You might also like
- Boies Text PDFDocument568 pagesBoies Text PDFKJ100% (3)
- Method Statement For PlasteringDocument14 pagesMethod Statement For Plasteringjameel100% (1)
- CBR Team Rehabilitation PresentationDocument21 pagesCBR Team Rehabilitation PresentationAzharul Islam ArjuNo ratings yet
- Rehabilitation NursingDocument62 pagesRehabilitation NursingKailash Nagar100% (1)
- REHABILITATION TEAMDocument4 pagesREHABILITATION TEAMDominion OgochukwuNo ratings yet
- Medsurg Rosales Part 1 and 2Document10 pagesMedsurg Rosales Part 1 and 2fiel borataNo ratings yet
- PTJ 1177Document11 pagesPTJ 1177phyterapistNo ratings yet
- Funda Notes1Document8 pagesFunda Notes1Veronica ShaneNo ratings yet
- The Patient RosalesDocument29 pagesThe Patient Rosalesfiel borataNo ratings yet
- Rle Lesson 3 Comprehensive Geriatric AssessmentDocument9 pagesRle Lesson 3 Comprehensive Geriatric AssessmentRoselyn Yu QuintoNo ratings yet
- Intro 2rehabilitationDocument25 pagesIntro 2rehabilitationSajida Bibi NoonariNo ratings yet
- The Concept of RehabilitationDocument22 pagesThe Concept of RehabilitationOdulio, Loise Danielle T.No ratings yet
- Nursing Care of Disable PeopleDocument40 pagesNursing Care of Disable PeoplePraZeeTaPuriNo ratings yet
- OT and Eating DysfunctionDocument1 pageOT and Eating DysfunctionMCris EsSemNo ratings yet
- Presentation FinalDocument7 pagesPresentation FinalCamille De La RosaNo ratings yet
- Introducton To Rehabilitation: DR: Sajida Bibi Noonari Lecturer at NiprmDocument12 pagesIntroducton To Rehabilitation: DR: Sajida Bibi Noonari Lecturer at NiprmsajidaNo ratings yet
- TFN Theorist Table Martin Andrea Bsn1y110Document12 pagesTFN Theorist Table Martin Andrea Bsn1y110Kyla Mae ZabalaNo ratings yet
- NCM 103 NotesDocument26 pagesNCM 103 NotesJohannaNo ratings yet
- Week 14 LEC Interdisciplinary Mental Health Team Collaboration BAUTISTADocument51 pagesWeek 14 LEC Interdisciplinary Mental Health Team Collaboration BAUTISTAAngelica GatdulaNo ratings yet
- Create A Graphic Organizer About Range of Special Education Programs Services and Support Services For Children With Special NeedsDocument3 pagesCreate A Graphic Organizer About Range of Special Education Programs Services and Support Services For Children With Special NeedsNeliza SalcedoNo ratings yet
- Nursing Care Plan for a Patient with Impaired Physical MobilityDocument2 pagesNursing Care Plan for a Patient with Impaired Physical MobilityROGEN KATE AZARCONNo ratings yet
- The Rehabiliation Team 2Document19 pagesThe Rehabiliation Team 2Jica Gula100% (1)
- What Is Rehabilitation Medicine? ImpairmentDocument2 pagesWhat Is Rehabilitation Medicine? Impairmentchenelyn_15No ratings yet
- Medical Rehabilitation for Arthritis PatientsDocument13 pagesMedical Rehabilitation for Arthritis PatientsRalph AlbertoNo ratings yet
- International Encyclopedia of RehabilitationDocument16 pagesInternational Encyclopedia of Rehabilitationshiela badiangNo ratings yet
- Disability and RehabilitationDocument40 pagesDisability and RehabilitationAbhishek Verma100% (1)
- HandoutDocument6 pagesHandoutKimberly EscalanteNo ratings yet
- RehabilitationDocument43 pagesRehabilitationDaniel CoxNo ratings yet
- Essay: 1. Definition and Philosophy of Rehabilitation Re Means Return Habilitation Means AbilityDocument17 pagesEssay: 1. Definition and Philosophy of Rehabilitation Re Means Return Habilitation Means Abilityfarid akbar100% (1)
- Geriatric Care TeamDocument2 pagesGeriatric Care TeamAveryNo ratings yet
- Henderson PDFDocument11 pagesHenderson PDFNicole SilorioNo ratings yet
- Compiled PPT - CompressedDocument56 pagesCompiled PPT - CompressedAnchal SinghNo ratings yet
- Ot 1Document4 pagesOt 1secret101No ratings yet
- Geriatrics - Geriatrics Health Care TeamDocument2 pagesGeriatrics - Geriatrics Health Care TeamBSN 1-N CASTRO, RicciNo ratings yet
- Activity 7 Care of Older PersonDocument2 pagesActivity 7 Care of Older PersonRachelNo ratings yet
- 13 Neonatal Fact SheetDocument4 pages13 Neonatal Fact SheetWalaa EldesoukeyNo ratings yet
- Nursing As A Profession M2CanvasDocument27 pagesNursing As A Profession M2Canvasilpicache8209valNo ratings yet
- Care of Elderly Patients: Role of NursesDocument2 pagesCare of Elderly Patients: Role of Nursespatel h100% (1)
- Rehabilitation of Health CareDocument95 pagesRehabilitation of Health CareAlm3iglyNo ratings yet
- C CEF Roles, Character, Team PlainDocument10 pagesC CEF Roles, Character, Team PlainConrad C. CatimbangNo ratings yet
- Health 1Document5 pagesHealth 1maxNo ratings yet
- Problem and It'S Background: Senior Centers Are AnDocument44 pagesProblem and It'S Background: Senior Centers Are Anrosencrantz_05No ratings yet
- Inbound 3882788338272933428Document6 pagesInbound 3882788338272933428nene.marylouise22No ratings yet
- ICF SwallowingDocument2 pagesICF SwallowingMarcela Sanhueza GarridoNo ratings yet
- End of LifeDocument17 pagesEnd of Lifeliz diazNo ratings yet
- RT 114 - Multidisciplinary Team ApproachDocument3 pagesRT 114 - Multidisciplinary Team ApproachCharisa Antonette HuelvaNo ratings yet
- Incussive Chap 1&2Document25 pagesIncussive Chap 1&2Tolesa MegersaNo ratings yet
- Assess mental status with this psychiatric nursing MSE guideDocument4 pagesAssess mental status with this psychiatric nursing MSE guideChien Lai R. BontuyanNo ratings yet
- The Roles of Occupational Therapy, Physical Therapy, and Speech/Language Pathology in Primary CareDocument8 pagesThe Roles of Occupational Therapy, Physical Therapy, and Speech/Language Pathology in Primary CarecpNo ratings yet
- Selected Local Nursing Theories andDocument2 pagesSelected Local Nursing Theories andBaisigried SechongNo ratings yet
- Traumatic Brain Injury PhysiotherapyDocument22 pagesTraumatic Brain Injury Physiotherapydarshika.vyasNo ratings yet
- Swallowing Swallowing: Person-Centered Focus On Function: Person-Centered Focus On FunctionDocument2 pagesSwallowing Swallowing: Person-Centered Focus On Function: Person-Centered Focus On FunctionGabriel MoralesNo ratings yet
- Funda Lesson3 Health Care Delivery SystemDocument3 pagesFunda Lesson3 Health Care Delivery SystemAzTech 233No ratings yet
- Activity 2Document3 pagesActivity 2Neliza SalcedoNo ratings yet
- Nursing: An Art and A Science: "Nutricius" - That Nourishes, Fosters and ProtectsDocument3 pagesNursing: An Art and A Science: "Nutricius" - That Nourishes, Fosters and ProtectsMykristie Jho B. MendezNo ratings yet
- Team Work in Palliative Care: Ns. Endah Panca Lydia F, MkepDocument15 pagesTeam Work in Palliative Care: Ns. Endah Panca Lydia F, Mkepyana suryanaNo ratings yet
- ABallesteros PeerSupportPoster 2023Document1 pageABallesteros PeerSupportPoster 2023stqcvdfq8dNo ratings yet
- Ms 7 Principles and Practices of Rehabilitation 1Document119 pagesMs 7 Principles and Practices of Rehabilitation 1Griethel MaireNo ratings yet
- 1 Introduction To Mental Health and Psychiatric NursingDocument6 pages1 Introduction To Mental Health and Psychiatric NursingRose Lyn Camarista VelascoNo ratings yet
- General Principles and Empirically Supported Techniques of Cognitive Behavior TherapyFrom EverandGeneral Principles and Empirically Supported Techniques of Cognitive Behavior TherapyNo ratings yet
- Parenting Neurodiverse Children: A Comprehensive Guide to Supporting Children with ADHD, Autism, and DyslexiaFrom EverandParenting Neurodiverse Children: A Comprehensive Guide to Supporting Children with ADHD, Autism, and DyslexiaNo ratings yet
- 1.1 Intro To Med JurisDocument3 pages1.1 Intro To Med JurisMary PropertiesNo ratings yet
- (Medjur) Intro To Medical JurisprudenceDocument2 pages(Medjur) Intro To Medical JurisprudenceMary PropertiesNo ratings yet
- Module 2 Lecture Notes on Deception Detection TechniquesDocument6 pagesModule 2 Lecture Notes on Deception Detection TechniquesMary PropertiesNo ratings yet
- Module 1 - LEGAL MEDDocument9 pagesModule 1 - LEGAL MEDMary PropertiesNo ratings yet
- Poster Clinical Investigation of Magic Ring (Modified Plastibell Device) For CircumcisionDocument1 pagePoster Clinical Investigation of Magic Ring (Modified Plastibell Device) For CircumcisionLutfi Aulia RahmanNo ratings yet
- Good WSH Practices Pictograms: Guide ToDocument7 pagesGood WSH Practices Pictograms: Guide Tobob juanNo ratings yet
- La Fortuna Nhs GPB 2022Document50 pagesLa Fortuna Nhs GPB 2022Jesselly ValesNo ratings yet
- Accomplishment Report: Municipality of NarvacanDocument3 pagesAccomplishment Report: Municipality of Narvacanuser computerNo ratings yet
- Cozen ResumeDocument3 pagesCozen Resumeapi-534216481No ratings yet
- Calderon 2022Document9 pagesCalderon 2022Roger CalderonNo ratings yet
- HirsutismDocument10 pagesHirsutismMarielle VentulaNo ratings yet
- Understanding Culture, Society and Politics: Quarter 4 - Module 11: Social InequalitiesDocument12 pagesUnderstanding Culture, Society and Politics: Quarter 4 - Module 11: Social InequalitiesBEBERLIE GALOS100% (4)
- Rare Case of Sirenomelia Congenital AnomalyDocument3 pagesRare Case of Sirenomelia Congenital Anomalymahesh shindeNo ratings yet
- Alexthymia in Sexual Disorder Clinic PatientsDocument7 pagesAlexthymia in Sexual Disorder Clinic PatientsFélix Aníbal Acuña OlivosNo ratings yet
- The Female Reproductive System: Dr. Emanuel Muro HkmuDocument41 pagesThe Female Reproductive System: Dr. Emanuel Muro HkmuMustafa DadahNo ratings yet
- Effect of Ethanol Leaf Extract of Chromolaena Odorata On Lipid Profile of Streptozotocin Induced Diabetic Wistar Albino RatsDocument9 pagesEffect of Ethanol Leaf Extract of Chromolaena Odorata On Lipid Profile of Streptozotocin Induced Diabetic Wistar Albino RatsPUBLISHER JOURNALNo ratings yet
- AP Psychology Review in 40 CharactersDocument83 pagesAP Psychology Review in 40 CharactersKitty chenNo ratings yet
- Cognitive Behavior Interventions For Self Defeating Thoughts Helping Clients To Overcome The Tyranny of I Cant 9780367460730 9780367460716 9781003026730 - CompressDocument335 pagesCognitive Behavior Interventions For Self Defeating Thoughts Helping Clients To Overcome The Tyranny of I Cant 9780367460730 9780367460716 9781003026730 - Compressnr3884424No ratings yet
- Argument Essay Final - Katie Adams 2Document6 pagesArgument Essay Final - Katie Adams 2api-608656301No ratings yet
- Jurnal MastoiditisDocument12 pagesJurnal Mastoiditisahtiyal murdinNo ratings yet
- How To Make Easy French ToastDocument4 pagesHow To Make Easy French Toastbintang pamungkasNo ratings yet
- Can Low-Fat Nutrition Labels Lead To Obesity PDFDocument15 pagesCan Low-Fat Nutrition Labels Lead To Obesity PDFSepti Lidya sariNo ratings yet
- Curriculum Vitae: Amir E. Ibrahim, M.DDocument11 pagesCurriculum Vitae: Amir E. Ibrahim, M.DkendoNo ratings yet
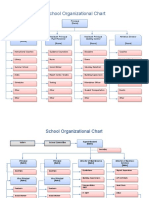
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- mgmt404 Final Project HMPDocument22 pagesmgmt404 Final Project HMPapi-25526962850% (2)
- Ethics in DentistryDocument4 pagesEthics in DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- LONG QUIZ # 1 IN ENGLISH 8 (4th Grading PeriodDocument2 pagesLONG QUIZ # 1 IN ENGLISH 8 (4th Grading PeriodAnthony Gio L. AndayaNo ratings yet
- Talent Management SystemDocument22 pagesTalent Management SystemDeepa Yadav100% (1)
- Microlife BP A3 Plus: EN ES FR IT DE TR PT NL GR ARDocument81 pagesMicrolife BP A3 Plus: EN ES FR IT DE TR PT NL GR ARYatzy Choi NekitoNo ratings yet
- Potensi Bahaya Fisika, Kimia, Biologi, Ergonomi, Dan Psikologi Pada Tenaga Kerja Di Area Produksi Pabrik GulaDocument5 pagesPotensi Bahaya Fisika, Kimia, Biologi, Ergonomi, Dan Psikologi Pada Tenaga Kerja Di Area Produksi Pabrik GulailhamNo ratings yet
- EpidemiologyDocument100 pagesEpidemiologyKailash NagarNo ratings yet
- Synopsis Format-1Document12 pagesSynopsis Format-1astha SinghNo ratings yet
- PSYCHOLOGY Lesson 2Document15 pagesPSYCHOLOGY Lesson 2KOSTKANo ratings yet