You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ashton Manual English PDFDocument58 pagesAshton Manual English PDFMalissa Bowen100% (2)
- NAC Protocol PrintableDocument21 pagesNAC Protocol Printablemaadyyy123100% (1)
- Nervous SystemDocument40 pagesNervous SystemNabeel Uddin100% (1)
- ABG Interpretation - ATSDocument5 pagesABG Interpretation - ATSHAMMYER ALROKHAMINo ratings yet
- CC, HPV & HPV VaccineDocument16 pagesCC, HPV & HPV VaccineBalqis BaslemanNo ratings yet
- RCDSO Guidelines Implant Dentistry PDFDocument16 pagesRCDSO Guidelines Implant Dentistry PDFl4j0b9No ratings yet
- Equipment Devices and Procedures in The Intensive Care Unit PDFDocument16 pagesEquipment Devices and Procedures in The Intensive Care Unit PDFJena Rose ReyesNo ratings yet
- Sublingual vs. Oral Captopril in Hypertensive CrisisDocument18 pagesSublingual vs. Oral Captopril in Hypertensive Crisisgrace liwantoNo ratings yet
- Postpartum Depression and Its Risk Factors in Women With A Potentially Lifethreatening ComplicationDocument18 pagesPostpartum Depression and Its Risk Factors in Women With A Potentially Lifethreatening Complicationgrace liwantoNo ratings yet
- COVID-19 Vaccine Acceptance in Pregnant WomenDocument6 pagesCOVID-19 Vaccine Acceptance in Pregnant Womengrace liwantoNo ratings yet
- Double Foley Catheter For Labor Induction - An Alternative MethodDocument9 pagesDouble Foley Catheter For Labor Induction - An Alternative Methodgrace liwantoNo ratings yet
- Jurnal 2Document16 pagesJurnal 2grace liwantoNo ratings yet
- Systematic Review Gastrointestinal Infection and IncidentDocument11 pagesSystematic Review Gastrointestinal Infection and Incidentgrace liwantoNo ratings yet
- Clinical Characteristics of COVID-19 PatientsDocument8 pagesClinical Characteristics of COVID-19 Patientsgrace liwantoNo ratings yet
- The Human EyeDocument33 pagesThe Human Eyegrace liwantoNo ratings yet
- Clinical, Microbiological, and Imaging Characteristics of InfectiveDocument10 pagesClinical, Microbiological, and Imaging Characteristics of Infectivegrace liwantoNo ratings yet
- COVID-19 Vaccination in PregnancyDocument12 pagesCOVID-19 Vaccination in Pregnancygrace liwantoNo ratings yet
- Asymptomatic SARS CoV2 InfectionDocument12 pagesAsymptomatic SARS CoV2 Infectiongrace liwantoNo ratings yet
- Pemicu 1 GI GraceDocument146 pagesPemicu 1 GI Gracegrace liwantoNo ratings yet
- Pterygium Excision and Conjunctival AutograftDocument13 pagesPterygium Excision and Conjunctival Autograftgrace liwantoNo ratings yet
- Alimentary TractDocument8 pagesAlimentary Tractgrace liwantoNo ratings yet
- Radiologi Modul Respirasi 2016Document123 pagesRadiologi Modul Respirasi 2016grace liwantoNo ratings yet
- Lung Diseases Lydia Tantoso, MD, INTERNISTDocument28 pagesLung Diseases Lydia Tantoso, MD, INTERNISTgrace liwantoNo ratings yet
- Fisio RespirasiDocument114 pagesFisio Respirasigrace liwantoNo ratings yet
- Colorectal CarcinomaDocument18 pagesColorectal Carcinomagrace liwantoNo ratings yet
- RCT Lactobacillus Reuteri in Chronic ConstipationDocument6 pagesRCT Lactobacillus Reuteri in Chronic Constipationgrace liwantoNo ratings yet
- 11 Benefits of Breastfeeding For Both Mom and BabyDocument15 pages11 Benefits of Breastfeeding For Both Mom and BabySubhranil MaityNo ratings yet
- 2 Jaundice in The NBDocument33 pages2 Jaundice in The NBCheru DugaseNo ratings yet
- BMJ Avian FluDocument49 pagesBMJ Avian Flualiakbar178No ratings yet
- US BTC FAQ 2015 Updated 1-5-16Document21 pagesUS BTC FAQ 2015 Updated 1-5-16Seau Vin NeeNo ratings yet
- Outscraper 2024020607591330fd Obstetrician Gynecologist +3Document265 pagesOutscraper 2024020607591330fd Obstetrician Gynecologist +3sanjulata.agriNo ratings yet
- Care For Client With Oxygenation Problem: OutcomesDocument19 pagesCare For Client With Oxygenation Problem: OutcomesPaul JacksonNo ratings yet
- Lithotripsy Salivary Stones OhpDocument5 pagesLithotripsy Salivary Stones Ohpaysha mksNo ratings yet
- Adequacy of PerfusionDocument11 pagesAdequacy of PerfusionLaiba SiddiqueNo ratings yet
- Canine Distemper: Hard Pad Disease, Canine InfluenzaDocument11 pagesCanine Distemper: Hard Pad Disease, Canine InfluenzaDr-Hassan SaeedNo ratings yet
- A 5-Year Observation of The Dahl Principle To Manage Localized Anterior Tooth WearDocument5 pagesA 5-Year Observation of The Dahl Principle To Manage Localized Anterior Tooth WearMohammad Abdulmon’emNo ratings yet
- Blood Pressure 911Document7 pagesBlood Pressure 911Judith J. LaneNo ratings yet
- Lecture NotesDocument61 pagesLecture NotesTom Anthony Tonguia100% (1)
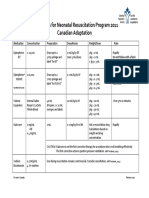
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- 3 Q Epidemiology Part 1Document26 pages3 Q Epidemiology Part 1Prince GoelNo ratings yet
- ATI Flash Cards 03, Medications Affecting Immune SystemDocument40 pagesATI Flash Cards 03, Medications Affecting Immune Systemensoooooooooo0% (1)
- Breastcrawl PDFDocument41 pagesBreastcrawl PDFFayrouz EssawiNo ratings yet
- ObjectiveDocument2 pagesObjectiveMarvinNo ratings yet
- Cellulitis - Acute - NICE CKS PDFDocument40 pagesCellulitis - Acute - NICE CKS PDFDinu IuliaNo ratings yet
- Myotonic DiseaseDocument11 pagesMyotonic DiseaseOhlee TanNo ratings yet
- Family Nursing Care Plan SeizuresDocument3 pagesFamily Nursing Care Plan SeizuresClaire AlcantaraNo ratings yet
- Philippine Dental Association Covid 19 Monitoring FormDocument1 pagePhilippine Dental Association Covid 19 Monitoring Formrhusolano rhusolanoNo ratings yet
- Early and Late Preeclamsia Are Characterized by High Cardiac Output, But in The Presence of Fetal Growth Restriction, Cardiac Output Is Low Insights From A Prospective Study PDFDocument12 pagesEarly and Late Preeclamsia Are Characterized by High Cardiac Output, But in The Presence of Fetal Growth Restriction, Cardiac Output Is Low Insights From A Prospective Study PDFJustiawan NazwanNo ratings yet