You might also like
- PCAP Pediatric Community Acquired Pneumonia PATHOPHYSIOLOGYDocument2 pagesPCAP Pediatric Community Acquired Pneumonia PATHOPHYSIOLOGYCHRISTIE MONTANO25% (4)
- SCI Cheat SheetDocument4 pagesSCI Cheat SheetJohann Sebastian CruzNo ratings yet
- Consumers Math ElectiveDocument1 pageConsumers Math ElectiveAdiel CalsaNo ratings yet
- Medication DilutionDocument22 pagesMedication DilutionYaser Salman100% (1)
- Nicotine - It May Have A Good Side - Harvard HealthDocument3 pagesNicotine - It May Have A Good Side - Harvard HealthzimkoNo ratings yet
- Exercise Physiology Theory and Application To Fitness and Performance Eleventh Edition Scott K Powers Full ChapterDocument68 pagesExercise Physiology Theory and Application To Fitness and Performance Eleventh Edition Scott K Powers Full Chapterhoward.mcguirl514100% (3)
- Autonomic Nervous System - Part 1Document8 pagesAutonomic Nervous System - Part 1karageeNo ratings yet
- Ecg Placement RetdemDocument3 pagesEcg Placement RetdemDianne Erika MeguinesNo ratings yet
- Disorder of Respiratory SystemDocument89 pagesDisorder of Respiratory SystemDarine Nasr100% (1)
- 3 ReviewerDocument46 pages3 ReviewerSHINE JASMIN LAXAMANA100% (1)
- Myasthenia GravisDocument2 pagesMyasthenia GravisJulia SalvioNo ratings yet
- Med-Surg Lecture 4th Year 1st Sem (Incomplete)Document70 pagesMed-Surg Lecture 4th Year 1st Sem (Incomplete)Raezhell Dianne RachoNo ratings yet
- Amputation Lower ExtremityDocument5 pagesAmputation Lower ExtremityJulia SalvioNo ratings yet
- Angina PectorisDocument8 pagesAngina PectorisJoanne LagusadNo ratings yet
- Total Hip Replacement - ProtocolDocument1 pageTotal Hip Replacement - ProtocolAhmad Rifai SarrajNo ratings yet
- EKG Quick ViewDocument1 pageEKG Quick ViewJe KirsteneNo ratings yet
- Management of ArrhythmiasDocument4 pagesManagement of ArrhythmiasAray Al-AfiqahNo ratings yet
- CA PEDIA Hand OutDocument13 pagesCA PEDIA Hand OutarianeNo ratings yet
- Pediatric Medication Math Review Jan 2011Document7 pagesPediatric Medication Math Review Jan 2011Tyrone Kent HalogNo ratings yet
- Alzheimer Dementia: Starting, Stopping Drug Therapy: ReviewDocument6 pagesAlzheimer Dementia: Starting, Stopping Drug Therapy: ReviewAnonymous ZUaUz1wwNo ratings yet
- Nur 111 Session 17 Sas 1Document8 pagesNur 111 Session 17 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Pathophysiology of Atrial FibrillationDocument12 pagesPathophysiology of Atrial FibrillationAndrew Surya Putra SccNo ratings yet
- UPump Pediatric NursingDocument21 pagesUPump Pediatric NursingJan Leslie VergaraNo ratings yet
- Comprehensive Lower Extremity AnatomyDocument53 pagesComprehensive Lower Extremity Anatomy정형화No ratings yet
- Pathophysiology of Acute Renal FailureDocument1 pagePathophysiology of Acute Renal FailureAina HaravataNo ratings yet
- Peripheral Artery DiseaseDocument42 pagesPeripheral Artery Diseaseadamu mohammadNo ratings yet
- IICP TransesDocument3 pagesIICP TransesJulia Rae Delos SantosNo ratings yet
- Drug Name Mechanism of Action Indication Side Effects/ Adverse Effects Contraindicatio N Nursing ConsiderationDocument9 pagesDrug Name Mechanism of Action Indication Side Effects/ Adverse Effects Contraindicatio N Nursing ConsiderationVanessa Naomi GalidoNo ratings yet
- Acute Coronary SyndromeDocument32 pagesAcute Coronary SyndromeVicky Lumalessil100% (2)
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- Cardio MnemonicsDocument21 pagesCardio MnemonicsAilene Ponce FillonNo ratings yet
- Motor Neuron DiseaseDocument4 pagesMotor Neuron Diseasem3d1kNo ratings yet
- Ncm116 CDN Nervous LecDocument11 pagesNcm116 CDN Nervous LecMilcah NuylesNo ratings yet
- Jade R. Dinolan BSN-4: Diagnosi SDocument5 pagesJade R. Dinolan BSN-4: Diagnosi SJhade Relleta100% (1)
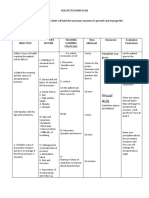
- Nursing Care PlanDocument10 pagesNursing Care PlanmariasomorayNo ratings yet
- I. A. Brief Description: Chakinala, 2015)Document54 pagesI. A. Brief Description: Chakinala, 2015)Kacelyn QuibanNo ratings yet
- Case Study (Pleural Effusion)Document4 pagesCase Study (Pleural Effusion)Jvspapa ShilohNo ratings yet
- The Balanced Skeletal TractionDocument1 pageThe Balanced Skeletal TractionGemarie Adarlo CastilloNo ratings yet
- 2 PlanningDocument8 pages2 PlanningAudrey Ann AcobNo ratings yet
- Midterms GeriaDocument18 pagesMidterms GeriaGiselle Estoquia100% (1)
- GYNECOLOGICALNURSINGDocument4 pagesGYNECOLOGICALNURSINGSheana TmplNo ratings yet
- Communicable Disease NursingDocument22 pagesCommunicable Disease NursingNur SanaaniNo ratings yet
- Neuro - Sir Chavez - AS OF 12PMDocument5 pagesNeuro - Sir Chavez - AS OF 12PMCarl JustineNo ratings yet
- Nervous Sytem 1Document11 pagesNervous Sytem 1Elaine Victoria ElizanNo ratings yet
- Nur 111 Session 18 Sas 1Document11 pagesNur 111 Session 18 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- 118 RLE Mechanical Ventilation PDFDocument5 pages118 RLE Mechanical Ventilation PDFclaire yowsNo ratings yet
- Cardiovascular System: AnatomyDocument19 pagesCardiovascular System: AnatomyStephanie MacVeighNo ratings yet
- NVS Written ReportDocument20 pagesNVS Written ReportbabiNo ratings yet
- Heart - CaDocument313 pagesHeart - Cafrenee aradanasNo ratings yet
- RLE NCMB 314-M2-CU8 Cardiovascular ChangesDocument5 pagesRLE NCMB 314-M2-CU8 Cardiovascular ChangesJordz PlaciNo ratings yet
- Acute Respiratory FailureDocument7 pagesAcute Respiratory FailureNurol-Ainah Hafizah U. PimpingNo ratings yet
- Intracerebral HemorrageDocument13 pagesIntracerebral HemorrageChristian JuarezNo ratings yet
- Ca - MS (Respiratory)Document4 pagesCa - MS (Respiratory)kyleNo ratings yet
- Perioperative Nursing Version 2Document38 pagesPerioperative Nursing Version 2Justine CagatanNo ratings yet
- Case 8 NCP (Multiple Sclerosis)Document2 pagesCase 8 NCP (Multiple Sclerosis)je-ann catedralNo ratings yet
- Cardiovascular Agents: Florianne E. Adlawan, R.NDocument31 pagesCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneNo ratings yet
- Medical-Surgical Nursing ArthritisDocument8 pagesMedical-Surgical Nursing ArthritisNoelyn BaluyanNo ratings yet
- Central Venous Pressure Monitoring: Assisting With CVP PlacementDocument3 pagesCentral Venous Pressure Monitoring: Assisting With CVP PlacementGlare RhayneNo ratings yet
- Cardivascular SystemDocument11 pagesCardivascular SystemAnneMarielleManaloNo ratings yet
- History and Assessment & Anatomy and Physiology of BurnsDocument10 pagesHistory and Assessment & Anatomy and Physiology of BurnsRina MaeNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- Ms Penta NotesDocument84 pagesMs Penta Notesshenric16No ratings yet
- Neurologic NursingDocument10 pagesNeurologic NursingAllisson Beckers100% (1)
- MPS Grade 2 Conso Filipino 2020 2021Document2 pagesMPS Grade 2 Conso Filipino 2020 2021Vhince PiscoNo ratings yet
- Implementation and Monitoring Mechanism For Blended ModularDocument13 pagesImplementation and Monitoring Mechanism For Blended ModularVhince PiscoNo ratings yet
- STS L 1.3 With AnswersDocument5 pagesSTS L 1.3 With AnswersVhince PiscoNo ratings yet
- Philo of Man CapSLET LC 4.1Document9 pagesPhilo of Man CapSLET LC 4.1Vhince PiscoNo ratings yet
- Philo of Man CapSLET LC 4.3Document10 pagesPhilo of Man CapSLET LC 4.3Vhince PiscoNo ratings yet
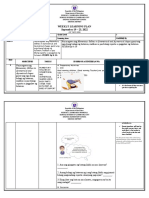
- WLP - Math2 Q1 W5 1 4Document10 pagesWLP - Math2 Q1 W5 1 4Vhince PiscoNo ratings yet
- Republic of The Philippines Department of Education Region Ix, Zamboanga Peninsula Schools Division of Zamboanga City Sinunuc DistrictDocument3 pagesRepublic of The Philippines Department of Education Region Ix, Zamboanga Peninsula Schools Division of Zamboanga City Sinunuc DistrictVhince PiscoNo ratings yet
- MTB WLP Q1 W4 Day1 4Document9 pagesMTB WLP Q1 W4 Day1 4Vhince PiscoNo ratings yet
- STS L 2.3 With AnswersDocument5 pagesSTS L 2.3 With AnswersVhince PiscoNo ratings yet
- STS L 2.4 With AnswersDocument6 pagesSTS L 2.4 With AnswersVhince PiscoNo ratings yet
- STS L 3.1 With AnswersDocument6 pagesSTS L 3.1 With AnswersVhince PiscoNo ratings yet
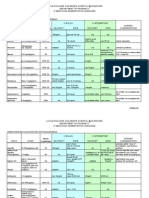
- Grade Ii Class ProgramDocument15 pagesGrade Ii Class ProgramVhince PiscoNo ratings yet
- STS L 3.2 With AnswersDocument4 pagesSTS L 3.2 With AnswersVhince PiscoNo ratings yet
- Complete File Case Study UPDATEDDocument65 pagesComplete File Case Study UPDATEDVhince PiscoNo ratings yet
- Final Sinunuc Es Form 1 and Form 1.1Document9 pagesFinal Sinunuc Es Form 1 and Form 1.1Vhince PiscoNo ratings yet
- Communicable Diseases 2.4-5.22Document9 pagesCommunicable Diseases 2.4-5.22Vhince PiscoNo ratings yet
- WLP Mapeh2p.e Q1 W5 8 Day1 4Document27 pagesWLP Mapeh2p.e Q1 W5 8 Day1 4Vhince PiscoNo ratings yet
- Ivolunteers Club Webinar LetterDocument4 pagesIvolunteers Club Webinar LetterVhince PiscoNo ratings yet
- Visual Aids: Pamphlet Was GivenDocument2 pagesVisual Aids: Pamphlet Was GivenVhince PiscoNo ratings yet
- Standard For The Management of Narcotics and Controlled Medicinal ProductsDocument10 pagesStandard For The Management of Narcotics and Controlled Medicinal ProductsVhince PiscoNo ratings yet
- Sportsfest 2019: BSN Program Snatches Second Straight WinDocument2 pagesSportsfest 2019: BSN Program Snatches Second Straight WinVhince PiscoNo ratings yet
- Chapter 3 and 4 (Chapter 5 Pending)Document31 pagesChapter 3 and 4 (Chapter 5 Pending)Vhince PiscoNo ratings yet
- Case Analysis Care of A Client With Acute Gastritis and Hypertension FinalDocument70 pagesCase Analysis Care of A Client With Acute Gastritis and Hypertension FinalVhince PiscoNo ratings yet
- Chapter 1 and 2Document24 pagesChapter 1 and 2Vhince PiscoNo ratings yet
- Arpan 9 New CollageDocument2 pagesArpan 9 New CollageVhince PiscoNo ratings yet
- Sysmex SEED Haematology InflammatoryDocument7 pagesSysmex SEED Haematology InflammatoryTzeto Han CongNo ratings yet
- Catholic Prayer List TemplateDocument4 pagesCatholic Prayer List TemplateBarangay CentroNo ratings yet
- Post Basic Bachelor of Sciences in Nursing (B.Sc.N. (PB) ) : Assignments 2022 1 YearDocument34 pagesPost Basic Bachelor of Sciences in Nursing (B.Sc.N. (PB) ) : Assignments 2022 1 YearMumthaz ANo ratings yet
- 316 RLE - Cast CareDocument4 pages316 RLE - Cast CareSophia LalagunaNo ratings yet
- Psychology and Sociology Terms For The MCATDocument53 pagesPsychology and Sociology Terms For The MCATlukehongNo ratings yet
- Atal Amrit Abhiyan: Department of Health & Family Welfare Government of AssamDocument2 pagesAtal Amrit Abhiyan: Department of Health & Family Welfare Government of AssamprantikduarahNo ratings yet
- Guia Idsa Pie Diabetico PDFDocument42 pagesGuia Idsa Pie Diabetico PDFAliciaNo ratings yet
- 10 1016@j Det 2018 05 008Document8 pages10 1016@j Det 2018 05 008Renata GoulartNo ratings yet
- TB - SeminarDocument12 pagesTB - SeminarLaith DmourNo ratings yet
- DrugsDocument2 pagesDrugsKrestine MolleNo ratings yet
- Unit 7 Application of EpidemiologyDocument33 pagesUnit 7 Application of EpidemiologySamantha Adduru100% (1)
- Vitamin B12 DeficiencyDocument12 pagesVitamin B12 DeficiencyMagazin HdPNo ratings yet
- Laboratory 3Document6 pagesLaboratory 3Mariel CaylanNo ratings yet
- Vitiligo - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument38 pagesVitiligo - Pathogenesis, Clinical Features, and Diagnosis - UpToDateInna MeratiNo ratings yet
- P3-F Prism 3 ListeningSpeaking Unit 3 L1 Vocabulary Exercise - InstructorDocument2 pagesP3-F Prism 3 ListeningSpeaking Unit 3 L1 Vocabulary Exercise - Instructorarda5456nNo ratings yet
- Jonelta Foundation School of Medicine: University of Perpetual Help System DaltaDocument5 pagesJonelta Foundation School of Medicine: University of Perpetual Help System DaltaMark Joshua CervantesNo ratings yet
- Sepsis and Severe Pneumonia (2022)Document39 pagesSepsis and Severe Pneumonia (2022)rina delsNo ratings yet
- Lecture 5 Curing and Healing Two Goals of Medicine.Document17 pagesLecture 5 Curing and Healing Two Goals of Medicine.RosaNo ratings yet
- TuberculosisDocument4 pagesTuberculosisMjel Kezhia BarrietaNo ratings yet
- ARRSILLAUFIATMA MAYHIMAMIA FAHMUAMALIA - 10319014 - Tugas Bu Endah - ENGLISH KELOMPOK 1Document11 pagesARRSILLAUFIATMA MAYHIMAMIA FAHMUAMALIA - 10319014 - Tugas Bu Endah - ENGLISH KELOMPOK 1miaNo ratings yet
- Pranic Healing For Partially Blind-A Case Study: Srikanth N Jois, Nagendra K PrasadDocument5 pagesPranic Healing For Partially Blind-A Case Study: Srikanth N Jois, Nagendra K PrasadMagdalena BozinoskaNo ratings yet
- Week 13 Check Your Understanding A. Use Your Notes. Answer The Questions Based On The LectureDocument2 pagesWeek 13 Check Your Understanding A. Use Your Notes. Answer The Questions Based On The LectureIrem YilmazNo ratings yet
- Nursing Education Department: Patient AssessmentDocument34 pagesNursing Education Department: Patient AssessmentSitti Mardiya SariolNo ratings yet
- Aspects of The Topic ReadingsDocument4 pagesAspects of The Topic ReadingsBettNo ratings yet
- Step 2 Clinical Knowledge (CK) : Sample Test QuestionsDocument55 pagesStep 2 Clinical Knowledge (CK) : Sample Test QuestionsDr.Mohammed N. AbedNo ratings yet
- Class IX-Chapter 13-Why Do We Fall IllDocument36 pagesClass IX-Chapter 13-Why Do We Fall IllPriyanshu choubeyNo ratings yet
- Syllabus Master Tung PDFDocument25 pagesSyllabus Master Tung PDFkamran ahmadNo ratings yet