Professional Documents
Culture Documents
Traumatic Spinal Cord Injury 2018
Uploaded by
LEONARDO ANTONIO CASTILLO ZEGARRACopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Traumatic Spinal Cord Injury 2018
Uploaded by
LEONARDO ANTONIO CASTILLO ZEGARRACopyright:
Available Formats
Traumatic Spinal REVIEW ARTICLE
Cord Injury C O NT I N U U M A U D I O
I NT E RV I E W A V A I L AB L E
O NL I N E
By Alejandro A. Rabinstein, MD, FAAN
S U P P L E M E N T A L D I G I T AL
CONTENT (SDC)
ABSTRACT A V AI L A B L E O N L I N E
PURPOSE OF REVIEW: This article provides an update on the acute and subacute
management and prognostication of patients with traumatic spinal cord
injury.
RECENT FINDINGS: Immobilization of the spine and spine clearance should be
individualized depending on the ability to perform a reliable neurologic
examination, the presence of neck pain, and the imaging findings. Early
surgery (within 24 hours) to achieve definitive cord decompression and
spine stabilization may be beneficial. Ensuring adequate oxygenation and
perfusion and avoiding secondary systemic complications remain the goals
of the critical care of these patients. No neuroprotective treatment has
been shown to improve outcomes. In fact, the use of high-dose
methylprednisolone is now generally discouraged because of its major
systemic adverse effects. Survivors of severe cervical traumatic spinal
cord injury typically sustain substantial long-term functional impairment.
Advances in our understanding of neuroregenerative strategies, especially
stem cell transplantation, can offer the future hope of functional
improvement to the many patients currently living with the consequences
of traumatic spinal cord injury. Yet, at present, these therapies remain
strictly investigational. CITE AS:
CONTINUUM (MINNEAP MINN)
2018;24(2, SPINAL CORD DISORDERS):
SUMMARY: The treatment of traumatic spinal cord injury remains supportive, 551–566.
and prognosis is still poor for patients who are severely affected. While
Address correspondence to
much remains to be learned about how to optimize the acute management Dr Alejandro A. Rabinstein, Mayo
of these patients, future efforts would be most useful if focused on Clinic, Department of Neurology,
injury prevention and the development of effective neuroregenerative W8B, 200 1st St SW, Rochester,
MN 55905, rabinstein.
therapies. alejandro@mayo.edu.
RELATIONSHIP DISCLOSURE:
Dr Rabinstein has received
research/grant support from
INTRODUCTION DJO Global, Inc and receives
T
raumatic spinal cord injury is a serious and complex condition that publishing royalties from Elsevier,
Oxford University Press, and
requires a multidisciplinary approach. Neurologists, neurosurgeons,
UpToDate, Inc.
emergency physicians, intensivists, and rehabilitation specialists must
collaborate to optimize the management of these patients in the UNLABELED USE OF
PRODUCTS/INVESTIGATIONAL
acute, subacute, and chronic phases. Neurologists can be crucial for USE DISCLOSURE:
refined evaluation of the degree of clinical deficits, diagnosis and management of Dr Rabinstein reports no
acute and chronic complications, and estimation of prognosis. This article disclosure.
provides an updated review on traumatic spinal cord injury with a focus on © 2018 American Academy
what a neurologist should know about the condition. of Neurology.
CONTINUUMJOURNAL.COM 551
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
EPIDEMIOLOGY
The annual incidence of traumatic spinal cord injury in the United States has been
recently estimated at 54 cases per million population, representing approximately
17,000 new cases of traumatic spinal cord injury each year.1 Between 243,000 and
347,000 persons with traumatic spinal cord injury are currently living in the
United States. Many of these people are young, which causes staggering costs in
terms of loss of productivity. Although the average age of patients with traumatic
spinal cord injury has increased over the past few decades from 29 years in the 1970s
to 42 years at present, many patients are still younger than 30 years of age at the
time of the injury.1 Furthermore, some of the most severe cases of traumatic spinal
cord injury occur in this very young segment of the population.
Motor vehicle accidents remain the most common cause of traumatic spinal
cord injury (38%), especially among the young.1 Other frequent causes include
falls (particularly in the elderly; 31%), gunshot wounds and other forms of
violence (14%), and sports or other recreational activities (9%). Traumatic spinal
cord injury occurs predominantly in men (80%) and is overrepresented among
non-Hispanic blacks. Most injuries affect the cervical spinal cord, and an injury is
typically considered high cervical when it involves the cord above the C5 level. At
the time of discharge from the acute hospitalization, the most frequent degree of
injury is incomplete quadriplegia (45%), followed by incomplete paraplegia
(22%), complete paraplegia (20%), and complete quadriplegia (13%).1,2 Recent
trends indicate a growing proportion of incomplete injuries due to falls.2,3
Average expenses during the first year after the injury for a patient with high
quadriplegia can exceed $1 million. Lifetime expenses among young patients
with severe high-cervical traumatic spinal cord injury can top $4.5 million, even
without including indirect costs (eg, losses in wages, fringe benefits, and
productivity) and may average more than $70,000 per year.1
PATHOPHYSIOLOGY
The main mechanisms of primary injury to the spinal cord are direct impact with
persistent or transient compression, vertebral fracture and displacement, and cord
laceration or transection. Multiple classification systems have been proposed to
categorize cervical spine injuries, depending on the morphology of the bone damage,
disruption of the ligaments and intervertebral disks, and degree of neurologic
impairment.4 Flexion injuries can produce wedge fractures, vertebral subluxations,
and facet dislocations. Extension injuries can cause fractures of the posterior column
of the spine; less severe extension can provoke transient spinal cord compression in
patients with cervical spondylosis. Axial load injury can result in burst fractures of
cervical or thoracic vertebrae. Lacerations and transections are less frequent and occur
as a consequence of penetrating injuries. All these primary injuries are the direct
consequences of mechanical forces at the time of the injury (and over the following
hours in case of persistent compression) and are mostly not amenable to treatment.
The therapeutic focus in traumatic spinal cord injury is the avoidance and
correction of secondary injuries. Among them, early hypoxia and hypoperfusion
are currently the most correctable. However, animal models have elucidated
multiple mechanisms of secondary injury, including reperfusion, acute
inflammation, local swelling from intracellular and extracellular edema,
impaired vasomotor function, blood–spinal cord barrier disruption,
microhemorrhages, microthrombosis, excitotoxicity, mitochondrial damage,
lipid peroxidation, free radical formation, excessive intracellular calcium, and
552 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
activation of apoptotic signals.5 The cord swelling resulting from these acute KEY POINTS
secondary insults tends to peak after 3 to 6 days and subsides slowly over the
● Motor vehicle accidents
ensuing weeks. This acute phase appears to be followed by a progressive remain the most common
neurodegeneration mediated by persistent inflammation and characterized by cause of traumatic spinal
extensive microglial and astroglial activation.6 cord injury (38%), especially
among the young.
EVALUATION
● Most traumatic spinal
Physical examination in the field and upon arrival to the emergency department as cord injuries affect the
well as emergency spine imaging and immediate neck immobilization by the first cervical spinal cord, and an
responders are indispensable for any patient with suspected acute injury to the spine. injury is typically considered
high cervical when it
involves the cord above the
Clinical Assessment C5 level.
Early recognition of traumatic spinal cord injury in the field is crucial to avoid
additional cord damage during transportation. However, the early evaluation of ● The main mechanisms of
any patient with traumatic spinal cord injury should include a careful exclusion primary injury to the spinal
cord are direct impact with
of other serious injuries, such as to the head, chest, abdomen, and pelvis. In fact, cord compression, vertebral
traumatic brain injury is present in one-fourth to one-half of patients with fracture/dislocation,
traumatic spinal cord injury.7 and cord laceration
Patients with high-cervical traumatic spinal cord injury always present with or transection.
respiratory failure because of loss of diaphragmatic function. However, lower
● The therapeutic focus in
cervical and some upper thoracic injuries can also precipitate ventilatory failure traumatic spinal cord injury
either at presentation or later during the acute phase. These patients exhibit a is the avoidance and
typical breathing pattern known as quad breathing, manifested by inward motion correction of secondary
of the chest and outward motion of the abdomen with each inspiratory effort injuries, especially hypoxia
and hypoperfusion.
(the opposite of the paradoxical breathing pattern of patients with diaphragmatic
weakness) resulting from preserved diaphragmatic contraction and absent ● Cord swelling after
innervation of chest and abdominal muscles. trauma tends to peak
Cervical and upper thoracic injuries can cause refractory hypotension and after 3 to 6 days and
subsides slowly over the
bradycardia due to neurogenic shock (ie, loss of sympathetic outflow with ensuing weeks.
unopposed vagal activity). The severity of the neurologic impairment can
initially be exaggerated by spinal shock, a transient severe dysfunction of the ● Patients with
spinal cord that develops within the first hours after the injury and can last for high-cervical traumatic
spinal cord injury always
days or even a few weeks, typically manifesting with areflexic flaccid paralysis
present with respiratory
and anesthesia below the level of the lesion. These two phenomena can coexist failure because of loss of
but represent different consequences of traumatic spinal cord injury, and the two diaphragmatic function.
terms should not be used interchangeably.
A detailed neurologic examination is necessary to determine the level of the ● Cervical and upper
thoracic injuries can cause
injury and the severity of the neurologic impairment. The American Spinal Injury refractory hypotension
Association (ASIA) international standards are recommended as the preferred and bradycardia due to
tool to standardize the neurologic examination and classify the severity of the neurogenic shock.
injury.8 The complete examination worksheet can be freely accessed online and
● The severity of the
is included in this issue (SDC APPENDIX, links.lww.com/CONT/A245).9 The
neurologic impairment in
neurologic level of the injury is defined as the most caudal segment of the spinal traumatic spinal cord injury
cord with antigravity muscle strength (3/5 or better) and intact sensation (to light can initially be exaggerated
touch and pinprick) provided motor and sensory function are normal rostral by a temporary spinal shock.
to this level. In addition, motor and sensory levels should be determined on
each side of the body. Impairment is considered incomplete if some function is
preserved below the neurologic level of injury. Examination should include careful
evaluation to determine if any sacral function is spared, which can be manifested
by voluntary anal contraction, preserved tactile sensation in S4-S5 dermatomes,
CONTINUUMJOURNAL.COM 553
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
KEY POINTS or sensation to deep anal pressure. These assessments allow the stratification of
patients into five grades of neurologic impairment according to the ASIA Impairment
● The American Spinal
Injury Association
Scale.10 The ASIA grade of impairment has strong prognostic implications.11
international standards are When evaluating the degree of neurologic impairment, it is necessary to
recommended as the keep in mind that patients may initially appear worse because of spinal shock or
preferred tool to standardize worsen after presentation because of swelling. Thus, for prognostication
the neurologic examination
purposes, it is advisable to use the ASIA impairment grade determined at the
and classify the severity of
traumatic spinal cord injury. end of the initial hospitalization or at the beginning of the rehabilitation phase.
Certain specific syndromes that can be seen in patients with traumatic spinal
● The American Spinal cord injury deserve recognition. The central cord syndrome is caused by cord
Injury Association grade of contusion from buckling of the ligamentum flavum during neck hyperextension.
impairment has strong
prognostic implications for It is characterized by loss of cervical motor function with relative sparing of
traumatic spinal cord injury. strength in the legs because the motor fibers going to the arms are located more
medially within the descending corticospinal tracts. Patients with central cord
● The central cord syndrome syndrome may also experience a suspended sensory loss in cervicothoracic
is characterized by loss of
cervical motor function with
dermatomes. The Brown-Séquard syndrome is produced by hemisection of the
relative sparing of strength cord resulting in ipsilateral loss of proprioception and motor function and
in the legs. contralateral loss of pain and temperature sensation. Complete cord transection,
anterior cord syndrome (more common with spinal cord infarction), posterior
● The need for radiologic
cord syndrome (more common with infectious, metabolic, vascular, or
assessment of the spine
after trauma depends on the inflammatory causes or compression from an epidural mass), and conus or cauda
mental condition of the equina syndromes (more common with compression or infections) can also
patient, the presence of occur after trauma but much less frequently.
neck or back pain, and the
ability to perform a reliable
physical examination. Radiologic Assessment
The need for radiologic assessment of the spine after trauma depends on the
● High-quality CT scan is mental condition of the patient, the presence of neck or back pain, and the ability
the initial preferred imaging to perform a reliable physical examination.12 Evidence-based recommendations
modality after traumatic
spinal cord injury. MRI within
to guide the decision of when and how to image the cervical spine after trauma
the first 48 hours can help have been proposed by the Joint Section on Spine and Peripheral Nerves of
exclude ligamentous injury. the American Association of Neurological Surgeons and the Congress of
Neurological Surgeons, as outlined in TABLE 8-1.8
● MRI can reliably show the
The additional value of MRI in patients with no evidence of structural damage
extent of cord compression
and signs of cord injury. on high-quality CT remains controversial. MRI (including short tau inversion
recovery [STIR] sequences) can detect ligamentous injury that could explain
persistent pain and put the patient at risk for subluxation after mobilization of
the neck is allowed.13 However, ligamentous injury is best appreciated within
48 hours of the trauma and may not necessarily imply spinal instability, limiting
its value to guide discontinuation of the cervical collar.8
MRI can reliably show the extent of cord compression and signs of cord injury
(edema, hemisection, transection, hemorrhage, and, with less sensitivity,
ischemia) (FIGURE 8-1).13 These findings may help guide surgical decisions and
have prognostic implications.14 In the subacute and chronic phases, MRI can also
help explain rare cases of delayed decline caused by a syrinx or progressive
ascending myelomalacia.13 Newer MRI modalities, such as diffusion tensor
imaging, magnetic resonance spectroscopy, and functional MRI (fMRI) are being
investigated as techniques that could refine the ability to assess the integrity of
the cord at various stages after trauma.15
Some patients may have clinical signs and symptoms of spinal cord
dysfunction without any evidence of structural damage on CT. These cases of
554 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
spinal cord injury without radiologic abnormalities (SCIWORA) are more
common in children16 but can also be seen in adults.17 However, SCIWORA is
diagnosed based on the absence of abnormalities on x-rays and CT scan only.
MRI of the region of suspected injury or the entire spine is recommended in these
cases because it often (but not always) shows intraneural or extraneural
abnormalities. In these cases, prolonged immobilization (for 12 weeks) is
recommended, and spinal stability should be confirmed with delayed
flexion/extension x-rays before immobilization is discontinued.8
Recommendations for Cervical Spine Imaging and Cervical Immobilization TABLE 8-1
After Traumaa
Level of
Clinical Situation Recommendation Recommendation
Patient is alert and not intoxicated, is Cervical spine imaging is not recommended, and Level I
asymptomatic (no neck pain or tenderness), cervical immobilization can be discontinued
has normal neurologic examination, does not
have associated injuries that detract from his or
her general evaluation, and is able to complete
a functional range of motion examination
Patient is alert and symptomatic High-quality CT of the cervical spine is Level I
recommended
If high-quality CT is not available, a three-view
(anteroposterior, lateral, and odontoid views)
cervical spine x-ray series is recommended, but it
should be supplemented with CT if it becomes
available
If CT or three-view cervical spine series is normal, Level III
cervical immobilization should be continued until
one of the following conditions is met:
Patient becomes asymptomatic
Normal and adequate dynamic flexion and
extension x-raysb
Normal MRI within 48 hours of the injury
It is safe according to the treating physician
Patient is not alert or cannot be reliably High-quality CT of the entire spine (three-view Level I
evaluated cervical series and x-rays of lower spine if CT not
available followed by CT if it becomes available)
Discontinuation of cervical immobilization as Level III
stated for alert and symptomatic patients
CT = computed tomography; MRI = magnetic resonance imaging.
a
Data from Walters BC, et al, Neurosurgery.8
b
Lateral flexion-extension cervical x-rays must be performed under controlled conditions to ensure that the movement of the neck does not
exceed the point of worsening symptoms, and they must include the C7-T1 disk space.
CONTINUUMJOURNAL.COM 555
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
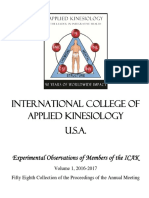
FIGURE 8-1
MRI of a young patient with lower cervical traumatic spinal cord injury with C5-C6 fracture
and dislocation with associated traumatic disk herniation and severe spinal cord
compression. Intramedullary signal change is seen on the sagittal T2-weighted image with
fat saturation (A) and more prominently appreciated on the sagittal short tau inversion
recovery (STIR) image (B). An axial T2-weighted image shows severe anterior compression
of the cord at the level of maximal displacement of the spinal elements (C) and extensive
intramedullary changes one level below (D).
TREATMENT
The therapeutic tenets of traumatic spinal cord injury include immobilizing the
spine; ensuring adequate ventilation, oxygenation, and perfusion; and
determining whether the patient needs surgical decompression.
Initial Stabilization and Medical Management
Providing adequate oxygenation is a major priority during the initial stabilization
phase after major trauma. When spinal injury is suspected, it is recommended
that the spine be immediately immobilized (with the sole exception of patients
556 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
with penetrating trauma, in whom any delay in resuscitation can be fatal),8 KEY POINTS
although the level of evidence supporting this widely accepted recommendation
● When spinal injury is
is not very strong.18 This is particularly important for patients with traumatic suspected, it is recommended
spinal cord injury who need tracheal intubation, because displacement of cervical that the spine be
spine elements can occur during this procedure. Consequently, patients with immediately immobilized.
suspected cervical traumatic spinal cord injury should have their necks manually
● Patients with suspected
stabilized in-line during tracheal intubation. Immobilization measures should traumatic spinal cord injury
include a rigid cervical collar, transportation on a rigid spine board, and should be transported to a
logrolling of the patient. When at all possible, patients with suspected traumatic specialized acute traumatic
spinal cord injury should be transported to a specialized acute traumatic spinal spinal cord injury treatment
center.
cord injury treatment center.8,19 Clearance of the cervical spine should then
proceed according to the recommendations outlined in TABLE 8-1. It is useful to ● The optimal timing of
remember that while immobilization of the spine can prevent serious secondary surgery for traumatic spinal
spinal cord damage in patients with spinal instability, its use is not devoid of cord injury has not been
conclusively established,
potential risks. Pain, pressure sores, airway compromise, increased risk of but prospective cohort
aspiration, and limitation of upper chest wall expansion can all be consequences studies suggest that
of cervical spine immobilization, particularly if prolonged. early intervention may
Avoiding hypoperfusion from systemic hypotension is also crucial. Patients be preferable.
with traumatic spinal cord injury can develop neurogenic shock with bradycardia
● Respiratory failure may
and reduced myocardial contractility due to loss of sympathetic innervation. occur at presentation or
Thus, a sympathetic agent with positive chronotropic and inotropic effects (such develop over the subsequent
as norepinephrine or epinephrine) is preferred to sustain the blood pressure. 5 days.
Also, other causes of shock that can occur after major trauma should be excluded,
● The duration of mechanical
such as active bleeding, pericardial tamponade, and tension pneumothorax. ventilation is typically
prolonged in patients with
Surgical Indications and Timing cervical traumatic spinal cord
The goals of spine surgery are decompression of neural elements with correction injury, but liberation from the
ventilator is possible in the
of deformities of the spinal canal, reduction of vertebral fractures, and fixation great majority of cases.
and fusion to ensure long-term spinal stability. Rapid closed reduction (to restore
spine alignment) is recommended for fracture and dislocation injuries until
the patient is taken to surgery.8
The optimal timing of surgery has not been conclusively established.
Prospective cohort studies favor early intervention.20 The largest among these
studies, the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS),
evaluated 313 patients and showed that those who underwent decompressive
surgery within 24 hours of the injury (mean 14.2 hours) were twice as likely to
have a two-grade improvement on the ASIA Impairment Scale at 6 months as
compared to patients undergoing surgery later (mean 48.3 hours).21 The Surgical
Treatment for Spinal Cord Injury study (SCI-POEM), another prospective
cohort study, is currently evaluating if surgery within 12 hours can be
beneficial.22 No randomized controlled trials have been conducted to address this
clinical question.
Critical Care
The critical care of patients with traumatic spinal cord injury is multifaceted and
demanding, but the respiratory and cardiovascular systems require the most
attention, particularly in the hyperacute phase.
RESPIRATORY MANAGEMENT. Respiratory failure after trauma can occur acutely
from injury to the brain, brainstem, or cervical spinal cord; secondary to
CONTINUUMJOURNAL.COM 557
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
aspiration; or because of airway obstruction. The diaphragm is innervated by the
C3-C5 roots and is the primary inspiratory muscle. Thus, complete injuries above
C3 inevitably cause acute ventilator failure in the field (CASE 8-1). When the
high-cervical cord lesion is partial or the level of injury is at C3 through C5,
ventilation can sometimes be maintained by accessory inspiratory muscles:
external intercostals (T1 through T11), sternocleidomastoids (cranial nerve XI),
trapezii (cranial nerve XI), and scalenes (C3 through C8). Although expiration
is normally driven by passive elastic recoil of the thoracic wall, patients with
severe trauma often depend on active expiration that requires the contraction
of the internal intercostal muscles (T1 through T11) and abdominal muscles
(T7 through L2). These anatomic considerations can help predict which
patients with traumatic spinal cord injury will be at higher risk of developing
respiratory failure and how likely they will be to remain dependent on
artificial ventilation. The development of respiratory failure is directly related to
the severity of the traumatic spinal cord injury as assessed by the ASIA
Impairment Scale.23
Patients with traumatic spinal cord injury who do not require immediate
mechanical ventilatory assistance often need it within the following 5 days.
Respiratory muscle fatigue, progressive atelectasis, accumulation of secretions
CASE 8-1 A 29-year-old woman with a history of type 1 diabetes mellitus and juvenile
rheumatoid arthritis was an unrestrained passenger when the car she
was riding in crashed and rolled over. She was found unconscious and
apneic by the paramedics who arrived promptly at the scene. She was
immediately intubated with manual in-line stabilization of the neck
and then transferred to a specialized trauma center with her spine
immobilized. On arrival to the emergency department, she was
hypotensive despite having received boluses of fluids, and she was also
bradycardic. Her hemodynamic parameters improved substantially after
initiation of a norepinephrine infusion. Her trauma survey was negative for
injuries to the head or elsewhere.
Examination showed flaccid quadriplegia with areflexia and complete
anesthesia below the neck. CT of her neck revealed fracture/dislocation at
the C2-C3 level with severe cord compression (FIGURE 8-2A). She underwent
closed reduction and was admitted to the neuroscience intensive care unit.
Her norepinephrine was adjusted to maintain a mean arterial pressure of
85 mm Hg to 90 mm Hg. Sixteen hours after the injury, she had surgical fusion
from C2 to C4. MRI of the cervical spine showed improvement of the cord
compression after the reduction but demonstrated extensive signs of cord
damage (FIGURES 8-2B and 8-2C). Except for atelectasis and pneumonia, her
intensive care unit course was uneventful. Her norepinephrine was weaned off
on day 7. She underwent tracheostomy and percutaneous gastrostomy on
day 8. As her spinal shock resolved, she regained some sensation below
the level of the injury and developed increased muscle tone in the
shoulders and upper chest. After slow weaning of the ventilator
assistance, she was liberated from the ventilator on day 42.
558 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
and mucous plugging due to ineffective cough, aspiration pneumonia,
pulmonary edema and pleural effusions after fluid resuscitation, and the direct
consequences of chest trauma may all contribute to respiratory failure.
Depending on the main causes, the respiratory failure may be hypoxemic,
hypercapnic, or—most commonly—mixed. When mechanical ventilation is
deemed necessary, intubation should not be delayed. Noninvasive ventilation has
a very limited role in the acute care of patients with traumatic spinal cord injury.
The duration of mechanical ventilation is typically prolonged in patients with
cervical traumatic spinal cord injury, but liberation from the ventilator is possible
in the great majority of cases.24 The duration of ventilator dependence depends
on the evolution of the neurologic deficits and whether major pulmonary
complications occur. As thoracic muscles go from flaccid to spastic, improvement
in chest wall stability may facilitate weaning. Yet, tracheostomy is often needed
in patients with poor ASIA motor scores.25 The optimal timing of tracheostomy is
not well defined. Patients with complete C1 to C3 cord injuries can sometimes
be liberated from the ventilator by means of diaphragmatic pacing.26
CARDIOVASCULAR MANAGEMENT. Aggressive treatment of hypotension during
the acute phase after the injury is associated with better outcomes in patients
FIGURE 8-2
Imaging of the patient in CASE 8-1. A, Sagittal reformatted CT shows a C2-C3 fracture with
severe dislocation compromising the spinal canal. After closed reduction, T2-weighted MRI
(B) and short tau inversion recovery (STIR) (C) show frank improvement of the dislocation
with some residual cord compression and clear evidence of spinal cord injury seen on the
T2-weighted image (B), but is better visualized on the STIR image (C).
This case illustrates the typical course of a young patient with severe upper COMMENT
cervical traumatic spinal cord injury causing respiratory failure and
neurogenic shock. Her cord compression was appropriately treated with
closed reduction followed by surgical decompression and fusion. The initial
examination was confounded by spinal shock, and her deficits improved
after this resolved, allowing for gradual liberation from the ventilator.
CONTINUUMJOURNAL.COM 559
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
KEY POINTS with traumatic spinal cord injury.27 Current guidelines recommend maintaining
a mean arterial pressure between 85 mm Hg and 90 mm Hg during the first week
● Current guidelines
recommend maintaining a
after the injury, although this recommendation is based on weak quality of
mean arterial pressure evidence.28 A recent study has shown that maintaining a spinal cord perfusion
between 85 mm Hg and pressure (ie, the difference between mean arterial pressure and CSF pressure
90 mm Hg during the first measured with an intrathecal catheter) above 50 mm Hg is associated with better
week after the injury,
functional outcomes.29 Achieving this mean arterial pressure goal very often
although the evidence
supporting this demands the use of vasopressors. Using agents with a1-adrenergic receptor and
recommendation is weak. b1-adrenergic receptor agonistic effects is advisable to correct the bradycardia
that accompanies hypotension from neurogenic shock. The risks of vasopressors
● Patients with traumatic should be carefully considered in each case, taking into consideration potential
spinal cord injury may have
multiple other complications deleterious consequences in other organs (including the brain in patients with
during their acute concomitant head injury).
hospitalization, but they
are mostly preventable. OTHER ASPECTS OF CRITICAL CARE. Patients with traumatic spinal cord injury
may have multiple other complications during their acute hospitalization, but
● No evidence currently
supports the use of any
they are mostly preventable (TABLE 8-2).30,31 Care in specialized units with
pharmacologic or intensivists, nurses, and physiatrists experienced in the management of patients
nonpharmacologic with traumatic spinal cord injury can minimize these risks. Neurologists can
interventions for contribute to the recognition and treatment of some of these complications, such
neuroprotection in patients
with traumatic spinal
as autonomic alterations, dysphagia, spasticity, pain, sphincter dysfunction, and
cord injury. mood disorders. Neurologists are also essential for the management of patients
with associated traumatic brain injury.
● Administration of
high-dose steroids can
produce major adverse NEUROPROTECTION. No evidence currently supports the use of any
effects in patients with pharmacologic or nonpharmacologic interventions for neuroprotection in
traumatic spinal cord injury patients with traumatic spinal cord injury. High-dose methylprednisolone was
and is not advisable. tested in the National Acute Spinal Cord Injury Study (NASCIS) trials.32,33 These
● Rigorous clinical trials are
trials showed higher rates of pneumonia, sepsis, acute respiratory distress
necessary to determine if syndrome, gastrointestinal hemorrhage, and death among patients treated with
therapeutic hypothermia corticosteroids. An association with modest improvement in motor outcome
can improve neurologic was only observed on a post hoc analysis restricted to patients treated within
outcomes in patients with
8 hours of the injury.34 Another randomized clinical trial that included a group
severe traumatic spinal
cord injury. of patients treated with methylprednisolone found no benefit in neurologic
outcomes at 1 year.35 Current guidelines do not recommend the use of
● The goals of rehabilitation corticosteroids for traumatic spinal cord injury.8
efforts for patients with Therapeutic hypothermia has shown promising results in translational studies
traumatic spinal cord injury
should be individualized to using local epidural or systemic cooling.36,37 However, no solid data exist to
achieve the patient’s fullest support its use in clinical practice. The Hypothermia Following Acute Spinal
physical, emotional, social, Cord Injury study, a prospective observational study with a planned size of
vocational, and functional 100 patients, is currently being conducted (NCT01739010),38 but no randomized
recovery.
studies are under way. Various pharmacologic agents are also being investigated
as possible neuroprotectants in traumatic spinal cord injury. They include
riluzole, minocycline, and fibroblast growth factor.5
REHABILITATION
The rehabilitation of patients with traumatic spinal cord injury starts in the
intensive care unit, and the neurologic and systemic complications observed
during the acute and rehabilitation phases frequently overlap. The goals of
rehabilitation efforts should be individualized to achieve the patient’s fullest
560 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Main Complications After Traumatic Spinal Cord Injury TABLE 8-2
Complication Prevention and Management
In the field
Spinal shock Preservation of adequate oxygenation and perfusion
Neurogenic shock Fluids and vasopressors
Respiratory failure Mechanical ventilation
In the hospital
Refractory shock Clarify mechanism(s), fluids and vasopressors
Respiratory failure Aggressive respiratory therapy, mechanical ventilation
Dysphagia Video swallowing, nasogastric tube/percutaneous gastrostomy
Infections Identify source, antibiotics
Venous thromboembolism Intermittent pneumatic compression, low-molecular-weight heparin, inferior vena
cava filter in some cases
Stress gastroduodenal ulcers Consider histamine 2 receptor blocker or proton pump inhibitor
In the rehabilitation unit (and beyond)
Autonomic dysreflexia Identify and avoid triggers
Orthostatic hypotension Compressive hoses, abdominal binder, midodrine (conservative dosing)
Pressure sores Meticulous surveillance of pressure spots, frequent mobilization, special bed when
available
Leg edema Leg elevation, compressive hose
Spasticity Physical therapy, baclofen, botulinum toxin injections
Chronic pain Physical therapy, analgesics and medications for neuropathic pain as pertinent
Temperature dysregulation Maintain stable room temperature
(“quad fever”)
Urinary retention Intermittent bladder catheterization
Constipation Cathartics
Obesity Caloric restriction
Heterotopic ossification Anti-inflammatory medications, bisphosphonates, local radiation
Renal stones (hypercalciuria) Hydration, monitoring and treatment of hypercalciuria
Sexual dysfunction Adjustment strategies
Depression and anxiety Psychotherapy, antidepressants as pertinent
Sleep disorders Sleep hygiene, control of pain and spasticity, melatonin, continuous positive airway
pressure if sleep breathing disorder with obstruction
CONTINUUMJOURNAL.COM 561
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
KEY POINTS physical, emotional, social, vocational, and functional recovery. Establishing
realistic goals and a feasible long-term plan to meet them is a crucial first step.
● Autonomic dysreflexia is
a common delayed
These goals will depend on the level and severity of injury, the age of the patient,
complication in patients and the presence of comorbidities.
with spinal cord injuries Mobilization, bowel and bladder training, and respiratory care can start before
above the T6 level and can transfer to the rehabilitation unit. Physical and occupational therapists will work
provoke sudden severe
with the patients on range of motion and strengthening exercises but also will
hypertension.
help manage edema in the extremities, recommend orthotic devices to provide
● The American Spinal support and prevent contractures, and train patients on the use of devices to
Injury Association Impairment assist their function (eg, different forms of functional electrical stimulation,
Scale grade, the level of electric wheelchairs, robotic systems for locomotor retraining, emerging
injury, and the appearance
of the cord on the MRI are brain-controlled neuroprostheses). Education of patients and families lies at the
the main prognostic core of this work.
indicators after traumatic Some of the most frequent complications during this phase are listed
spinal cord injury. in TABLE 8-2. Among them, autonomic dysreflexia can be particularly
● Mortality is highest within
problematic. Autonomic dysreflexia may occur in over half of patients with
the first 6 to 12 months cervical or high thoracic cord injuries (T6 or higher) and is especially common
after a traumatic spinal cord among patients with complete lesions; however, the degree of symptoms is
injury, but it remains higher highly variable, and in a sizable proportion of cases the diagnosis can only be
for patients with traumatic
made with certainty by using information from specific autonomic testing
spinal cord injury than in the
general population even (such as urodynamic studies).39 Manifestations of autonomic dysreflexia may
years later. emerge shortly after resolution of the initial spinal shock or, more often,
weeks or even months later (CASE 8-2). They result from unopposed
sympathetic discharge triggered by an intense stimulus below the level of the
lesion.39 Signs and symptoms include sudden hypertension, tachycardia or
reflex bradycardia, and severe headache. Patients may also have flushing,
sweating, and increased secretions above the level the lesion because of
compensatory increase in the parasympathetic tone. Meanwhile, below the
lesion, patients can exhibit piloerection and signs of vasoconstriction (pale, cool
limbs) from excessive sympathetic innervation. The main triggers of autonomic
dysreflexia include bladder distension, detrusor sphincter dyssynergia, fecal
impaction, and pressure sores. Identification and elimination of the precipitating
factor are the most effective treatment interventions. Hypertension can be very
severe and require specific treatment. Patients should be placed in an upright
sitting position, and, if medications are needed, short-acting direct vasodilators
(such as hydralazine) are preferred. Vasoactive medications should be dosed
conservatively because patients can react excessively to them, resulting in
sudden hypotension.
PROGNOSIS
The ASIA Impairment Scale grade, the level of injury, and the appearance of
the cord on MRI are the main prognostic indicators after traumatic spinal cord
injury.11,14,41–43 The Spinal Cord Independence Measure is the most recommended
tool to categorize the functional outcome and monitor the evolution of these
patients.8 This linear scale ranges from 0 to 100 and comprises sections on self-care
activities, respiratory function, bladder and bowel management, and mobility.44,45
However, many other disability scales with different characteristics and
relative advantages are also available.46
Mortality is highest within the first 6 to 12 months after the injury. The main
causes of death are respiratory failure, pulmonary embolism, cardiovascular
562 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
A 20-year-old man sustained a C5-C6 fracture dislocation with cord CASE 8-2
compression (FIGURE 8-3A) after a high-speed collision as an unrestrained
driver. He was admitted to a specialized trauma center where traction
reestablished spine realignment (FIGURE 8-3B). One day later, his spine
was stabilized with a C5 through T1 anterior fusion. He had persistent
deficits consistent with American Spinal Injury Association (ASIA)
Impairment Scale grade A at the C6 level. His acute course in the intensive
care unit included neurogenic shock treated with norepinephrine, sepsis
from pneumonia that resolved on antibiotics, and a deep venous
thrombosis in his leg that was managed with a combination of
anticoagulation with low-
molecular-weight heparin and
a retrievable inferior vena
cava filter.
Ten days after the accident,
he was transferred to the acute
rehabilitation unit. There he
started to have sudden
episodes of severe headache
associated with facial flushing
and severe hypertension. These
episodes were precipitated
by bladder or abdominal
distension. Typically, the
hypertension could be
controlled by having the FIGURE 8-3
patient sit upright, but Imaging of the patient in CASE 8-2. A,
occasionally it required Reformatted sagittal neck CT reveals a C5-C6
fracture-dislocation with complete distortion of
administration of a direct
the spinal canal that caused transection of the
vasodilator. Adjustments to the cord at that level. B, Sagittal T2-weighted
bladder and bowel program MRI obtained after closed reduction of the spine
progressively led to near demonstrates the extensive cord damage that had
resolution of these episodes. resulted from its originally severe compression.
This patient with a lower cervical cord injury had developed classic COMMENT
manifestations of autonomic dysreflexia. This complication is triggered by
stimulation below the level of the cord lesion (which the patient may not
feel because of anesthesia) that results in an exaggerated sympathetic
response that, in turn, provokes a compensatory increase of vagal
transmission. As a result, patients can develop signs and symptoms of
excessive parasympathetic tone above the cord lesion and excessive
sympathetic tone below the cord lesion. Sudden and sometimes extreme
hypertension is the most dangerous manifestation of this autonomic disorder.
CONTINUUMJOURNAL.COM 563
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
KEY POINT diseases, and sepsis.47 Early mortality is greater in older patients, those with high
cervical lesions, and those with the most severe neurologic deficits.11,48 Overall,
● Neuroregenerative
strategies, especially stem
the adjusted mortality of patients with traumatic spinal cord injury is up to 3
cell transplantation, are times higher than in the general population.42 Unfortunately, the life expectancy
promising but currently are of patients with traumatic spinal cord injury has not improved over the past
strictly investigational. few decades.1
It is estimated that only 12% of patients with traumatic spinal cord injury are
employed 1 year after the injury.1 This proportion increases over time, primarily
among young patients, but remains low nonetheless. Rehospitalizations are very
common (about 30% of patients in any given year). The main causes include
urinary infections, pressure sores, and a variety of other diagnoses.1
NEUROREGENERATION
The search for effective neuroregenerative strategies is undoubtedly the most
active area of research in the field of spinal cord injury. These strategies offer the
possibility of improvement in patients with chronic cord injury. Inhibitors of the
rho-associated protein kinase pathway (Rho/ROCK pathway) and enzymes that
degrade chondroitin sulfate proteoglycans are only some of the pharmacologic
strategies under investigation.5 However, cell-based therapies capture the most
attention. Transplantation of embryonic stem cells, induced pluripotent stem
cells, neural stem cells, mesenchymal stem cells, oligodendrocyte precursor cells,
Schwann cells, and olfactory ensheathing cells is the focus of acute research by
various teams across the world.5,49 At present, all these therapies remain
strictly investigational.
CONCLUSION
Trauma to the spinal cord remains a very serious condition with limited effective
therapies. Early and delayed mortality rates are still high, and survivors sustain
major functional impairments. Undoubtedly, injury prevention will always be
the most efficacious strategy to diminish the societal impact of this condition.
Once the injury has occurred, immediate attention to the prevention of hypoxia
and hypoperfusion and transportation to a center with experience in the
management of patients with traumatic spinal cord injury should be the
priorities. Currently, no proven strategies exist for neuroprotection, but
preservation of adequate oxygenation and perfusion and prevention of systemic
complications can improve outcomes. Advances in our understanding of the
molecular mechanisms preventing cord restoration after the trauma and a
growing knowledge of cell lines capable of facilitating cord healing have opened
windows for the development of neuroregenerative strategies. Collaborative
research and adequate funding may allow the discovery of an effective treatment
for patients with chronic spinal cord injuries in the future.
REFERENCES
1 National Spinal Cord Injury Statistical Center. 2 Devivo MJ. Epidemiology of traumatic spinal
Spinal cord injury: facts and figures at a glance. cord injury: trends and future implications.
https://www.nscisc.uab.edu/Public/Facts% Spinal Cord 2012;50(5):365–372. doi:10.1038/
20and%20Figures%20-%202017.pdf. Updated 2017. sc.2011.178.
Accessed January 29, 2018.
564 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
3 McCaughey EJ, Purcell M, McLean AN, et al. 16 Boese CK, Oppermann J, Siewe J, et al. Spinal
Changing demographics of spinal cord injury over cord injury without radiologic abnormality in
a 20-year period: a longitudinal population-based children: a systematic review and meta-analysis.
study in Scotland. Spinal Cord 2016;54(4):270–276. J Trauma Acute Care Surg 2015;78(4):874–882.
doi:10.1038/sc.2015.167. doi:10.1097/TA.0000000000000579.
4 Zhang S, Wadhwa R, Haydel J, et al. Spine and 17 Boese CK, Lechler P. Spinal cord injury without
spinal cord trauma: diagnosis and management. radiologic abnormalities in adults: a systematic
Neurol Clin 2013;31(1):183–206. doi:10.1016/j. review. J Trauma Acute Care Surg 2013;75(2):
ncl.2012.09.012. 320–330. doi:10.1097/TA.0b013e31829243c9.
5 Ahuja CS, Martin AR, Fehlings M. Recent advances 18 Oteir AO, Smith K, Stoelwinder JU, et al.
in managing a spinal cord injury secondary to Should suspected cervical spinal cord injury be
trauma. F1000Res 2016;5. pii:F1000 Faculty Rev-1017. immobilised?: a systematic review. Injury 2015;
doi:10.12688/f1000research.7586.1. 46(4):528–535. doi:10.1016/j.injury.2014.12.032.
6 Faden AI, Wu J, Stoica BA, Loane DJ. Progressive 19 Parent S, Barchi S, LeBreton M, et al. The impact of
inflammation-mediated neurodegeneration after specialized centers of care for spinal cord injury
traumatic brain or spinal cord injury. Br J Pharmacol on length of stay, complications, and mortality: a
2016;173(4):681–691. doi:10.1111/bph.13179. systematic review of the literature. J Neurotrauma
2011;28(8):1363–1370. doi:10.1089/neu.2009.1151.
7 Holly LT, Kelly DF, Counelis GJ, et al. Cervical spine
trauma associated with moderate and severe 20 Liu JM, Long XH, Zhou Y, et al. Is urgent
head injury: incidence, risk factors, and injury decompression superior to delayed surgery for
characteristics. J Neurosurg 2002;96(3 suppl): traumatic spinal cord injury? A meta-analysis.
285–291. doi:10.3171/spi.2002.96.3.0285. World Neurosurg 2016;87:124–131. doi:10.1016/j.
wneu.2015.11.098.
8 Walters BC, Hadley MN, Hurlbert RJ, et al.
Guidelines for the management of acute cervical 21 Fehlings MG, Vaccaro A, Wilson JR, et al. Early versus
spine and spinal cord injuries: 2013 update. delayed decompression for traumatic cervical spinal
Neurosurgery 2013;60(suppl 1):82–91. cord injury: results of the Surgical Timing in Acute
doi:10.1227/01.neu.0000430319.32247.7f. Spinal Cord Injury Study (STASCIS). PLoS One 2012;7
(2):e32037. doi:10.1371/journal.pone.0032037.
9 American Spinal Injury Association. International
Standards for Neurological Classification of 22 Clinicaltrials.gov website. Surgical treatment for
Spinal Cord Injury. asia-spinalinjury.org/wp-content/ spinal cord injury (SCI-POEM) (NCT01674764).
uploads/2016/02/International_Stds_Diagram_ clinicaltrials.gov/ct2/show/NCT01674764. Updated
Worksheet.pdf. Accessed January 29, 2018. April 4, 2017. Accessed January 29, 2018.
10 Maynard FMJr, Bracken MB, Creasey G, et al. 23 Stein DM, Menaker J, McQuillan K, et al. Risk
International Standards for Neurological and factors for organ dysfunction and failure in
Functional Classification of Spinal Cord Injury. patients with acute traumatic cervical spinal
American Spinal Injury Association. Spinal Cord cord injury. Neurocrit Care 2010;13(1):29–39.
1997;35(5):266–274. doi:10.1038/sj.sc.3100432. doi:10.1007/s12028-010-9359-9.
11 Wilson JR, Cadotte DW, Fehlings MG. Clinical 24 Jackson AB, Groomes TE. Incidence of
predictors of neurological outcome, functional respiratory complications following spinal cord
status, and survival after traumatic spinal cord injury. Arch Phys Med Rehabil 1994;75(3):
injury: a systematic review. J Neurosurg Spine 2012; 270–275. doi:10.1016/0003-9993(94)90027-2.
17(1 suppl):11–26. doi:10.3171/2012.4.AOSPINE1245.
25 Menaker J, Kufera JA, Glaser J, et al. Admission
12 Hoffman JR, Mower WR, Wolfson AB, et al. ASIA motor score predicting the need for
Validity of a set of clinical criteria to rule out tracheostomy after cervical spinal cord injury.
injury to the cervical spine in patients with blunt J Trauma Acute Care Surg 2013;75(4):629–634.
trauma. National Emergency X-Radiography doi:10.1097/TA.0b013e3182a12b86.
Utilization Study Group. N Engl J Med 2000;
26 Posluszny JA Jr, Onders R, Kerwin AJ, et al.
343(2):94–99. doi:10.1056/NEJM200007133430203.
Multicenter review of diaphragm pacing in spinal
13 Chandra J, Sheerin F, Lopez de Heredia L, et al. cord injury: successful not only in weaning from
MRI in acute and subacute post-traumatic spinal ventilators but also in bridging to independent
cord injury: pictorial review. Spinal Cord 2012; respiration. J Trauma Acute Care Surg 2014;76(2):
50(1):2–7. doi:10.1038/sc.2011.107. 303–309; discussion 309–310. doi:10.1097/
TA.0000000000000112.
14 Talbott JF, Whetstone WD, Readdy WJ, et al. The
Brain and Spinal Injury Center score: a novel, simple, 27 Casha S, Christie S. A systematic review of
and reproducible method for assessing the severity intensive cardiopulmonary management after
of acute cervical spinal cord injury with axial spinal cord injury. J Neurotrauma 2011;28(8):
T2-weighted MRI findings. J Neurosurg Spine 2015; 1479–1495. doi:10.1089/neu.2009.1156.
23(4):495–504. doi:10.3171/2015.1.SPINE141033.
28 Ryken TC, Hurlbert RJ, Hadley MN, et al. The acute
15 Ellingson BM, Salamon N, Holly LT. Imaging cardiopulmonary management of patients with
techniques in spinal cord injury. World Neurosurg cervical spinal cord injuries. Neurosurgery 2013;
2014;82(6):1351–1358. doi:10.1016/j.wneu.2012.12.004. 72(suppl 2):84–92. doi:10.1227/NEU.0b013e318276ee16.
CONTINUUMJOURNAL.COM 565
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TRAUMATIC SPINAL CORD INJURY
29 Squair JW, Bélanger LM, Tsang A, et al. Spinal 39 Curt A, Nitsche B, Rodic B, et al. Assessment of
cord perfusion pressure predicts neurologic autonomic dysreflexia in patients with spinal
recovery in acute spinal cord injury. Neurology cord injury. J Neurol Neurosurg Psychiatry 1997;
2017;89(16):1660–1667. doi:10.1212/ 62(5):473–477. doi:10.1136/jnnp.62.5.473.
WNL.0000000000004519.
40 Kirshblum SC, Priebe MM, Ho CH, et al. Spinal
30 Wuermser LA, Ho CH, Chiodo AE, et al. Spinal cord injury medicine. 3. Rehabilitation phase
cord injury medicine. 2. Acute care management after acute spinal cord injury. Arch Phys Med
of traumatic and nontraumatic injury. Arch Phys Rehabil 2007;88(3 suppl 1):S62–S70. doi:10.1016/
Med Rehabil 2007;88(3 suppl 1):S55–S61. doi:10. j.apmr.2006.12.003.
1016/j.apmr.2006.12.002. 41 Bozzo A, Marcoux J, Radhakrishna M, et al. The
31 Hagen EM. Acute complications of spinal cord role of magnetic resonance imaging in the
injuries. World J Orthop 2015;6(1):17–23. doi:10. management of acute spinal cord injury.
5312/wjo.v6.i1.17. J Neurotrauma 2011;28(8):1401–1411. doi:10.1089/
neu.2009.1236.
32 Bracken MB, Shepard MJ, Collins WF, et al. A
randomized, controlled trial of methylprednisolone 42 van den Berg ME, Castellote JM, de Pedro-Cuesta
or naloxone in the treatment of acute J, Mahillo-Fernandez I. Survival after spinal cord
spinal-cord injury. Results of the Second injury: a systematic review. J Neurotrauma 2010;
National Acute Spinal Cord Injury Study. N Engl J 27(8):1517–1528. doi:10.1089/neu.2009.1138.
Med 1990;322(20):1405–1411. doi:10.1056/ 43 Kaminski L, Cordemans V, Cernat E, et al. Functional
NEJM199005173222001. outcome prediction after traumatic spinal cord
injury based on acute clinical factors. J Neurotrauma
33 Bracken MB, Shepard MJ, Holford TR, et al.
2017;34(12):2027–2033. doi:10.1089/neu.2016.4955.
Administration of methylprednisolone for 24
or 48 hours or tirilazad mesylate for 48 hours 44 Catz A, Itzkovich M, Agranov E, et al.
in the treatment of acute spinal cord injury. SCIM—spinal cord independence measure: a
Results of the Third National Acute Spinal new disability scale for patients with spinal cord
Cord Injury Randomized Controlled Trial. lesions. Spinal Cord 1997;35(12):850–856.
National Acute Spinal Cord Injury Study.
JAMA 1997;277(20):1597–1604. doi:10.1001/ 45 Spinal Cord Injury Research Evidence website.
jama.1997.03540440031029. Spinal Cord Independence Measure (SCIM).
scireproject.com/outcome-measures/outcome-
34 Bracken MB. Steroids for acute spinal cord measure-tool/spinal-cord-independence-
injury. Cochrane Database Syst Rev 2012;1: measure-scim. Accessed January 29, 2018.
CD001046. doi:10.1002/14651858.CD001046.pub2.
46 Furlan JC, Noonan V, Singh A, Fehlings MG.
35 Pointillart V, Petitjean ME, Wiart L, et al. Assessment of disability in patients with acute
Pharmacological therapy of spinal cord injury traumatic spinal cord injury: a systematic review
during the acute phase. Spinal Cord 2000;38(2): of the literature. J Neurotrauma 2011;28(8):
71–76. doi:10.1038/sj.sc.3100962. 1413–1430. doi:10.1089/neu.2009.1148.
36 Wang J, Pearse DD. Therapeutic hypothermia in 47 Osterthun R, Post MW, van Asbeck FW, et al.
spinal cord injury: the status of its use and open Causes of death following spinal cord injury
questions. Int J Mol Sci 2015;16(8):16848–16879. during inpatient rehabilitation and the first five
doi:10.3390/ijms160816848. years after discharge. A Dutch cohort study.
Spinal Cord 2014;52(6):483–488. doi:10.1038/
37 Alkabie S, Boileau AJ. The role of therapeutic
sc.2014.28.
hypothermia after traumatic spinal cord
injury–a systematic review. World Neurosurg 48 Noe BB, Stapelfeldt CM, Parner ET, Mikkelsen
2016;86: 432–449. doi:10.1016/j. EM. Survival after traumatic spinal cord injury in
wneu.2015.09.079. Denmark: a hospital-based study among
patients injured in 1990–2012. Spinal Cord 2017;
38 Clinicaltrials.gov website. Hypothermia
55(4): 373–377. doi:10.1038/sc.2016.154.
following acute spinal cord injury (NCT01739010).
clinicaltrials.gov/ct2/show/NCT01739010. 49 Nagoshi N, Okano H. Applications of induced
Updated November 17, 2017. Accessed pluripotent stem cell technologies in spinal cord
January 29, 2018. injury. J Neurochem 2017. doi:10.1111/jnc.13986.
566 APRIL 2018
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- Clasificacion de Tumores Cerebreales de La OMS 2016 Articulo de RevisionDocument17 pagesClasificacion de Tumores Cerebreales de La OMS 2016 Articulo de RevisionSebastian SalvadorNo ratings yet
- Neuro Trauma PICDocument19 pagesNeuro Trauma PICNadir MonteroNo ratings yet
- Pulmonary EmbolismDocument28 pagesPulmonary EmbolismMaNiaaa LoxONo ratings yet
- Disorders of The Cauda EquinaDocument19 pagesDisorders of The Cauda Equinanight.shadowNo ratings yet
- Gunshot Wounds - Ballistic Trauma in The Emergency DepartmentDocument30 pagesGunshot Wounds - Ballistic Trauma in The Emergency DepartmentMulugeta DagneNo ratings yet
- Toxic Ingestions Pediatric EmergencyDocument24 pagesToxic Ingestions Pediatric EmergencyXimenaEspinaNo ratings yet
- Intracranial Pressure: Current Perspectives On Physiology and MonitoringDocument11 pagesIntracranial Pressure: Current Perspectives On Physiology and MonitoringCristian Andres Arancibia GomezNo ratings yet
- Updates and Controversies in The Early Management of Sepsis and Septic ShockDocument34 pagesUpdates and Controversies in The Early Management of Sepsis and Septic Shockdogui0071No ratings yet
- Multiple Sclerosis and Other Cns in Ammatory Diseases: Guest Editor: Dean M. Wingerchuk, MD, MSC, FRCPC, FaanDocument318 pagesMultiple Sclerosis and Other Cns in Ammatory Diseases: Guest Editor: Dean M. Wingerchuk, MD, MSC, FRCPC, FaanabelNo ratings yet
- Diabetic EmergenciesDocument24 pagesDiabetic EmergencieshabibfmNo ratings yet
- Procedural Sedation AnalgesiaDocument24 pagesProcedural Sedation Analgesiabenitez1228No ratings yet
- Review Course Vascular - AnaesthesiaDocument36 pagesReview Course Vascular - AnaesthesiazaidNo ratings yet
- HFNC Noninvasive VentilationDocument24 pagesHFNC Noninvasive VentilationAbody MenaNo ratings yet
- Jurnal FartokDocument195 pagesJurnal FartokMustafa RahmatillahNo ratings yet
- Ventilatory Targets Following Brain Injury: ReviewDocument9 pagesVentilatory Targets Following Brain Injury: ReviewAlan padilla sesmaNo ratings yet
- Practical: Invasive Mechanical VentilationDocument307 pagesPractical: Invasive Mechanical VentilationDayana CheriyanNo ratings yet
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDocument14 pagesOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhNo ratings yet
- 0822 Cardiac Valve EmergenciesDocument23 pages0822 Cardiac Valve EmergenciessarahmacielNo ratings yet
- Chest Tube SizeDocument10 pagesChest Tube SizeilpollolocoNo ratings yet
- Spinal Cord Anatomy and LocalizationDocument18 pagesSpinal Cord Anatomy and LocalizationJuanCarlosRiveraAristizabalNo ratings yet
- Blunt Cardiac InjuryDocument23 pagesBlunt Cardiac InjuryDaniel Cárdenas RojasNo ratings yet
- HSA ContinuunDocument35 pagesHSA ContinuunJose DavidNo ratings yet
- 0413 Massive Upper GI BleedingDocument12 pages0413 Massive Upper GI BleedingIsaura MendezNo ratings yet
- Libro VM Obeso 2018 PDFDocument305 pagesLibro VM Obeso 2018 PDFNataly Osorio MarínNo ratings yet
- Obstetric Life Support ManualDocument71 pagesObstetric Life Support Manualtf.jorgeNo ratings yet
- Surgical AirwaysDocument24 pagesSurgical AirwaysMed. TrackNo ratings yet
- Emergency Department Management of Acute Asthma ExacerbationsDocument32 pagesEmergency Department Management of Acute Asthma ExacerbationsFercho MedNo ratings yet
- TraducirChiasmal and Postchiasmal - DiseaseDocument19 pagesTraducirChiasmal and Postchiasmal - DiseasejacquelineNo ratings yet
- Advances in Emergent Airway Management in PediatricsDocument19 pagesAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNo ratings yet
- 1115 Ocular Injuries PDFDocument24 pages1115 Ocular Injuries PDFAndrea Valentina Villarroel BarriosNo ratings yet
- Vol 21.2 Neuro-Oncology.2015Document315 pagesVol 21.2 Neuro-Oncology.2015sammy_emerichNo ratings yet
- Secondary Fracture Prevention: An International PerspectiveFrom EverandSecondary Fracture Prevention: An International PerspectiveMarkus J. SeibelNo ratings yet
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDocument13 pages00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNo ratings yet
- Guide to multimodal brain monitoring techniques following traumatic brain injuryDocument12 pagesGuide to multimodal brain monitoring techniques following traumatic brain injuryConcepcion Jeronimo AguilarNo ratings yet
- Guia 2023 de Manejo de SdraDocument9 pagesGuia 2023 de Manejo de SdraBrian Antonio Veramatos LopezNo ratings yet
- Topical Issues in Anesthesia 2016Document207 pagesTopical Issues in Anesthesia 2016Ketzalzin DmgNo ratings yet
- Anesthesia and Perioperative Care For Organ Transplantation-Kathirvel Subramaniam, Tetsuro Sakai (Eds.) - ASpringer-Verlag New York (2017) - Repaired PDFDocument572 pagesAnesthesia and Perioperative Care For Organ Transplantation-Kathirvel Subramaniam, Tetsuro Sakai (Eds.) - ASpringer-Verlag New York (2017) - Repaired PDFmarcoNo ratings yet
- Antithrombotic Treatment of Acute Ischemic Stroke and Transient Ischemic Attack - UpToDateDocument24 pagesAntithrombotic Treatment of Acute Ischemic Stroke and Transient Ischemic Attack - UpToDateFerasNo ratings yet
- Pediatric Vascular Neurosurgery (Part 2)Document263 pagesPediatric Vascular Neurosurgery (Part 2)lailaakely.fisioNo ratings yet
- @medicalbook Store ShoDocument337 pages@medicalbook Store ShoAdriana LobatoNo ratings yet
- Major Incident Medical Management and Support: The Practical Approach at the SceneFrom EverandMajor Incident Medical Management and Support: The Practical Approach at the SceneNo ratings yet
- Review: Eduardo Tolosa, Alicia Garrido, Sonja W Scholz, Werner PoeweDocument13 pagesReview: Eduardo Tolosa, Alicia Garrido, Sonja W Scholz, Werner PoeweSaraNo ratings yet
- Intracerebral Hemorrhage TherapeuticsDocument12 pagesIntracerebral Hemorrhage TherapeuticsPedro Jerry Sevilla RomeroNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- 792Document527 pages792MarcNicaNo ratings yet
- Resident - Handbook - January 2016 - Final PDFDocument205 pagesResident - Handbook - January 2016 - Final PDFAliAlissa85No ratings yet
- Mecanical VentilationDocument433 pagesMecanical Ventilationmihaela popescuNo ratings yet
- Failed Spinal Anesthesia PDFDocument2 pagesFailed Spinal Anesthesia PDFShamim100% (1)
- Omnibus Risk EstimatorDocument6 pagesOmnibus Risk EstimatorranaNo ratings yet
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- Stoelting Pharmacology and Physiology 5th EditionDocument3 pagesStoelting Pharmacology and Physiology 5th EditionAsyur0% (1)
- MS4 Residency Survival GuideDocument202 pagesMS4 Residency Survival GuideShibb ShubbNo ratings yet
- Mood Disorders After TBIDocument17 pagesMood Disorders After TBIJaun CarrilloNo ratings yet
- CCCDocument487 pagesCCCSlaviša KovačevićNo ratings yet
- Diagnosis of Stupor and Coma-1-250!1!125Document125 pagesDiagnosis of Stupor and Coma-1-250!1!125Crhistian Andreé Cervantes CartagenaNo ratings yet
- Anaesthesia For Trauma PatientsDocument5 pagesAnaesthesia For Trauma Patientscahya candraNo ratings yet
- Idiopathic Intracranial HypertensionDocument21 pagesIdiopathic Intracranial HypertensionJorge Dornellys LapaNo ratings yet
- E148 FullDocument17 pagesE148 Fullpatricx10100% (1)
- Spinal Coding HandoutDocument66 pagesSpinal Coding HandoutagnaveenanNo ratings yet
- HNPDocument47 pagesHNPSyifa RabiahNo ratings yet
- Chapter 2 Science Form 4Document26 pagesChapter 2 Science Form 4Shafie Buyamin100% (2)
- Physio Uhs Solved Past Papers 2nd YearDocument126 pagesPhysio Uhs Solved Past Papers 2nd YearMudassar Roomi100% (3)
- Skeletal and Nervous SystemDocument50 pagesSkeletal and Nervous SystemDAKSHINA NAIRNo ratings yet
- Systematic Anatomy Final Exam Practice 2014Document9 pagesSystematic Anatomy Final Exam Practice 2014sammyNo ratings yet
- GPC Fractura VertebralDocument44 pagesGPC Fractura VertebralEdgar Vargas GranadosNo ratings yet
- Central Sulcus Separates The Following Two Lobes in The Cerebral CortexDocument8 pagesCentral Sulcus Separates The Following Two Lobes in The Cerebral CortexyoussefNo ratings yet
- International College of Applied Kinesiology USA (PDFDrive)Document241 pagesInternational College of Applied Kinesiology USA (PDFDrive)dvenumohan100% (3)
- Spondylodiscitis Severity Code: Scoring System For The Classification and Treatment of Non-Specific SpondylodiscitisDocument9 pagesSpondylodiscitis Severity Code: Scoring System For The Classification and Treatment of Non-Specific SpondylodiscitisEduardo RodriguezNo ratings yet
- Reception Response & Coordination-1Document116 pagesReception Response & Coordination-1jamesndong78No ratings yet
- Embryology Finals ReviewDocument53 pagesEmbryology Finals ReviewNdor BariboloNo ratings yet
- Oncologic Emergencies: Treatment, Structural Obstructions, and Metabolic ComplicationsDocument48 pagesOncologic Emergencies: Treatment, Structural Obstructions, and Metabolic ComplicationsStephen Joseph GarciaNo ratings yet
- Scientific Survey of The Yogic PosesDocument66 pagesScientific Survey of The Yogic PosesSnehal Kale100% (1)
- Neuroanatomy Questions GuideDocument19 pagesNeuroanatomy Questions GuideGoNo ratings yet
- What Are Spinal Tracts?Document2 pagesWhat Are Spinal Tracts?Ahsan JamilNo ratings yet
- 2ND Periodical Test in Science 6 With Tos KeyDocument9 pages2ND Periodical Test in Science 6 With Tos KeyJumaliza Francisco Paguirigan67% (3)
- Human Spinal Cord Picture C1 To S5 VertebraDocument3 pagesHuman Spinal Cord Picture C1 To S5 Vertebraajjju02No ratings yet
- Control of Posture & Movement-Blok15Document36 pagesControl of Posture & Movement-Blok15BonitavanyNo ratings yet
- Physiology JOHARIDocument165 pagesPhysiology JOHARIArrya DSNo ratings yet
- Anatomy and Physiology Chapter 19 Neurological SystemDocument38 pagesAnatomy and Physiology Chapter 19 Neurological SystemBrantNo ratings yet
- Bruce Frantzis - Learning Bagua (2010)Document23 pagesBruce Frantzis - Learning Bagua (2010)Scoala SolomonaraNo ratings yet
- 1-External Features of Spinal CordDocument24 pages1-External Features of Spinal Cordyaram3512No ratings yet
- Mechanism of Human BehaviorDocument7 pagesMechanism of Human BehaviorelkupiteroNo ratings yet
- Multiple Choice Questions: Traumatic Brain Injury: An Evidence-Based Review of ManagementDocument5 pagesMultiple Choice Questions: Traumatic Brain Injury: An Evidence-Based Review of Managementaftab alamNo ratings yet
- Unit 13 - Coordination and Response: Cambridge Biology iGCSEDocument58 pagesUnit 13 - Coordination and Response: Cambridge Biology iGCSEMirani R100% (1)
- AnaphyDocument8 pagesAnaphyCELLINA CLARISSE DE LEONNo ratings yet
- G6 Science LP W22 Q3Document7 pagesG6 Science LP W22 Q3Jubelaaa De RomaNo ratings yet
- Microcosmic OrbitDocument19 pagesMicrocosmic OrbitellemisteryNo ratings yet
- Kapandji - The Physiology of The Joints, Volume 3 - The Vertebral Column, Pelvic Girdle and HeadDocument345 pagesKapandji - The Physiology of The Joints, Volume 3 - The Vertebral Column, Pelvic Girdle and HeadGeo Sanchez100% (4)