You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ele&Arr&Com&Rev&Das&Zip&1 STDocument492 pagesEle&Arr&Com&Rev&Das&Zip&1 STeuinpersoana100% (3)
- Osmosis ECG EKG BookDocument61 pagesOsmosis ECG EKG Booknadia amalia pusadan88% (8)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Stemi, Stemi Equivalents and STEMI Mimics: Kyaw Soe WinDocument114 pagesStemi, Stemi Equivalents and STEMI Mimics: Kyaw Soe WinYoung MilkNo ratings yet
- GREY BOOK August 2017 66thDocument146 pagesGREY BOOK August 2017 66thxedoyis969No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- RN Pocket Guide 2nd Edition PDFDocument200 pagesRN Pocket Guide 2nd Edition PDFTasha100% (1)
- ECG Case Studies Moosa1.Document54 pagesECG Case Studies Moosa1.m.ikhsan.adi.nugrahaNo ratings yet
- Diagnosis of IMADocument32 pagesDiagnosis of IMARamón Ruesta BerdejoNo ratings yet
- Ecg Eeg EmgDocument16 pagesEcg Eeg EmgNeha100% (1)
- Understanding Pediatric ECGDocument8 pagesUnderstanding Pediatric ECGNabeel Obad100% (1)
- ECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial CentreDocument90 pagesECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial Centrevaishali TayadeNo ratings yet
- ECG Changes in Drug and Electrolyte AbnormalitiesDocument28 pagesECG Changes in Drug and Electrolyte AbnormalitiesNachiket Vijay PotdarNo ratings yet
- Systemic AmyloidosisDocument25 pagesSystemic AmyloidosisMathew McCarthy100% (1)
- DOI - ReviewedDoiSummary EHRA NOAC 2021 ReviewersDocument4 pagesDOI - ReviewedDoiSummary EHRA NOAC 2021 ReviewersMathew McCarthyNo ratings yet
- Left Atrial Expansion Index Predicts All-Cause Mortality and Heart Failure Admissions in DyspnoeaDocument8 pagesLeft Atrial Expansion Index Predicts All-Cause Mortality and Heart Failure Admissions in DyspnoeaMathew McCarthyNo ratings yet
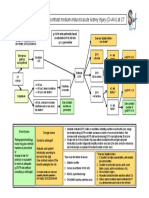
- Risk Assessment of Contrast Medium-Induced Acute Kidney Injury (CI-AKI) at CTDocument1 pageRisk Assessment of Contrast Medium-Induced Acute Kidney Injury (CI-AKI) at CTMathew McCarthyNo ratings yet
- MamaGioMeny Host 22 ENGDocument2 pagesMamaGioMeny Host 22 ENGMathew McCarthyNo ratings yet
- Rest and Inf CMPs P1Document19 pagesRest and Inf CMPs P1Mathew McCarthyNo ratings yet
- Nejmra 2000348Document16 pagesNejmra 2000348Mathew McCarthyNo ratings yet
- Victims of Success in Failure: CirculationDocument3 pagesVictims of Success in Failure: CirculationMathew McCarthyNo ratings yet
- Jeaa 243Document10 pagesJeaa 243Mathew McCarthyNo ratings yet
- Tailor PciDocument11 pagesTailor PciMathew McCarthyNo ratings yet
- Schmidt Int J Cardiovasc ImagDocument8 pagesSchmidt Int J Cardiovasc ImagMathew McCarthyNo ratings yet
- Acs 2022 Bav 18Document10 pagesAcs 2022 Bav 18Mathew McCarthyNo ratings yet
- Ehra Consensus Paper: Europace (2020) 22, 515-516 Doi:10.1093/europace/euz246Document35 pagesEhra Consensus Paper: Europace (2020) 22, 515-516 Doi:10.1093/europace/euz246Mathew McCarthyNo ratings yet
- Prognostic Significance of Left Ventricular Noncompaction: Original ArticleDocument14 pagesPrognostic Significance of Left Ventricular Noncompaction: Original ArticleMathew McCarthyNo ratings yet
- Extensive Dermatitis (Coumadin) : Due Warfarin SodiumDocument2 pagesExtensive Dermatitis (Coumadin) : Due Warfarin SodiumMathew McCarthyNo ratings yet
- Swedish: An Elementary Grammar-Reader PDF, Epub, EbookDocument5 pagesSwedish: An Elementary Grammar-Reader PDF, Epub, EbookMathew McCarthyNo ratings yet
- Practical Guidance in Echocardiographic Assessment of Global Longitudinal StrainDocument4 pagesPractical Guidance in Echocardiographic Assessment of Global Longitudinal StrainMathew McCarthyNo ratings yet
- Position PaperDocument16 pagesPosition PaperMathew McCarthyNo ratings yet
- GaibazziDocument7 pagesGaibazziMathew McCarthyNo ratings yet
- Circulationaha 122 059598Document10 pagesCirculationaha 122 059598Mathew McCarthyNo ratings yet
- Euab 065Document65 pagesEuab 065Mathew McCarthyNo ratings yet
- Esc CurriculumDocument88 pagesEsc CurriculumMathew McCarthyNo ratings yet
- Bar MenuDocument13 pagesBar MenuMathew McCarthyNo ratings yet
- HCMP Multimodality ImagingDocument16 pagesHCMP Multimodality ImagingMathew McCarthyNo ratings yet
- Imail: Cardiac Magnetic Resonance Imaging in Danon Disease CardiomyopathyDocument2 pagesImail: Cardiac Magnetic Resonance Imaging in Danon Disease CardiomyopathyMathew McCarthyNo ratings yet
- Biomarkers in AmyloidosisDocument11 pagesBiomarkers in AmyloidosisMathew McCarthyNo ratings yet
- The Myocardial Phenotype of Fabry Disease Pre-Hypertrophy and Pre-Detectable StorageDocument10 pagesThe Myocardial Phenotype of Fabry Disease Pre-Hypertrophy and Pre-Detectable StorageMathew McCarthyNo ratings yet
- Ecg Ospe QuizDocument26 pagesEcg Ospe Quizsivakamasundari pichaipillaiNo ratings yet
- ECG For Beginners PDFDocument153 pagesECG For Beginners PDFIonut MoisaNo ratings yet
- PericarditisDocument37 pagesPericarditispriyanka bhowmikNo ratings yet
- QuestionsDocument55 pagesQuestionsInchic MirandaNo ratings yet
- Myocardial InfarctionDocument17 pagesMyocardial InfarctionJoshua ReyesNo ratings yet
- VeltassaDocument3 pagesVeltassaMikaela Gabrielle GeraliNo ratings yet
- Jose Gianni C. Espada Clinical ClerkDocument133 pagesJose Gianni C. Espada Clinical ClerkJohn Christopher LucesNo ratings yet
- CVS ElectrocardiogramDocument167 pagesCVS ElectrocardiogramSheral AidaNo ratings yet
- ECG EKG Examples and QuizDocument26 pagesECG EKG Examples and QuizBUBBUNo ratings yet
- Electrocardiogram: Dr. PacnaDocument13 pagesElectrocardiogram: Dr. PacnaEcel AggasidNo ratings yet
- ECG PresentationDocument52 pagesECG PresentationShah NahidNo ratings yet
- MCQ'S Part 2Document169 pagesMCQ'S Part 2Kripa SusanNo ratings yet
- ECGchanges in Patients With Acute StrokeDocument6 pagesECGchanges in Patients With Acute StrokeV RakeshreddyNo ratings yet
- (2019) Passmedicine - Passmedicine MRCP Part IDocument6,249 pages(2019) Passmedicine - Passmedicine MRCP Part IAchyut KanungoNo ratings yet
- Deep Learning For ECG SegmentationDocument10 pagesDeep Learning For ECG SegmentationPablo FonsecaNo ratings yet
- Dolor ToracicoDocument11 pagesDolor ToracicoSandy A.No ratings yet
- Ecg 1Document50 pagesEcg 1Rohit DagarNo ratings yet
- Medical Investigations PDFDocument136 pagesMedical Investigations PDFFathy ElsheshtawyNo ratings yet
- E Lectrocardiography ECG: Practical Physiology 2020-2021 LabDocument8 pagesE Lectrocardiography ECG: Practical Physiology 2020-2021 LabBushra AlkaqaniNo ratings yet