You might also like
- CIBIL Score & ReportDocument20 pagesCIBIL Score & ReportKumar GowdaNo ratings yet
- PDFDocument1 pagePDFharessh100% (1)
- Digit Private Car Liability Only Policy ScheduleDocument2 pagesDigit Private Car Liability Only Policy ScheduleVishvkumar patelNo ratings yet
- Consented Consumer Credit Report SummaryDocument3 pagesConsented Consumer Credit Report Summaryrazzak kathatNo ratings yet
- Tata Fixed Deposit FormDocument4 pagesTata Fixed Deposit Formkirang gandhi0% (1)
- MCA21 - Company Master DetailsDocument1 pageMCA21 - Company Master DetailsHimanshu ThakkarNo ratings yet
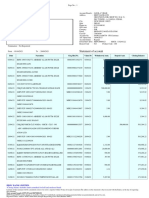
- AccountStatement - 06 DEC 2022 - To - 06 JUN 2023Document7 pagesAccountStatement - 06 DEC 2022 - To - 06 JUN 2023hancyboxNo ratings yet
- Iec Certificate Aagcb5911jDocument1 pageIec Certificate Aagcb5911jNagi ReddyNo ratings yet
- Y3 and Personal Data Form 2Document5 pagesY3 and Personal Data Form 2Shakil AhmedNo ratings yet
- Bank Statement FinalDocument1 pageBank Statement Finalshem dennisNo ratings yet
- Your CIBIL Score Where You StandDocument50 pagesYour CIBIL Score Where You StandApoorva kNo ratings yet
- Acct Statement XX4381 19122022Document31 pagesAcct Statement XX4381 19122022abhilash kondapuramNo ratings yet
- CPR 2022 Tax ReturnDocument1 pageCPR 2022 Tax ReturnUmair MughalNo ratings yet
- Coj 2017-09-05 551970573Document3 pagesCoj 2017-09-05 551970573Benny BerniceNo ratings yet
- HDFC Bank statement for Javed AliDocument3 pagesHDFC Bank statement for Javed AliNew NewNo ratings yet
- Wells Fargo Everyday CheckingDocument5 pagesWells Fargo Everyday CheckingTrish HitNo ratings yet
- Tax Invoice/bill of Supply/Cash Memo: This Is A Computer Generated Invoice and Does Not Require A Physical SignatureDocument1 pageTax Invoice/bill of Supply/Cash Memo: This Is A Computer Generated Invoice and Does Not Require A Physical SignatureAnonymous ythVLOyX6lNo ratings yet
- Account StatementDocument65 pagesAccount StatementBASHA SHAFIQNo ratings yet
- Manage finances online with this bank account statementDocument7 pagesManage finances online with this bank account statementphani sagarNo ratings yet
- Employer-Employee Proposal Form PDFDocument2 pagesEmployer-Employee Proposal Form PDFGD SinghNo ratings yet
- Statement of Account: HDFC Bank LimitedDocument1 pageStatement of Account: HDFC Bank LimitedPraveen Kumar MNo ratings yet
- Bill To / Ship To:: Qty Gross Amount Discount Other Charges Taxable Amount CGST SGST/ Ugst Igst Cess Total AmountDocument1 pageBill To / Ship To:: Qty Gross Amount Discount Other Charges Taxable Amount CGST SGST/ Ugst Igst Cess Total AmountPriya SinghNo ratings yet
- Account Statement For Account:0114002101107545: Branch DetailsDocument4 pagesAccount Statement For Account:0114002101107545: Branch DetailsHappy JainNo ratings yet
- Business Account Services ApplicationDocument9 pagesBusiness Account Services ApplicationZaccheus JulesNo ratings yet
- Statement of Account: From 01-APR-2020 To 31-MAR-2021Document2 pagesStatement of Account: From 01-APR-2020 To 31-MAR-2021debanwitaNo ratings yet
- Reliance Two Wheeler Package Policy - Schedule: Policy Number: 920222223121261091 Proposal/Covernote No: R01052205931Document6 pagesReliance Two Wheeler Package Policy - Schedule: Policy Number: 920222223121261091 Proposal/Covernote No: R01052205931MuraliMohanNo ratings yet
- Wright Express - Non Acquiring - MemphisDocument8 pagesWright Express - Non Acquiring - MemphisShashi Mae BonifacioNo ratings yet
- NPS Registration Form GuideDocument12 pagesNPS Registration Form GuidePascal ChhakchhuakNo ratings yet
- (05D)Document1 page(05D)Yosmell Fritzan Paz UrbizagasteguiNo ratings yet
- Customer PDFDocument2 pagesCustomer PDFSuraj BhandariNo ratings yet
- Sales Finance Loan Application Form: SalariedDocument6 pagesSales Finance Loan Application Form: SalariedKrishna KumarNo ratings yet
- 1.11091338 - 12 Mar 2013Document5 pages1.11091338 - 12 Mar 2013Deepak KumarNo ratings yet
- Concentrix Daksh Services India Private Limited Payslip For The Month of September - 2021Document1 pageConcentrix Daksh Services India Private Limited Payslip For The Month of September - 2021Prity PandeyNo ratings yet
- Jyoti Joshi HDFCDocument3 pagesJyoti Joshi HDFCJyoti JoshiNo ratings yet
- 0ad101670000001001658 ESTATEMENT 072022 0ad1016700000010 PDFDocument3 pages0ad101670000001001658 ESTATEMENT 072022 0ad1016700000010 PDFLOL Comix Ltd.No ratings yet
- 6 Month Transaction BankDocument15 pages6 Month Transaction BankShravan KumarNo ratings yet
- Policy No 3005 - 117287654 - 01 - 000Document3 pagesPolicy No 3005 - 117287654 - 01 - 000Prakash ChoudharyNo ratings yet
- Anita Kumari's January 2022 bank statementDocument1 pageAnita Kumari's January 2022 bank statementHari OmNo ratings yet
- Anand 3Document15 pagesAnand 3C K ANANDNo ratings yet
- 01 Apr 2023 - 05 Apr 2023Document2 pages01 Apr 2023 - 05 Apr 2023SUJIT SINGHNo ratings yet
- HDFC Bank account statement for M/S. TRAVBAE INTERNATIONAL CORP from April 2018 to March 2019Document13 pagesHDFC Bank account statement for M/S. TRAVBAE INTERNATIONAL CORP from April 2018 to March 2019Fortuna Power TECHNOLOGYNo ratings yet
- MSME CertificateDocument1 pageMSME Certificateavadhut gadeNo ratings yet
- Statements 5957Document4 pagesStatements 5957spark johnsonNo ratings yet
- Canara - Epassbook - 2023-06-17 16:03:13.102279Document3 pagesCanara - Epassbook - 2023-06-17 16:03:13.102279hamidanwarbelinjaNo ratings yet
- ListDocument4 pagesListNathy FrometaNo ratings yet
- RPPL F 054 Easa Form 19Document8 pagesRPPL F 054 Easa Form 19Sohail KhalidNo ratings yet
- Date Transaction Description Amount (In RS.) : Card No: 0036 1135 XXXX 3831 AAN: 0001015340002833839Document2 pagesDate Transaction Description Amount (In RS.) : Card No: 0036 1135 XXXX 3831 AAN: 0001015340002833839Satish RengarajanNo ratings yet
- Enquiry Information: Commercial Credit Information ReportDocument31 pagesEnquiry Information: Commercial Credit Information ReportTHERELEK MACHINES PRIVATE LIMITEDNo ratings yet
- (Ddau Am (E (Ê$.) : (NN BM H$M'M WJVMZ Es Oñq - Q G DV© - MZ Ewëh$ HW$B Xo' Am (E WJVMZ Xo' (V (WDocument5 pages(Ddau Am (E (Ê$.) : (NN BM H$M'M WJVMZ Es Oñq - Q G DV© - MZ Ewëh$ HW$B Xo' Am (E WJVMZ Xo' (V (WDeepak DahiyaNo ratings yet
- IDFCFIRSTBankstatement 10004015952Document10 pagesIDFCFIRSTBankstatement 10004015952Rahul BhadoriaNo ratings yet
- Account statement for May-July 2022Document13 pagesAccount statement for May-July 2022Meherun Bibi100% (1)
- Udyam Registration CertificateDocument1 pageUdyam Registration Certificatesabir hussainNo ratings yet
- CreditReport Piramal - Gamer Singh - 2023 - 05!27!10!36!38.PDF 27-May-2023Document3 pagesCreditReport Piramal - Gamer Singh - 2023 - 05!27!10!36!38.PDF 27-May-2023srk singhNo ratings yet
- Account StatementDocument12 pagesAccount StatementSiva GanaNo ratings yet
- SIDS Health Care Pvt. LTD.: Payslip For January-2019Document1 pageSIDS Health Care Pvt. LTD.: Payslip For January-2019hitesh gandhiNo ratings yet
- Voucher 6Document1 pageVoucher 6John Matthew SilvanoNo ratings yet
- Request for a Business NumberDocument5 pagesRequest for a Business Numberrouzbeh1797No ratings yet
- Acct Statement - XX9566 - 04012023Document4 pagesAcct Statement - XX9566 - 04012023ANKIT SINGHNo ratings yet
- Abu Dhabi to Chennai flight booking confirmationDocument3 pagesAbu Dhabi to Chennai flight booking confirmationLate KillerNo ratings yet
- Proposal FormDocument7 pagesProposal FormHandloom WorldNo ratings yet
- BenefitIllustartion Early Cash Plan 15102022173146Document2 pagesBenefitIllustartion Early Cash Plan 15102022173146dharam singhNo ratings yet
- Advisor Contest OND-18Document14 pagesAdvisor Contest OND-18dharam singhNo ratings yet
- Nominee Change FormatDocument4 pagesNominee Change Formatdharam singhNo ratings yet
- Sip 1.5l Surbhi GargDocument2 pagesSip 1.5l Surbhi Gargdharam singhNo ratings yet
- Proposal Form SLICDocument4 pagesProposal Form SLICdharam singhNo ratings yet
- Benefit Illustration For: Policy Year Total Annualised Premiums Paid Till Date Guaranteed Special Surrender BenefitDocument1 pageBenefit Illustration For: Policy Year Total Annualised Premiums Paid Till Date Guaranteed Special Surrender Benefitdharam singhNo ratings yet
- Company Cancelled ChequeDocument1 pageCompany Cancelled Chequedharam singhNo ratings yet
- Parul Sharma BIpdfDocument2 pagesParul Sharma BIpdfdharam singhNo ratings yet
- Life Insurance Plan BenefitsDocument1 pageLife Insurance Plan Benefitsdharam singhNo ratings yet
- Sip 1.5l Surbhi GargDocument2 pagesSip 1.5l Surbhi Gargdharam singhNo ratings yet
- Life insurance plan for Mr. AggarwalDocument1 pageLife insurance plan for Mr. Aggarwaldharam singhNo ratings yet
- Best Fixed Deposit Rates from Top BanksDocument1 pageBest Fixed Deposit Rates from Top Banksdharam singhNo ratings yet
- Reya BI 25kDocument2 pagesReya BI 25kdharam singhNo ratings yet
- Manan Bansal BI 20kDocument2 pagesManan Bansal BI 20kdharam singhNo ratings yet
- Applicable To All Fcs of Agency ChannelDocument5 pagesApplicable To All Fcs of Agency Channeldharam singhNo ratings yet
- Benefit Illustration For Shriram Life Golden Premier Saver Plan 128N088V02Document2 pagesBenefit Illustration For Shriram Life Golden Premier Saver Plan 128N088V02dharam singhNo ratings yet
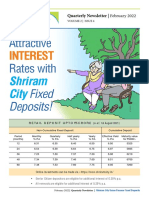
- Attractive Rates With: InterestDocument4 pagesAttractive Rates With: Interestdharam singhNo ratings yet
- Star Women Care Insurance Policy SummaryDocument2 pagesStar Women Care Insurance Policy Summarydharam singhNo ratings yet
- Dimension Group building commercial area coupon rating yield face value securitiesDocument1 pageDimension Group building commercial area coupon rating yield face value securitiesdharam singhNo ratings yet
- Key Features: Why SBI Life - Smart Champ Insurance Plan?Document2 pagesKey Features: Why SBI Life - Smart Champ Insurance Plan?dharam singhNo ratings yet
- D D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration FormDocument7 pagesD D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration Formdharam singhNo ratings yet
- To, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New BusinessDocument1 pageTo, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New Businessdharam singhNo ratings yet
- Educ 65 FinalsDocument73 pagesEduc 65 FinalsCarla Andrea QuilloNo ratings yet
- Total Body Lift SurgeryDocument224 pagesTotal Body Lift SurgeryI.M. Raluca IulianaNo ratings yet
- DR Ali Alanbaki MCQ MicrobiologyDocument14 pagesDR Ali Alanbaki MCQ MicrobiologyDr. noor taherNo ratings yet
- Nursing Association Diagnosis and Treatment GuideDocument40 pagesNursing Association Diagnosis and Treatment Guidemohammad odehNo ratings yet
- Hyperthyroidism in Sickle Cell AnaemiaDocument6 pagesHyperthyroidism in Sickle Cell AnaemiaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Nursing Care Plan Otitis MediaDocument3 pagesNursing Care Plan Otitis Mediaevi nur laili100% (2)
- K1 - Upper and Lower Resp System - Sindhu Wisesa - ReK1Document74 pagesK1 - Upper and Lower Resp System - Sindhu Wisesa - ReK1Dessy Dwi ZNo ratings yet
- Spine and Back Pain Treatment Without Surgery KKDocument6 pagesSpine and Back Pain Treatment Without Surgery KKMuhammed ANNo ratings yet
- NUR 205-Week 5 Pre Class Assignment WI 21Document6 pagesNUR 205-Week 5 Pre Class Assignment WI 21Oliver Namyalo100% (3)
- CHN 2018 RevisedDocument154 pagesCHN 2018 RevisedAubrey Unique EvangelistaNo ratings yet
- Compilation Liver Cirrhosis (4) - 1Document45 pagesCompilation Liver Cirrhosis (4) - 1Nagabharana Hm HollattiNo ratings yet
- Place a chest tubeDocument83 pagesPlace a chest tubehwelpNo ratings yet
- Butter Coffee Recipes - 48 Delic - Sam WharfDocument61 pagesButter Coffee Recipes - 48 Delic - Sam WharfOlivera Mihajlovic Tzanetou100% (1)
- Clinical Electro Physiological TestingDocument22 pagesClinical Electro Physiological TestingPaul VkNo ratings yet
- DM ExamDocument4 pagesDM Examyayooo2004100% (1)
- FAQCo WINforcitizensDocument5 pagesFAQCo WINforcitizensRaj AgrawalNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaIndah Pratiwii IriandyNo ratings yet
- Introduction of Acupuncture in Medical PracticeDocument49 pagesIntroduction of Acupuncture in Medical PracticeAnonymous 5IUoLwGSd100% (1)
- 1 Apple/day No Doctor 1 Tulsi Leaf/day No Cancer 1 Lemon /day No Fat 1 Cup Milk/day No Bone Prob 3 LTR Water A Day No DiseasesDocument1 page1 Apple/day No Doctor 1 Tulsi Leaf/day No Cancer 1 Lemon /day No Fat 1 Cup Milk/day No Bone Prob 3 LTR Water A Day No DiseasesAnkit YadavNo ratings yet
- Food Ideology2Document23 pagesFood Ideology2Patrick Larbi AwukuNo ratings yet
- History and Development of Community and Public HealthDocument49 pagesHistory and Development of Community and Public HealthCj LowryNo ratings yet
- MEGACOLONDocument19 pagesMEGACOLONstrumff1675% (4)
- Ijam 1Document5 pagesIjam 1Chakradhar ChakrreNo ratings yet
- Kuisioner SpiritualDocument9 pagesKuisioner SpiritualFirosika's HouseNo ratings yet
- Cracked Tooth SyndromeDocument49 pagesCracked Tooth SyndromeUzair Aftab100% (1)
- Right to Decide Funeral ArrangementsDocument7 pagesRight to Decide Funeral ArrangementsRechiel BagoodNo ratings yet
- Jurnal Pakai 4 (Edefinisi, Etiologi, Gejala, Diagnosis, Tatalaksana, Prognosis)Document10 pagesJurnal Pakai 4 (Edefinisi, Etiologi, Gejala, Diagnosis, Tatalaksana, Prognosis)Satrya DitaNo ratings yet
- 7 Drug StudyDocument17 pages7 Drug StudyMa. Mechile MartinezNo ratings yet
- Caterpillars and MothsDocument14 pagesCaterpillars and MothsIsabela IsazaNo ratings yet
- Blue Manila DigestDocument5 pagesBlue Manila DigestLenette LupacNo ratings yet