You might also like
- Pgi Manimtim - PFC MatrixDocument14 pagesPgi Manimtim - PFC MatrixKim Adarem Joy Manimtim100% (2)
- Energy conservation techniques for respiratory patientsDocument9 pagesEnergy conservation techniques for respiratory patientsqwas zNo ratings yet
- Therapeutic Exercise: Impact on Physical FunctionDocument30 pagesTherapeutic Exercise: Impact on Physical FunctionMyrgen TingsonNo ratings yet
- PAE 5 Techniques of The Treatment With Faradic Type Current-1Document35 pagesPAE 5 Techniques of The Treatment With Faradic Type Current-1Huzaifa HabibNo ratings yet
- Brachial Plexus InjuryDocument21 pagesBrachial Plexus InjurySemi IqbalNo ratings yet
- Orthopaedic Management in Cerebral Palsy, 2nd EditionFrom EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannRating: 3 out of 5 stars3/5 (2)
- At The Crossroads of Gout and Psoriatic Arthritis: "Psout"Document9 pagesAt The Crossroads of Gout and Psoriatic Arthritis: "Psout"ireneardianiNo ratings yet
- Palliative Care Billing 101Document47 pagesPalliative Care Billing 101mturchianoNo ratings yet
- Comparison of UMN & LMN SyndromesDocument2 pagesComparison of UMN & LMN SyndromesPJHGNo ratings yet
- Physiotherapy Management in Icu Patients: Dr.S.Ramachandran MPTDocument37 pagesPhysiotherapy Management in Icu Patients: Dr.S.Ramachandran MPTvaishnaviNo ratings yet
- Tinetti Assessment Tool: Balance and Gait TestDocument3 pagesTinetti Assessment Tool: Balance and Gait TestAlexandra DeacNo ratings yet
- Low Back Pain ICD-10 Code M54.5Document1 pageLow Back Pain ICD-10 Code M54.5fisioterapi 2019No ratings yet
- Proprioceptive Neuromuscular Facilitation (PNF) Stretching Techniques Hold-Relax HR ALLDocument8 pagesProprioceptive Neuromuscular Facilitation (PNF) Stretching Techniques Hold-Relax HR ALLKiné Therapeut-manuelle Masseur GabiNo ratings yet
- AARC Clinical Practice Guideline - Pulmonary RehabilitationDocument9 pagesAARC Clinical Practice Guideline - Pulmonary RehabilitationCristina CamachoNo ratings yet
- Normal Human LocomotionDocument16 pagesNormal Human LocomotionWendy NgNo ratings yet
- Postural Drainage& Breathing ExerciseDocument33 pagesPostural Drainage& Breathing ExerciseIkon ikonic100% (1)
- Bronchiectasis Pa Tho Physiology, Presentation and ManagementDocument8 pagesBronchiectasis Pa Tho Physiology, Presentation and ManagementCristhian MellaNo ratings yet
- Physiotherapy For Cardiac SurgeryDocument15 pagesPhysiotherapy For Cardiac SurgeryMuruganNo ratings yet
- Exercise Metabolism, Carbohydrates and LipidsDocument39 pagesExercise Metabolism, Carbohydrates and LipidsMohdSyamRoslanNo ratings yet
- Low Back Pain Lapkas 2Document27 pagesLow Back Pain Lapkas 2rini najoanNo ratings yet
- Physical Examination of The SpineDocument33 pagesPhysical Examination of The SpineyudiNo ratings yet
- Healing of Bone and Cartilage FracturesDocument36 pagesHealing of Bone and Cartilage Fracturescatharinam100% (1)
- The History of COPDDocument12 pagesThe History of COPDcarloscano1994No ratings yet
- PNF Techniques for Strengthening MusclesDocument76 pagesPNF Techniques for Strengthening MusclesHasan KhawaldehNo ratings yet
- Therapybook Interferencial TherapyDocument34 pagesTherapybook Interferencial TherapyBrian RaymondNo ratings yet
- Lung SurgeriesDocument43 pagesLung SurgeriesSereinNo ratings yet
- SoalDocument8 pagesSoalNunis Nur AzizahNo ratings yet
- Theraex For IKFRDocument130 pagesTheraex For IKFRsingle_ladyNo ratings yet
- Tes 1Document20 pagesTes 1Nunis Nur Azizah100% (1)
- 7-3-9 - Chest PhysiotherapyDocument10 pages7-3-9 - Chest PhysiotherapyPrabu G SatiyaNo ratings yet
- Foot Function Index: Pain Subscale: How Severe Is Your Foot PainDocument1 pageFoot Function Index: Pain Subscale: How Severe Is Your Foot Painmekar retnoningsihNo ratings yet
- ICUDocument12 pagesICUNabilahNo ratings yet
- Frozen Shoulder MX Guideline (Full) Natlie Yuen 2011Document14 pagesFrozen Shoulder MX Guideline (Full) Natlie Yuen 2011pangNo ratings yet
- Regenerative RehabilitationDocument9 pagesRegenerative RehabilitationAndreeaBubuNo ratings yet
- McKenzie CONCEPT AnilDocument12 pagesMcKenzie CONCEPT AnilSOUMYADEEP BHUINYANo ratings yet
- PAE 1 Introduction To ElectrotherapyDocument37 pagesPAE 1 Introduction To ElectrotherapyHasnat AhmedNo ratings yet
- Functional Exercise ProgressionDocument6 pagesFunctional Exercise ProgressionAnastasia Skamagki100% (1)
- Chest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Document19 pagesChest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Physio EbookNo ratings yet
- De Quervain SyndromeDocument5 pagesDe Quervain Syndromebangla018No ratings yet
- BFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesDocument9 pagesBFO-Ankle Foot Orthotics - Introduction and Biomechanical PrinciplesnovitaNo ratings yet
- The Role of Physical Therapy & Rehabilitation in Mechanical Low Back PainDocument40 pagesThe Role of Physical Therapy & Rehabilitation in Mechanical Low Back PainruriNo ratings yet
- Neck Pain Disability Index QuestionnaireDocument2 pagesNeck Pain Disability Index Questionnairericha_mahajan_8No ratings yet
- Kumpulan Soal Modas2Document7 pagesKumpulan Soal Modas2Nikolas EdwinNo ratings yet
- PathomechanicsDocument8 pagesPathomechanicsMike B AndersonNo ratings yet
- The Cyriax Method of MSK Examination ROMDocument78 pagesThe Cyriax Method of MSK Examination ROMMittulNo ratings yet
- The Active Cycle of Breathing Technique (Acbt) : Slightly, It Should Fall As You Breathe Out - Do Not Force The Air OutDocument2 pagesThe Active Cycle of Breathing Technique (Acbt) : Slightly, It Should Fall As You Breathe Out - Do Not Force The Air OutGopi KrishnanNo ratings yet
- Brunnstorm ApproachDocument33 pagesBrunnstorm ApproachFareeha KausarNo ratings yet
- Rehabilitation of LeprosyDocument72 pagesRehabilitation of LeprosyNur OctavianiNo ratings yet
- Foot and Ankle ArthrokinematicsDocument6 pagesFoot and Ankle ArthrokinematicsCraig StewartNo ratings yet
- Short Wave Diathermy Is Defined As The Clinical Application of High Frequency Alternating Current, at A Frequency of 27.12Mhz and Wavelength of 11.06 MeterDocument1 pageShort Wave Diathermy Is Defined As The Clinical Application of High Frequency Alternating Current, at A Frequency of 27.12Mhz and Wavelength of 11.06 MeterMohd AsadNo ratings yet
- Shoulder ComplexDocument55 pagesShoulder ComplexKim VillalobosNo ratings yet
- 4 Diathermy SWD MWDDocument63 pages4 Diathermy SWD MWDmupt77No ratings yet
- Antenatal and Postnatal PPT PDFDocument15 pagesAntenatal and Postnatal PPT PDFNikita -0251 ENo ratings yet
- 1.laser TherapyDocument12 pages1.laser TherapyFaisal Mehboob67% (3)
- Orthotic Prescription Factors for KAFODocument54 pagesOrthotic Prescription Factors for KAFOFERYANDA UTAMI100% (1)
- Foundation Handout For Physical Therapy Students in OLFUDocument3 pagesFoundation Handout For Physical Therapy Students in OLFUBogart Macatangay100% (1)
- Arthrokinematics of Body Joints FinalDocument3 pagesArthrokinematics of Body Joints FinalnmahpbooksNo ratings yet
- Physiotherapy in Disaster MenegementDocument82 pagesPhysiotherapy in Disaster MenegementAtiKa YuLiantiNo ratings yet
- DiathermyDocument55 pagesDiathermyHaniya KhanNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionFrom EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionNo ratings yet
- MEDICAL EMERGENCY RESPONSE PLAN Draft KolomDocument42 pagesMEDICAL EMERGENCY RESPONSE PLAN Draft Kolomfarid akbarNo ratings yet
- Img 0003Document1 pageImg 0003farid akbarNo ratings yet
- Acute Renal Failure DXDocument7 pagesAcute Renal Failure DXfarid akbarNo ratings yet
- Img 0004Document1 pageImg 0004farid akbarNo ratings yet
- FINAL MARET 22 - TGI-MN-07-10 Emergency Response Plan (Rev-02) 23 Mar 2022 - Review by RMCGDocument69 pagesFINAL MARET 22 - TGI-MN-07-10 Emergency Response Plan (Rev-02) 23 Mar 2022 - Review by RMCGfarid akbarNo ratings yet
- Rqrue6s5ffi: RZXS'ZDocument1 pageRqrue6s5ffi: RZXS'Zfarid akbarNo ratings yet
- Img 0002Document1 pageImg 0002farid akbarNo ratings yet
- Monthly Report April 2017Document4 pagesMonthly Report April 2017farid akbarNo ratings yet
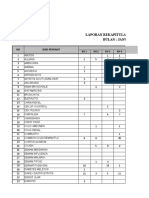
- Laporan Rekapitulasi Jenis Penyakit Bulan: Januari 2018: FM-SAG-ADM-KTU-050008Document8 pagesLaporan Rekapitulasi Jenis Penyakit Bulan: Januari 2018: FM-SAG-ADM-KTU-050008farid akbarNo ratings yet
- Grafik Disease Hikmah Dua Des 2016Document1 pageGrafik Disease Hikmah Dua Des 2016farid akbarNo ratings yet
- Laporan Rekapitulasi Jenis Penyakit Bulan: Februari 2018: FM-SAG-ADM-KTU-050008Document8 pagesLaporan Rekapitulasi Jenis Penyakit Bulan: Februari 2018: FM-SAG-ADM-KTU-050008farid akbarNo ratings yet
- Laporan Rekapitulasi Jenis Penyakit Bulan:Maret 2018: FM-SAG-ADM-KTU-050008Document8 pagesLaporan Rekapitulasi Jenis Penyakit Bulan:Maret 2018: FM-SAG-ADM-KTU-050008farid akbarNo ratings yet
- Water and Sodium BalanceDocument4 pagesWater and Sodium Balanceapi-3712326No ratings yet
- Audit Report RSPODocument12 pagesAudit Report RSPOfarid akbarNo ratings yet
- PT TELAGA HIKMAH PHYSICAL INVENTORY RESULTSDocument10 pagesPT TELAGA HIKMAH PHYSICAL INVENTORY RESULTSfarid akbarNo ratings yet
- Stok 1-30 September 2017Document12 pagesStok 1-30 September 2017farid akbarNo ratings yet
- Stock Opname April 2017Document11 pagesStock Opname April 2017farid akbarNo ratings yet
- Stok Opname Oktober 17Document12 pagesStok Opname Oktober 17farid akbarNo ratings yet
- Pt. Telaga Hikmah Unit: Kebun Hikmah SatuDocument11 pagesPt. Telaga Hikmah Unit: Kebun Hikmah Satufarid akbarNo ratings yet
- STOCK OPNAME September 2017Document10 pagesSTOCK OPNAME September 2017farid akbarNo ratings yet
- Stok Opname November 17Document12 pagesStok Opname November 17farid akbarNo ratings yet
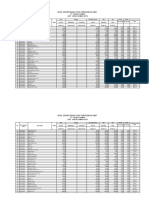
- Hasil Perhitungan Fisik Persediaan Obat: Pt. Telaga Hikmah Unit: Kebun Hikmah SatuDocument11 pagesHasil Perhitungan Fisik Persediaan Obat: Pt. Telaga Hikmah Unit: Kebun Hikmah Satufarid akbarNo ratings yet
- Stock Opname Aprl 2017Document12 pagesStock Opname Aprl 2017farid akbarNo ratings yet
- PT Telaga Hikmah Physical Inventory ResultsDocument10 pagesPT Telaga Hikmah Physical Inventory Resultsfarid akbarNo ratings yet
- Stock Opname Aprl 2017Document12 pagesStock Opname Aprl 2017farid akbarNo ratings yet
- Stok Opname Juni 2017Document4 pagesStok Opname Juni 2017farid akbarNo ratings yet
- Stok Opname Mei 2017Document5 pagesStok Opname Mei 2017farid akbarNo ratings yet
- Stok Opname April 2017-1Document4 pagesStok Opname April 2017-1farid akbarNo ratings yet
- Pt. Telaga Hikmah Unit: Kebun Hikmah SatuDocument10 pagesPt. Telaga Hikmah Unit: Kebun Hikmah Satufarid akbarNo ratings yet
- Stock Opname Aprl 2017Document12 pagesStock Opname Aprl 2017farid akbarNo ratings yet
- Vaccines Wavre 2019 Ir Event Slides 26 Sep 2019 Final 3Document45 pagesVaccines Wavre 2019 Ir Event Slides 26 Sep 2019 Final 3hau vuvanNo ratings yet
- Stamford University Bangladesh: Assignment On COVID 19 and Its Impact On Service IndustryDocument8 pagesStamford University Bangladesh: Assignment On COVID 19 and Its Impact On Service IndustryRI ShawonNo ratings yet
- Stress and Adjustment DisorderDocument32 pagesStress and Adjustment DisorderSharvari ShahNo ratings yet
- Medical Surgical 1 PDFDocument19 pagesMedical Surgical 1 PDFheyyymeeeNo ratings yet
- Acute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODocument29 pagesAcute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODOCTOR DanishNo ratings yet
- ACC166 Example 1Document4 pagesACC166 Example 1URANG CHITONo ratings yet
- Practice QuestionsDocument32 pagesPractice QuestionsMary Danielle SaludarioNo ratings yet
- Krok 19 20 21 - CompressedDocument148 pagesKrok 19 20 21 - CompressedPaulNo ratings yet
- AtherosclerosisDocument23 pagesAtherosclerosisPoonam soniNo ratings yet
- Human Capital: Education and Health in Economic DevelopmentDocument16 pagesHuman Capital: Education and Health in Economic DevelopmentRoselle Jane LanabanNo ratings yet
- Лекция 7Document76 pagesЛекция 7ramtin malekshahiNo ratings yet
- Serum CPK Levels Indicative of Oral Cancer SeverityDocument4 pagesSerum CPK Levels Indicative of Oral Cancer SeverityDeepak KumarNo ratings yet
- Keratosis ObturansDocument2 pagesKeratosis ObturansAnish RajNo ratings yet
- 10 AnxietyDocument24 pages10 AnxietyAhinsa LokudadallaNo ratings yet
- Lecture-10 (Body and Spirit) (Compatibility Mode)Document50 pagesLecture-10 (Body and Spirit) (Compatibility Mode)DS E100% (1)
- PSYC A232 Study Guide U3 236Document26 pagesPSYC A232 Study Guide U3 236TKTGNo ratings yet
- RLE Module for Colorectal CancerDocument16 pagesRLE Module for Colorectal CancerDa BondadNo ratings yet
- Cellulitis: SHVNDR 1Document13 pagesCellulitis: SHVNDR 1Simran SinghNo ratings yet
- Top 100 Pathology Secrets List W/ NotesDocument6 pagesTop 100 Pathology Secrets List W/ NotesPA2014100% (4)
- NCMB 312 Midterms Dash 7Document65 pagesNCMB 312 Midterms Dash 7Roseann meranoNo ratings yet
- HEALTH INFINITY Plan ONE PagerDocument3 pagesHEALTH INFINITY Plan ONE PagerVikas SharmaNo ratings yet
- OCD ChecklistDocument3 pagesOCD ChecklistfarrukhakhtarNo ratings yet
- Nur3111p Professionalism and Lifelong Learning ReflectionDocument6 pagesNur3111p Professionalism and Lifelong Learning Reflectionapi-578141969No ratings yet
- Gait Analysis GuideDocument66 pagesGait Analysis GuidesenoNo ratings yet
- Confounding and Effect Modification ExplainedDocument49 pagesConfounding and Effect Modification Explainedtakele loveNo ratings yet
- To Do SWTDocument8 pagesTo Do SWTnirajan parajuliNo ratings yet
- Purposive Communication Module 4Document9 pagesPurposive Communication Module 4Kristine G. BatanesNo ratings yet