf51No ratings yet
- Residual Ridge ResorptionDocument38 pagesResidual Ridge Resorptionwaf51No ratings yet
- TARLOWimplantstentarticleDocument3 pagesTARLOWimplantstentarticlewaf51No ratings yet
- A Review of The Recent Literature On Maxillary Overdenture With Dental ImplantsDocument5 pagesA Review of The Recent Literature On Maxillary Overdenture With Dental Implantswaf51No ratings yet
- ATWOODDocument15 pagesATWOODwaf51No ratings yet
- Use of Diagnostic and Surgical Stent A SimplifiedDocument7 pagesUse of Diagnostic and Surgical Stent A Simplifiedwaf51No ratings yet
- Implant Surgical Guides From The Past To The PresentDocument6 pagesImplant Surgical Guides From The Past To The Presentwaf51No ratings yet
- 3D Printing Guide Implant Placement A Case ReportDocument5 pages3D Printing Guide Implant Placement A Case Reportwaf51No ratings yet
- The Third Point of Reference and Its EffDocument7 pagesThe Third Point of Reference and Its Effwaf51No ratings yet
- Evaluation of Two Facebow/Semi-adjustable Articulator Systems For Orienting Maxillary Cast On Articulators: A Pilot StudyDocument5 pagesEvaluation of Two Facebow/Semi-adjustable Articulator Systems For Orienting Maxillary Cast On Articulators: A Pilot Studywaf51No ratings yet
- Philosophy and Physics of Mandibular Hinge Axis: A Review: International Journal of Scientific Research April 2014Document3 pagesPhilosophy and Physics of Mandibular Hinge Axis: A Review: International Journal of Scientific Research April 2014waf51No ratings yet
- ANTERIORPOINTOFREFERENCEDocument6 pagesANTERIORPOINTOFREFERENCEwaf51No ratings yet
- 補 綴 誌,J Jpn Prosthodont Soc, 31: 1405∼1412, 1987Document8 pages補 綴 誌,J Jpn Prosthodont Soc, 31: 1405∼1412, 1987waf51No ratings yet
- Textbook of Prosthodontics PDFDriveDocument864 pagesTextbook of Prosthodontics PDFDrivewaf51No ratings yet
- Effect of Joint Surface Contours On The Transverse and Impactstrength of Denture Base Resin Repaired by Various Methods. An Invitro StudyDocument12 pagesEffect of Joint Surface Contours On The Transverse and Impactstrength of Denture Base Resin Repaired by Various Methods. An Invitro Studywaf51No ratings yet
- Maxillary Immediate Denture: A Case Report: International Journal of Medical and Health ResearchDocument3 pagesMaxillary Immediate Denture: A Case Report: International Journal of Medical and Health Researchwaf51No ratings yet
- CNS TumorDocument32 pagesCNS TumorBbem ooNo ratings yet
- UntitledDocument10 pagesUntitledMashkat AbdelwahabNo ratings yet
- Anterior Rhinoscopy-Hanan BakriDocument15 pagesAnterior Rhinoscopy-Hanan BakriMadalina DutanNo ratings yet
- 333 566 1 PBDocument6 pages333 566 1 PBSaud JafarNo ratings yet
- Anatomo-Physiologic Basis For Auricular StimulationDocument10 pagesAnatomo-Physiologic Basis For Auricular StimulationMiki ShimizuNo ratings yet
- HISTOLOGY Tongue and OsephagusDocument8 pagesHISTOLOGY Tongue and OsephagusAkachukwu ObunikeNo ratings yet
- Cephalometric SentDocument17 pagesCephalometric SentMuhammad NiyalishNo ratings yet
- Bone Regeneration in ImplantologyDocument348 pagesBone Regeneration in ImplantologyThanh Nhan DinhNo ratings yet
- Lower Blepharoplasty: Transconjunctival Fat Repositioning: Facialplastic Surgeryclinics OfnorthamericaDocument7 pagesLower Blepharoplasty: Transconjunctival Fat Repositioning: Facialplastic Surgeryclinics OfnorthamericaBFF BotoxNo ratings yet
- Performing Facial TreatmentDocument48 pagesPerforming Facial TreatmentAngela Mae Gratija100% (1)
- Giai Phau Mach Mau NaoDocument40 pagesGiai Phau Mach Mau NaoHoàng Bùi TháiNo ratings yet
- Juxtacortical Lesions and Cortical Thinning in Multiple SclerosisDocument7 pagesJuxtacortical Lesions and Cortical Thinning in Multiple SclerosishelenNo ratings yet
- Human BrainDocument44 pagesHuman BrainSri vaishnava100% (1)
- English Vocabulary: Parts of Your BodyDocument6 pagesEnglish Vocabulary: Parts of Your BodyCarmen Elena CarteșNo ratings yet
- Brain Structure and FunctionDocument5 pagesBrain Structure and Functionmademoiselle in transitNo ratings yet
- Tooth Supported OverdenturesDocument5 pagesTooth Supported OverdenturesStudy RoomNo ratings yet
- Zygomatico-Maxillary OsteotomyDocument8 pagesZygomatico-Maxillary Osteotomypratiksha malhotraNo ratings yet
- Ent History Taking and Examination-1Document16 pagesEnt History Taking and Examination-1Jyotirmayee100% (5)
- اسئلة تراما سابقةDocument15 pagesاسئلة تراما سابقةمروه صفاء رحيم حسنNo ratings yet
- Woodward,: 2. A. SmithDocument26 pagesWoodward,: 2. A. SmithFabio PicassoNo ratings yet
- Williams & Gowans 2003Document4 pagesWilliams & Gowans 2003Eryson Thiago PradoNo ratings yet
- القيادة الاداريةDocument73 pagesالقيادة الاداريةosamaNo ratings yet
- IntegumentaryDocument67 pagesIntegumentaryKz ParasNo ratings yet
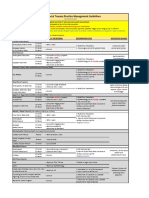
- VUMC Facial Trauma Practice Management GuidelinesDocument1 pageVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNo ratings yet
- Imaging ATMDocument27 pagesImaging ATM4gxwkppybdNo ratings yet
- Parts of The Nose and SkinDocument18 pagesParts of The Nose and SkinMarielle BarredoNo ratings yet
- Oral Surgery 2 Prelims 1Document27 pagesOral Surgery 2 Prelims 1Ken HoiNo ratings yet
- DR B. Neuroanatomy BookDocument134 pagesDR B. Neuroanatomy BookMURESAN MARIANo ratings yet
- Endo Set 2 QuestionsDocument7 pagesEndo Set 2 QuestionsBinayak UpadhyayaNo ratings yet