You might also like
- ESC-GASTPE School COVID19 Recovery and Readiness Plan S.Y. 2020 - 2021Document5 pagesESC-GASTPE School COVID19 Recovery and Readiness Plan S.Y. 2020 - 2021Jubylyn Aficial100% (3)
- Geriatrics Eval Management Tool For FrailtyDocument2 pagesGeriatrics Eval Management Tool For FrailtyDaulat JosuaNo ratings yet
- Benefits of Exercise and Physical Activity: Why Workout? Why Exercise? Why Be Physically Active?Document5 pagesBenefits of Exercise and Physical Activity: Why Workout? Why Exercise? Why Be Physically Active?Justine MainNo ratings yet
- Pathfit02 Prelims ReviewerDocument3 pagesPathfit02 Prelims ReviewerowenbacatancorporalNo ratings yet
- Peh 12 1ST Sem-1st Quarter ReviewerDocument15 pagesPeh 12 1ST Sem-1st Quarter ReviewerRalph Louis RosarioNo ratings yet
- Be Active 2008-Factsheet ProfessionalsDocument2 pagesBe Active 2008-Factsheet ProfessionalsLaurencia LenyNo ratings yet
- Fitness - Physical ActivityDocument22 pagesFitness - Physical ActivityZizo AboshadiNo ratings yet
- Articulo Salud PublicaDocument18 pagesArticulo Salud PublicaCatherinne Quiñonez GutierrezNo ratings yet
- PATHFITT 2 - HandoutsDocument14 pagesPATHFITT 2 - HandoutsDona Caballejo- ArcenaNo ratings yet
- Exercise Prescription For Healthy Populations With Special Considerations FormattedDocument49 pagesExercise Prescription For Healthy Populations With Special Considerations Formattedashlyn granthamNo ratings yet
- Exercise Prescription in Primary Care SettingDocument34 pagesExercise Prescription in Primary Care Settingdr.gunturadwiNo ratings yet
- OKK 2 - Leo - Yunia - Exercise To Increase The Components of Physical FitnessDocument43 pagesOKK 2 - Leo - Yunia - Exercise To Increase The Components of Physical FitnessAna NurfaizahNo ratings yet
- Fitness Exercise Fitt 2Document16 pagesFitness Exercise Fitt 2darillpabilando09No ratings yet
- FITTDocument7 pagesFITTAllona VillarinNo ratings yet
- Answer Yes or No: Pre-TestDocument7 pagesAnswer Yes or No: Pre-TestNabi BratzchNo ratings yet
- Lifestyle and Weight ManagementDocument2 pagesLifestyle and Weight ManagementcashieentanNo ratings yet
- MBR 2019 - Rehab Med HandoutsDocument4 pagesMBR 2019 - Rehab Med HandoutsRgm UyNo ratings yet
- Class Presentation - Effects of Exercise On Physiologic AgingDocument26 pagesClass Presentation - Effects of Exercise On Physiologic AgingTruman ChiuNo ratings yet
- PEH1Document8 pagesPEH1Jana De LiñaNo ratings yet
- Functional Exercise To Improve Fitness Balance & AgilityDocument70 pagesFunctional Exercise To Improve Fitness Balance & Agilityhadyahmed0318No ratings yet
- Aktivitas Fisik Pada Dewasa Dan GeriatriDocument20 pagesAktivitas Fisik Pada Dewasa Dan GeriatriAdinda Suci MaghfiraNo ratings yet
- Presented By: DR - Shilpa K PrajapatiDocument46 pagesPresented By: DR - Shilpa K PrajapatijothiNo ratings yet
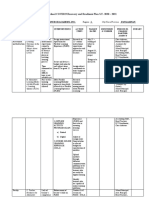
- Wollo University College of Natural & Computational Science Course Name Health and Physical Fitness Abebaw W. (MSC in S. Medicine) Feb.2021Document68 pagesWollo University College of Natural & Computational Science Course Name Health and Physical Fitness Abebaw W. (MSC in S. Medicine) Feb.2021abebawNo ratings yet
- Exercise For Fitness: (Shs-Videolecture-1 & 2 Week)Document18 pagesExercise For Fitness: (Shs-Videolecture-1 & 2 Week)Mark Joshua MandaniNo ratings yet
- Weebly Questions Week NineDocument4 pagesWeebly Questions Week Nineapi-459697337No ratings yet
- PE 02 Chapter-1Document9 pagesPE 02 Chapter-1Milk BrotherNo ratings yet
- Hubs2503 Lecture NotesDocument150 pagesHubs2503 Lecture NotesSruthi SruthiNo ratings yet
- Day 3 Principles of Rehabilitation in Elderly The NewestDocument43 pagesDay 3 Principles of Rehabilitation in Elderly The NewestaniendyawijayaNo ratings yet
- GRADE 11 PE Chapter 1 DoneDocument30 pagesGRADE 11 PE Chapter 1 DoneBananaNo ratings yet
- PA in Stroke - Chutima Aug1,2020Document25 pagesPA in Stroke - Chutima Aug1,2020ridaimroNo ratings yet
- An Introduction To Physical Activity: Study Guide For Module No. 2Document6 pagesAn Introduction To Physical Activity: Study Guide For Module No. 2MC BlancoNo ratings yet
- DISABILITYDocument8 pagesDISABILITYahmedNo ratings yet
- Fitness Training: Danish LatifDocument26 pagesFitness Training: Danish LatifShimmering MoonNo ratings yet
- Promoting Physical Activity To PatientsDocument7 pagesPromoting Physical Activity To PatientsAlexander OchoaNo ratings yet
- Presentation 2Document16 pagesPresentation 2Mohammad Ajmal MadniNo ratings yet
- Week 1 Slides Aug 31 Final StudentsDocument39 pagesWeek 1 Slides Aug 31 Final StudentsMaude GohierNo ratings yet
- Fisiologi SenamDocument4 pagesFisiologi SenamFatin FatinNo ratings yet
- Lifestyle, Fitness and WellnessDocument275 pagesLifestyle, Fitness and WellnessCaldwellNo ratings yet
- Exercise Prescription: Exercise Recommenda2ons For Persons With Special NeedsDocument29 pagesExercise Prescription: Exercise Recommenda2ons For Persons With Special NeedsThe Health Therapist AcademyNo ratings yet
- Hope 1Document4 pagesHope 1Sea are YellowNo ratings yet
- TE Chapter 1Document45 pagesTE Chapter 1tooba khanNo ratings yet
- Pathfi Module 1: Movement: C. Manipulative SkillsDocument4 pagesPathfi Module 1: Movement: C. Manipulative SkillsAndrea Gail UlitinNo ratings yet
- PE ReviewerDocument2 pagesPE ReviewerGeorgette Princess Yvonne R. GatdulaNo ratings yet
- The Benefits of ExerciseDocument3 pagesThe Benefits of ExerciseAtet KurniadiNo ratings yet
- Nutrition and Exercise Physiology 1st-1Document23 pagesNutrition and Exercise Physiology 1st-1Dawat E Islam.No ratings yet
- 10-Lecture 13 - HAN - Physical Fitness and HealthDocument24 pages10-Lecture 13 - HAN - Physical Fitness and HealthSuleiman AbdallahNo ratings yet
- WardDocument41 pagesWardSuman DeyNo ratings yet
- Fitness Tests Management For Sustainable HealthDocument5 pagesFitness Tests Management For Sustainable HealthkyleNo ratings yet
- Ronai 2013 Inespecific Low Back PainDocument4 pagesRonai 2013 Inespecific Low Back PainivanNo ratings yet
- Care of Older Adult Finals IlgDocument77 pagesCare of Older Adult Finals IlgMiden AlbanoNo ratings yet
- WELLNESSDocument2 pagesWELLNESScessyriveracruzNo ratings yet
- 2008 Physical Activity Guidelines: National Council On Strength & FitnessDocument2 pages2008 Physical Activity Guidelines: National Council On Strength & FitnessPaulo ZulluNo ratings yet
- Ch01.Intro To Phys Fit WellDocument24 pagesCh01.Intro To Phys Fit WellDREAM UPNo ratings yet
- Movement Enhancement 1: Module 7: Moderate and Vigorous Physical ActivitiesDocument8 pagesMovement Enhancement 1: Module 7: Moderate and Vigorous Physical ActivitiesMarjorie PolinarNo ratings yet
- Female Athlete TriadDocument29 pagesFemale Athlete TriadShimmering MoonNo ratings yet
- Exercise Testing and Prescription in Older AdultsDocument19 pagesExercise Testing and Prescription in Older Adultspushplata.19770No ratings yet
- Pe Lecture NotesDocument7 pagesPe Lecture NotesAnonymous LJrX4dzNo ratings yet
- The Benefits of Physical Activity UploadDocument17 pagesThe Benefits of Physical Activity UploadDorart IsmajliNo ratings yet
- Exercise and Cardiovascular HealthDocument2 pagesExercise and Cardiovascular HealthsynysterbraveNo ratings yet
- Exercise Prescription Certificate Course: Exercise Recommenda2ons For Persons With Special NeedsDocument59 pagesExercise Prescription Certificate Course: Exercise Recommenda2ons For Persons With Special NeedsThe Health Therapist AcademyNo ratings yet
- Dry Lab Exercise 4 EndocrineDocument4 pagesDry Lab Exercise 4 Endocrine06Fajrian RidhatunnisaNo ratings yet
- AAAAA - Family Developmental TaskDocument2 pagesAAAAA - Family Developmental TaskMaevan BacolNo ratings yet
- EU Approved Units EIA - MaharashtraDocument7 pagesEU Approved Units EIA - MaharashtragibinkumarNo ratings yet
- Container Data UtilizationDocument2,910 pagesContainer Data UtilizationCege Wa NjorogeNo ratings yet
- AVTC 5 - 09 - Group 3 - Business PlanDocument9 pagesAVTC 5 - 09 - Group 3 - Business Planda zelNo ratings yet
- TFN Reviewer PrelimsDocument8 pagesTFN Reviewer PrelimsCUBILLAS, JASMIN G.No ratings yet
- Alumunium Chlorohydrate: Material Safety Data SheetDocument4 pagesAlumunium Chlorohydrate: Material Safety Data Sheethinur awaNo ratings yet
- Mine? ? ??Document16 pagesMine? ? ??Samskruthi ChallaNo ratings yet
- QuestionDocument5 pagesQuestionJavy mae masbateNo ratings yet
- 4 Van Der Linden Et Al. (2020) Inoculating Against Fake NewsDocument7 pages4 Van Der Linden Et Al. (2020) Inoculating Against Fake Newsegenaz tunçdemirNo ratings yet
- Pe9 - q1 - Mod1 - Physical Activity and Physical Fitness Assessments - v3Document11 pagesPe9 - q1 - Mod1 - Physical Activity and Physical Fitness Assessments - v3JaysonMananquilLabsanNo ratings yet
- Benzofurano-Isatins: Search For Antimicrobial Agents: Arabian Journal of ChemistryDocument8 pagesBenzofurano-Isatins: Search For Antimicrobial Agents: Arabian Journal of Chemistrylucian_lovNo ratings yet
- Meaning of Self-Esteem: by Dr. Ranjit Singh MalhiDocument2 pagesMeaning of Self-Esteem: by Dr. Ranjit Singh Malhieva pandanaNo ratings yet
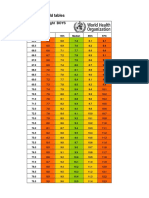
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet
- CMR 00062-17Document78 pagesCMR 00062-17pokhara144No ratings yet
- Material Safety Data Sheet Avades 100Document4 pagesMaterial Safety Data Sheet Avades 100fs1640No ratings yet
- Tatalaksana Oftalmia Neonatorum Ec Infeksi Gonokokal Dengan Ikterik Neonatorum - Viora Rianda PiscalokaDocument12 pagesTatalaksana Oftalmia Neonatorum Ec Infeksi Gonokokal Dengan Ikterik Neonatorum - Viora Rianda Piscalokasupaidi97No ratings yet
- List of Empanelled Hospitals & Diagnostic Centres DGEHSDocument33 pagesList of Empanelled Hospitals & Diagnostic Centres DGEHSaaryan0% (2)
- ABI Worksheet: Patient Name: Patient ID: DateDocument2 pagesABI Worksheet: Patient Name: Patient ID: Datezaqqi ubaidillahNo ratings yet
- Print Boarding PassDocument2 pagesPrint Boarding PassAshu SinghNo ratings yet
- Các Thì C A Đ NG TDocument3 pagesCác Thì C A Đ NG TThanh TuyếtNo ratings yet
- Cumulative Adversity As A Correlate of Posttraumatic GrowthDocument20 pagesCumulative Adversity As A Correlate of Posttraumatic GrowthLorena RodríguezNo ratings yet
- E-Cigarette Wholesale Distributor in USA - Vape Supplier in USADocument10 pagesE-Cigarette Wholesale Distributor in USA - Vape Supplier in USAAnjum JohnNo ratings yet
- Ca1 PrelimDocument60 pagesCa1 PrelimAira EspleguiraNo ratings yet
- TESTS DISEASES OF BLOOD AND ENDOCRINE SYSTEM Methodical Manual For The 5 Year PDFDocument152 pagesTESTS DISEASES OF BLOOD AND ENDOCRINE SYSTEM Methodical Manual For The 5 Year PDFMayur WakchaureNo ratings yet
- Citizens Civil Complaint Against Pittsfield, Cell TowerDocument65 pagesCitizens Civil Complaint Against Pittsfield, Cell ToweriBerkshires.comNo ratings yet
- Common Errors in Dental RadiographyDocument48 pagesCommon Errors in Dental RadiographyDarwin D. J. LimNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
- Green Gradient Monotone Minimalist Presentation TemplateDocument20 pagesGreen Gradient Monotone Minimalist Presentation TemplateJo-ann AguirreNo ratings yet