You might also like
- Week 7. COURSE TASK - Case Study - Cushing SyndromeDocument5 pagesWeek 7. COURSE TASK - Case Study - Cushing SyndromeTerence SalamatNo ratings yet
- Cushing's Syndrome Is A Disorder That Occurs When Your Body Makes Too Much ofDocument6 pagesCushing's Syndrome Is A Disorder That Occurs When Your Body Makes Too Much ofIra C. SarapatNo ratings yet
- CushingDocument3 pagesCushingaiki parkNo ratings yet
- Understanding Cushing's Syndrome: Signs, Symptoms and DiagnosisDocument19 pagesUnderstanding Cushing's Syndrome: Signs, Symptoms and DiagnosisBitz Basos ViadoNo ratings yet
- Cushing SyndromeDocument15 pagesCushing Syndromeandrea.maungca.mnlNo ratings yet
- Week 5 Endokrin WO - Michael GeraldilDocument5 pagesWeek 5 Endokrin WO - Michael GeraldilMichael GNo ratings yet
- Cushing's Syndrome: Diagnosis, Treatment and Nursing CareDocument2 pagesCushing's Syndrome: Diagnosis, Treatment and Nursing CareCourtney HammonsNo ratings yet
- Group D Case Study Cushing SyndromeDocument6 pagesGroup D Case Study Cushing SyndromeMari IllustriousNo ratings yet
- Cushing-Syndrome SyndromeDocument16 pagesCushing-Syndrome SyndromeVanetNo ratings yet
- Cushing SyndromeDocument2 pagesCushing SyndromeKesyaNo ratings yet
- What is Cushing's syndrome? Causes, symptoms, and treatment of this hormonal disorderDocument10 pagesWhat is Cushing's syndrome? Causes, symptoms, and treatment of this hormonal disorderkuroroexileNo ratings yet
- Case Pre.. Cushing SyndromeDocument11 pagesCase Pre.. Cushing Syndromedee_day_8No ratings yet
- Cushing Syndrome Diagnostic TestsDocument12 pagesCushing Syndrome Diagnostic TestsJamaica Leslie NovenoNo ratings yet
- CUSHINGDocument17 pagesCUSHINGAfdhalia Khairunnisa SyammarhanNo ratings yet
- Cushing's SyndromeDocument68 pagesCushing's SyndromeKaye De Guzman, BSN - Level 3ANo ratings yet
- Hyper-cortisolism (Cushing Syndrome), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-cortisolism (Cushing Syndrome), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- CushingDocument4 pagesCushingavinash dhameriyaNo ratings yet
- Cushing Syndrome: M.Sc. (N) 1 YearDocument30 pagesCushing Syndrome: M.Sc. (N) 1 YearRanjana SharmaNo ratings yet
- Neurosurg Focus Article Pe4Document11 pagesNeurosurg Focus Article Pe4Asad ParvezNo ratings yet
- CushingDocument26 pagesCushingAlexSusantoNo ratings yet
- Dermatology: RoundsDocument6 pagesDermatology: RoundsPin Wijaya100% (1)
- What Is Cushing's Syndrome?Document9 pagesWhat Is Cushing's Syndrome?Nurul Shafiqah SafianNo ratings yet
- What Is Cushing's Syndrome?Document5 pagesWhat Is Cushing's Syndrome?Virza Chairunnisa LatuconsinaNo ratings yet
- Cushing's Treatment Depends on CauseDocument6 pagesCushing's Treatment Depends on CauseErico OoiNo ratings yet
- Cushings Syndrome and Addison Disease - BPTDocument45 pagesCushings Syndrome and Addison Disease - BPTAanchal GuptaNo ratings yet
- Cushing's SyndromeDocument24 pagesCushing's SyndromeUdtjeVanDerJeyk100% (1)
- REPORTDocument13 pagesREPORTEarlou MagbanuaNo ratings yet
- Cushing's Syndrome: HypercortisolismDocument22 pagesCushing's Syndrome: HypercortisolismA HNo ratings yet
- Cushing's Syndrome, Addison's Disease and Hyperparathyroidism.Document29 pagesCushing's Syndrome, Addison's Disease and Hyperparathyroidism.pranjl100% (1)
- Cushing SyndromeDocument19 pagesCushing SyndromerituNo ratings yet
- Case Study - Cushing's DiseaseDocument5 pagesCase Study - Cushing's DiseaseHoney1694No ratings yet
- HyperpituitarismDocument25 pagesHyperpituitarismBheru Lal0% (1)
- Endocrinology Course Content: Semester (5) Clinical Pharmacy CourseDocument91 pagesEndocrinology Course Content: Semester (5) Clinical Pharmacy CourseSadigMukhNo ratings yet
- Cushing'S Syndrome: PathophysiologyDocument7 pagesCushing'S Syndrome: PathophysiologyNorsida LailiNo ratings yet
- EndokrinDocument27 pagesEndokrinSarah Putri AbellysaNo ratings yet
- Diagnostic Tests For Cushing'sDocument6 pagesDiagnostic Tests For Cushing'sChristine ParrillaNo ratings yet
- RARE BILATERAL ADRENOCORTICAL ADENOMASDocument8 pagesRARE BILATERAL ADRENOCORTICAL ADENOMASJhuRise Ann ManganaNo ratings yet
- Case Study Cushing Syndrome 1Document5 pagesCase Study Cushing Syndrome 1Selena Marie100% (1)
- Cushings, Addisons and Acromegaly: DR J Storrow FY2Document38 pagesCushings, Addisons and Acromegaly: DR J Storrow FY2abdalkhalidNo ratings yet
- Cushing SyndromeDocument5 pagesCushing SyndromeRosa Yulise PutriNo ratings yet
- Uso de Esteroides en AnestesiaDocument7 pagesUso de Esteroides en AnestesiatitinodeNo ratings yet
- Addisons DiseaseDocument5 pagesAddisons DiseaseCrystal ManguneNo ratings yet
- Adrenal Fatigue Solution: Powerful Methods to Boost Your Energy, Improve Metabolism, And Stimulate Your HormonesFrom EverandAdrenal Fatigue Solution: Powerful Methods to Boost Your Energy, Improve Metabolism, And Stimulate Your HormonesNo ratings yet
- Cushings Addisons and Acromegaly EdDocument45 pagesCushings Addisons and Acromegaly EdAny PopNo ratings yet
- El Síndrome de Cushing: Sintomas de Enfermedad en Las PersonasDocument7 pagesEl Síndrome de Cushing: Sintomas de Enfermedad en Las PersonasAmilcar CaizaNo ratings yet
- Cushing DiseaseDocument24 pagesCushing DiseaseSuci AlimaNo ratings yet
- Drugs Affecting Endocrine SystemDocument28 pagesDrugs Affecting Endocrine SystemShion SimpNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Perioperative Corticosteroid Administration: Adel M. Bassily-Marcus, MD - Andrew B. Leibowitz, MDDocument6 pagesPerioperative Corticosteroid Administration: Adel M. Bassily-Marcus, MD - Andrew B. Leibowitz, MDEka NovitasariNo ratings yet
- Cushing SyndromeDocument9 pagesCushing SyndromealyakaramyNo ratings yet
- Cushings Addisons and Acromegaly EdDocument45 pagesCushings Addisons and Acromegaly Edsamehseef100% (1)
- Cushing SyndromeDocument25 pagesCushing Syndromeroland helmizarNo ratings yet
- Cushing2015 PDFDocument25 pagesCushing2015 PDFRoxana Ioana DumitriuNo ratings yet
- Back Pain and HypercortisolismDocument2 pagesBack Pain and HypercortisolismAlex CostaNo ratings yet
- 655 FullDocument16 pages655 FullGhina nurulNo ratings yet
- Progressive Muscle Weakness: More There Than Meets The Eye: Im Board ReviewDocument7 pagesProgressive Muscle Weakness: More There Than Meets The Eye: Im Board Reviewbdalcin5512No ratings yet
- Cushing's Syndrome: Excess Cortisol and Its CausesDocument3 pagesCushing's Syndrome: Excess Cortisol and Its CausesYoga KarsendaNo ratings yet
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
- Week 1 Critical Care Nursing. SlideDocument80 pagesWeek 1 Critical Care Nursing. SlideArmand Bong SantiagoNo ratings yet
- NCMB317: Week 2 RLE Theories in The Care Patients With Maladaptive BehaviorDocument5 pagesNCMB317: Week 2 RLE Theories in The Care Patients With Maladaptive BehaviorArmand Bong Santiago100% (1)
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
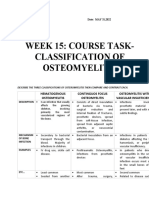
- OSTEOMYELITISDocument2 pagesOSTEOMYELITISArmand Bong Santiago100% (1)
- NCBM317: Week 15Document2 pagesNCBM317: Week 15Armand Bong Santiago100% (2)
- NCMB317: Shared Psychotic DisorderDocument21 pagesNCMB317: Shared Psychotic DisorderArmand Bong Santiago100% (1)
- NCMB317 LECTURE Cu 3 Week 3 Lec SchizophreniaDocument3 pagesNCMB317 LECTURE Cu 3 Week 3 Lec SchizophreniaArmand Bong Santiago100% (1)
- NCMB317 AutismDocument1 pageNCMB317 AutismArmand Bong Santiago100% (1)
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- NCMB 317 AdhdDocument14 pagesNCMB 317 AdhdArmand Bong Santiago100% (1)
- NCMB317: RupturedDocument12 pagesNCMB317: RupturedArmand Bong Santiago100% (1)
- NCMB 317: Mental Health and IllnessDocument52 pagesNCMB 317: Mental Health and IllnessArmand Bong SantiagoNo ratings yet
- NCMB316: Compilation Finals in NCMB316Document23 pagesNCMB316: Compilation Finals in NCMB316Armand Bong Santiago100% (1)
- NCMB316 Cu1 DiscussionDocument1 pageNCMB316 Cu1 DiscussionArmand Bong Santiago100% (1)
- NCMB316 Week 7 InfographicsDocument2 pagesNCMB316 Week 7 InfographicsArmand Bong Santiago100% (1)
- Case StudyDocument16 pagesCase StudyArmand Bong Santiago100% (1)
- NCMB 316: Week 1 Course Unit 1Document3 pagesNCMB 316: Week 1 Course Unit 1Armand Bong Santiago100% (1)
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- NCMB 316 (Case Study Cholecystitis Cholelithiasis Disease)Document27 pagesNCMB 316 (Case Study Cholecystitis Cholelithiasis Disease)Armand Bong Santiago100% (2)
- Plagiarism Checker X Originality Report: Similarity Found: 24%Document5 pagesPlagiarism Checker X Originality Report: Similarity Found: 24%DonaldNo ratings yet
- Materi DR Aziza Ariyani SP - PKDocument92 pagesMateri DR Aziza Ariyani SP - PKArgadia YuniriyadiNo ratings yet
- NegOr Q4 EAPP Module8 v2Document20 pagesNegOr Q4 EAPP Module8 v2XYZA LopezNo ratings yet
- Kejadian Plebitis Bulan April 2019Document326 pagesKejadian Plebitis Bulan April 2019Ridho YulfiahNo ratings yet
- Energy Expenditure and FatigueDocument49 pagesEnergy Expenditure and FatigueAh Zhang100% (1)
- المعدات وغرف الانتاج والتنظيف والصيانة دليل الطالبDocument56 pagesالمعدات وغرف الانتاج والتنظيف والصيانة دليل الطالبbionorluxeNo ratings yet
- This Study Resource Was: Running Head: Merck & Company 1Document6 pagesThis Study Resource Was: Running Head: Merck & Company 1vijay SinghNo ratings yet
- Colles FractureDocument5 pagesColles FractureKimbraPataraNo ratings yet
- An Introduction To API 653 PDFDocument14 pagesAn Introduction To API 653 PDFGiorgi KOGOSHVILINo ratings yet
- Empirical Treatment of Sepsis in AdultsDocument11 pagesEmpirical Treatment of Sepsis in AdultsMarnia SulfianaNo ratings yet
- PCL Tears: Causes, Symptoms and Treatment of Posterior Cruciate Ligament InjuriesDocument2 pagesPCL Tears: Causes, Symptoms and Treatment of Posterior Cruciate Ligament InjuriesklebetNo ratings yet
- Philippe L. de Coster - Meditation and SexDocument11 pagesPhilippe L. de Coster - Meditation and SexArcanistNo ratings yet
- Penerapan Model Pembelajaran Problem Based Learning Untuk Meningkatkan Hasil Belajar Siswa Mata Pelajaran PAK Di Kelas V SDN 003 Bintan TimurDocument12 pagesPenerapan Model Pembelajaran Problem Based Learning Untuk Meningkatkan Hasil Belajar Siswa Mata Pelajaran PAK Di Kelas V SDN 003 Bintan Timurrony carolesNo ratings yet
- Prism 3 L&S-51-100Document50 pagesPrism 3 L&S-51-100bui thangNo ratings yet
- CSU Cannabis ConferenceDocument2 pagesCSU Cannabis ConferenceD Plump ConsultingNo ratings yet
- Anna University Industrial Relations Question Bank BA7034Document45 pagesAnna University Industrial Relations Question Bank BA7034Shupiksha LoganathanNo ratings yet
- Beyond The Confinement of Afßiction: A Discursive Field of ExpérienceDocument6 pagesBeyond The Confinement of Afßiction: A Discursive Field of ExpérienceAnnachiara ForteNo ratings yet
- Diurinal VariationDocument5 pagesDiurinal VariationKEERTIMAAN JOSHINo ratings yet
- ICPR 5 1 WebDocument96 pagesICPR 5 1 WebAndreea-Luciana UrzicăNo ratings yet
- Celebrating Our Newest LeadersDocument42 pagesCelebrating Our Newest LeadersBaptist Memorial Health CareNo ratings yet
- MDD Classification Document: Mapping of RequirementsDocument12 pagesMDD Classification Document: Mapping of Requirementsdhir.ankurNo ratings yet
- BUS 5113 - Motivation TheoriesDocument5 pagesBUS 5113 - Motivation TheoriesEzekiel PatrickNo ratings yet
- CPDprogram MEDTECH-101518Document187 pagesCPDprogram MEDTECH-101518PRC Board0% (1)
- Best Practices For EconomistsDocument4 pagesBest Practices For EconomistsMahlatse MabebaNo ratings yet
- Breaking Free From AddictionsDocument9 pagesBreaking Free From AddictionslivromeoNo ratings yet
- Councillor Danny Thorpe: Leader, Royal Borough of GreenwichDocument2 pagesCouncillor Danny Thorpe: Leader, Royal Borough of GreenwichDr-Syed Ali TarekNo ratings yet
- Research EssayDocument12 pagesResearch Essayapi-608972617No ratings yet
- ProspectusDocument14 pagesProspectusJawad KhanNo ratings yet
- SHS Student Handbook 2023 Ed v2Document154 pagesSHS Student Handbook 2023 Ed v2Alvin Xtian NucumNo ratings yet