You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Surgical Management of Giant Intracranial Meningiomas: Original ArticleDocument6 pagesSurgical Management of Giant Intracranial Meningiomas: Original ArticleAdel SalehNo ratings yet
- RG 256055137Document20 pagesRG 256055137Adel SalehNo ratings yet
- Pica Strok0Document1 pagePica Strok0Adel SalehNo ratings yet
- Book Reviews: Rang's Children's FracturesDocument1 pageBook Reviews: Rang's Children's FracturesAdel SalehNo ratings yet
- Karnofsky+Performance+Status+Scale+-+MDCalc 1654037194718Document3 pagesKarnofsky+Performance+Status+Scale+-+MDCalc 1654037194718Adel SalehNo ratings yet
- Clinical Importance of The Posterior Inferior Cerebellar Artery: A Review of The LiteratureDocument24 pagesClinical Importance of The Posterior Inferior Cerebellar Artery: A Review of The LiteratureAdel SalehNo ratings yet
- Neuroanatomy Q 1 - 7: EANS/UEMS European Examination in NeurosurgeryDocument14 pagesNeuroanatomy Q 1 - 7: EANS/UEMS European Examination in NeurosurgeryAdel Saleh100% (1)
- Physiology Stomatognathic SystemDocument19 pagesPhysiology Stomatognathic SystemDan 04No ratings yet
- Neoplasms of The LungDocument58 pagesNeoplasms of The LungLloyd Daniel BarrantesNo ratings yet
- Module 11. Pre-Natal DevelopmentDocument5 pagesModule 11. Pre-Natal DevelopmentRachel Joy SaldoNo ratings yet
- Head Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaDocument48 pagesHead Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaNinaNo ratings yet
- Rosenberg 1979Document6 pagesRosenberg 1979Aliénor VienneNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARINo ratings yet
- Neurological Health AssessmentDocument55 pagesNeurological Health Assessment09-bays-rhythmsNo ratings yet
- Q4 - Module 3 Consumer ChemistryDocument23 pagesQ4 - Module 3 Consumer Chemistryjessie100% (2)
- Computer Aided Brain Tumor Edge Extraction Using Morphological Op PDFDocument89 pagesComputer Aided Brain Tumor Edge Extraction Using Morphological Op PDFChitra VigneshNo ratings yet
- Neurologic AssessmentDocument29 pagesNeurologic AssessmentJoessel_Marie__8991100% (1)
- Endocrine of The Pancreas: Eman Alyaseen 20181081Document8 pagesEndocrine of The Pancreas: Eman Alyaseen 20181081ÂmoOł ÀhmdNo ratings yet
- BMI Priory Edgbaston Hospitals Consultant DirectoryDocument28 pagesBMI Priory Edgbaston Hospitals Consultant DirectorypsdsportsdocNo ratings yet
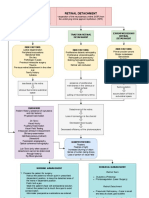
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- Neuro ImagingDocument12 pagesNeuro ImagingToby PearceNo ratings yet
- Ultrasound in Obstet Gyne - 2022 - PaladiniDocument8 pagesUltrasound in Obstet Gyne - 2022 - PaladiniKarim Muñoz NiñoNo ratings yet
- Assessment Explanation of The Problem Outcomes Interventions Rationale Evaluation STO: (Goal Met)Document2 pagesAssessment Explanation of The Problem Outcomes Interventions Rationale Evaluation STO: (Goal Met)Arian May MarcosNo ratings yet
- Blood Supply of Brain and Spinal Cord: W Prasasti Mutiadesi, DR., M. BiomedDocument26 pagesBlood Supply of Brain and Spinal Cord: W Prasasti Mutiadesi, DR., M. Biomedhelda dwianaNo ratings yet
- MID YEAR Assessment - SCIENCE10Document5 pagesMID YEAR Assessment - SCIENCE10anelou guingueNo ratings yet
- ASA Neuroaxial in Parturient With Intracranial PathologyDocument16 pagesASA Neuroaxial in Parturient With Intracranial PathologyKj BrionesNo ratings yet
- Seminar On Condylar Fractures - EDIT 1Document66 pagesSeminar On Condylar Fractures - EDIT 1Saranya MohanNo ratings yet
- Cerebrospinal Fluid (CSF) Sample RequirementsDocument7 pagesCerebrospinal Fluid (CSF) Sample RequirementsDr.Nouf alhasawiNo ratings yet
- Lab 12: A. General Sensation B. Special Senses Vision Hearing and EquilibriumDocument13 pagesLab 12: A. General Sensation B. Special Senses Vision Hearing and EquilibriumJAGDEV PANESARNo ratings yet
- 3-Pharynx. Diseases of NasopharynxDocument54 pages3-Pharynx. Diseases of NasopharynxislamNo ratings yet
- Sci 10 Week 3 Nervous SystemDocument17 pagesSci 10 Week 3 Nervous SystemNikkha elle Teleron100% (1)
- Psychology Module 1 &4Document49 pagesPsychology Module 1 &4John nyoikeNo ratings yet
- ACFrOgBz6SCL6SA VJUDh46tP6NUDhw3P47 NPjiCaRlywgh9trN 5PhQeKcHqMl2xUsHtUBcc7n4mL1On5SlTP2X94BYDVb HoGkGegg5erftVOvtVci7Q4s0omLCXYn6dldjBQhk2bZ6Jpfl6cDocument24 pagesACFrOgBz6SCL6SA VJUDh46tP6NUDhw3P47 NPjiCaRlywgh9trN 5PhQeKcHqMl2xUsHtUBcc7n4mL1On5SlTP2X94BYDVb HoGkGegg5erftVOvtVci7Q4s0omLCXYn6dldjBQhk2bZ6Jpfl6cMalavika A GNo ratings yet
- 7 Oragn SystemsDocument11 pages7 Oragn SystemsTobit Andre CaballoNo ratings yet
- All Your Advanced Analysis Needs One Comprehensive Solution: StartDocument185 pagesAll Your Advanced Analysis Needs One Comprehensive Solution: StartMitra MedistraNo ratings yet
- Aj CSF - Rhinorrhea - + - Nasal - Foreign - Body - + - Myiasis - + - ChoanalDocument63 pagesAj CSF - Rhinorrhea - + - Nasal - Foreign - Body - + - Myiasis - + - ChoanalTradigrade PukarNo ratings yet
- Lab 2 MC100Document3 pagesLab 2 MC100Aj MendozaNo ratings yet