You might also like
- To Improve Our Holistic BeingDocument2 pagesTo Improve Our Holistic BeingDonna Villafuerte RamosNo ratings yet
- Reflective EssayDocument7 pagesReflective EssayJEA MARIE MENDOZANo ratings yet
- NCMB 316: Week 1 Course Unit 1Document3 pagesNCMB 316: Week 1 Course Unit 1Armand Bong Santiago100% (1)
- Ca Copd (Emphysema)Document42 pagesCa Copd (Emphysema)Charisse CaydanNo ratings yet
- Catatonic Schizophrenia - Case StudyDocument11 pagesCatatonic Schizophrenia - Case StudyKrizzia Louise B. CabreraNo ratings yet
- Iv Therapy With Edited RationaleDocument5 pagesIv Therapy With Edited RationaleKysha HuangNo ratings yet
- A. Ideational LearningDocument2 pagesA. Ideational LearningSherish Millen CadayNo ratings yet
- Subjective Data-Health AssessmentDocument2 pagesSubjective Data-Health AssessmentQueen RiquezNo ratings yet
- Complete Ca1 Prelim ReviewersDocument37 pagesComplete Ca1 Prelim ReviewersANDREW DEL ROSARIONo ratings yet
- Electronic Gadgets Restrains The Children Social Interaction.Document40 pagesElectronic Gadgets Restrains The Children Social Interaction.David Dhea Refazo LinatokNo ratings yet
- War of DrugsDocument18 pagesWar of DrugsGleyn LusayaNo ratings yet
- Teacher As A Person in A SocietyDocument16 pagesTeacher As A Person in A SocietyAngel AndesNo ratings yet
- NCMB317: Shared Psychotic DisorderDocument21 pagesNCMB317: Shared Psychotic DisorderArmand Bong Santiago100% (1)
- Nursing Health History: Demographic ProfileDocument19 pagesNursing Health History: Demographic ProfileRoyce Vincent TizonNo ratings yet
- Case StudyDocument16 pagesCase StudyArmand Bong Santiago100% (1)
- Voluntariness of Human Act NotesDocument2 pagesVoluntariness of Human Act NotesKurt MacaslingNo ratings yet
- 30 Different Types of Doctors and What They DoDocument4 pages30 Different Types of Doctors and What They DoGemma C AlejagaNo ratings yet
- Johari WindowDocument11 pagesJohari WindowRevathiSaiReddyNo ratings yet
- A Survey On SmokingDocument40 pagesA Survey On SmokingBenz Atnapas100% (1)
- Revised Module in EthicsDocument135 pagesRevised Module in EthicsHazel Mae BeldaNo ratings yet
- Veritas Listening QuizDocument1 pageVeritas Listening QuizMushy_ayaNo ratings yet
- New CurriculumDocument14 pagesNew CurriculumROMER LOZADANo ratings yet
- NCM 107 RLE 1F - Labor and DeliveryDocument68 pagesNCM 107 RLE 1F - Labor and DeliveryNotur BarbielatNo ratings yet
- NCM 112 - HepatitisDocument8 pagesNCM 112 - HepatitisMara Jon Ocden CasibenNo ratings yet
- Consent 1Document4 pagesConsent 1Pau-pau BasiNo ratings yet
- Research 2Document17 pagesResearch 2Glenn OthersNo ratings yet
- Home For The AgedDocument6 pagesHome For The AgedSSA CommissionNo ratings yet
- Final Thesis Copy - Gonzales, ADocument114 pagesFinal Thesis Copy - Gonzales, ADONNABELLE ALIWALAS100% (1)
- The Assessment and Management of Acute Pain in ChildrenDocument7 pagesThe Assessment and Management of Acute Pain in ChildrenMadyline VictoryaNo ratings yet
- Research ConceptualizationDocument54 pagesResearch ConceptualizationKaren MaturanNo ratings yet
- "A Leader Is One Others Follow Willingly and Voluntarily": Passive Aggressive AssertiveDocument4 pages"A Leader Is One Others Follow Willingly and Voluntarily": Passive Aggressive AssertiveYucef Bahian-AbangNo ratings yet
- Research PaperDocument16 pagesResearch Paperapi-547048713No ratings yet
- Frustration in Human BehaviorDocument36 pagesFrustration in Human BehaviorhahahahahaNo ratings yet
- CHN 2 Lec Week 11 Community Organizing Participatory Action ResearchDocument60 pagesCHN 2 Lec Week 11 Community Organizing Participatory Action Researchyuuki konnoNo ratings yet
- UntitledDocument6 pagesUntitledDada Tin GoTanNo ratings yet
- Let Review On Principles and Theories of Learning in MotivationDocument135 pagesLet Review On Principles and Theories of Learning in MotivationEra Mae BarriosNo ratings yet
- UTS MidtermDocument8 pagesUTS MidtermMiko QuisayNo ratings yet
- Nutrition Anthropology KMTC Liz 1Document44 pagesNutrition Anthropology KMTC Liz 1Sharfa WamboiNo ratings yet
- Who Leprosy Control BurdenDocument44 pagesWho Leprosy Control BurdenClaire SoletaNo ratings yet
- WHO 2019 NCoV Contact Tracing 2021.1 EngDocument11 pagesWHO 2019 NCoV Contact Tracing 2021.1 EngNyaboke OlyviahNo ratings yet
- BIOETHICS ABCDE Compilation WK 2 6Document268 pagesBIOETHICS ABCDE Compilation WK 2 6Sexbomb Adela KirstenNo ratings yet
- Module 3 NSTPDocument80 pagesModule 3 NSTPJamie Federizo100% (1)
- Chapter 1 To 6Document73 pagesChapter 1 To 6Geraldine RamosNo ratings yet
- The Maslow ReportDocument31 pagesThe Maslow ReportRoberto Martin SingNo ratings yet
- RESEARCHDocument24 pagesRESEARCHJim Lloyd SalvadorNo ratings yet
- The Psychological and Emotional Effects of The Limited Societal Roles of Persons With Disabilities in Molino, Bacoor City, Cavite (2018) PDFDocument69 pagesThe Psychological and Emotional Effects of The Limited Societal Roles of Persons With Disabilities in Molino, Bacoor City, Cavite (2018) PDFJericho Daniel IgdanesNo ratings yet
- Eden Iquin Serrano: The NursepreneurDocument8 pagesEden Iquin Serrano: The NursepreneurHanah Angelica GalupoNo ratings yet
- Finals Reviewer and Activities NCM 116 LecDocument24 pagesFinals Reviewer and Activities NCM 116 LecMary CruzNo ratings yet
- Martha Rogers, Dorothea Orem, Imogene KingDocument9 pagesMartha Rogers, Dorothea Orem, Imogene KingCASTRO, ANDREI KARL Z.No ratings yet
- NCMB 418 Midterm ReviewerDocument13 pagesNCMB 418 Midterm ReviewerMARIA KYLA PAMANo ratings yet
- The Level of Mental Health Literacy of Filipino Adults in Metro Manila at The Time of COVID-19 PandemicDocument18 pagesThe Level of Mental Health Literacy of Filipino Adults in Metro Manila at The Time of COVID-19 PandemicPsychology and Education: A Multidisciplinary Journal100% (1)
- Mental HealthDocument18 pagesMental HealthHpg HsuNo ratings yet
- Jose C. Feliciano College FoundationDocument12 pagesJose C. Feliciano College FoundationJake Aaron CatanghalNo ratings yet
- Post Test and CfuDocument10 pagesPost Test and CfuMarie Fatima Quidet UdalbeNo ratings yet
- NCM 114 ReviewerDocument12 pagesNCM 114 ReviewerEmmanuelNo ratings yet
- The Quarter-Life PeriodDocument21 pagesThe Quarter-Life Periodkevin bayuNo ratings yet
- Eco MapDocument2 pagesEco MapBeyLha Ituwh AquhNo ratings yet
- 6.3 7Document26 pages6.3 7Revy CumahigNo ratings yet
- BIOETHICSDocument11 pagesBIOETHICSMaderazo, Rowan XinNo ratings yet
- Neurodevelopmental Disorders ADHDDocument40 pagesNeurodevelopmental Disorders ADHDTrisha Mae MarquezNo ratings yet
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
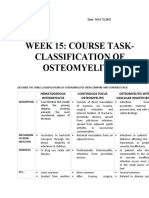
- OSTEOMYELITISDocument2 pagesOSTEOMYELITISArmand Bong Santiago100% (1)
- Week 1 Critical Care Nursing. SlideDocument80 pagesWeek 1 Critical Care Nursing. SlideArmand Bong SantiagoNo ratings yet
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
- NCBM317: Week 15Document2 pagesNCBM317: Week 15Armand Bong Santiago100% (2)
- NCMB317: Week 2 RLE Theories in The Care Patients With Maladaptive BehaviorDocument5 pagesNCMB317: Week 2 RLE Theories in The Care Patients With Maladaptive BehaviorArmand Bong Santiago100% (1)
- NCMB317: Shared Psychotic DisorderDocument21 pagesNCMB317: Shared Psychotic DisorderArmand Bong Santiago100% (1)
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- NCMB 317: Mental Health and IllnessDocument52 pagesNCMB 317: Mental Health and IllnessArmand Bong SantiagoNo ratings yet
- NCMB317: RupturedDocument12 pagesNCMB317: RupturedArmand Bong Santiago100% (1)
- NCMB317 LECTURE Cu 3 Week 3 Lec SchizophreniaDocument3 pagesNCMB317 LECTURE Cu 3 Week 3 Lec SchizophreniaArmand Bong Santiago100% (1)
- Case StudyDocument16 pagesCase StudyArmand Bong Santiago100% (1)
- NCMB317 AutismDocument1 pageNCMB317 AutismArmand Bong Santiago100% (1)
- NCMB316: Compilation Finals in NCMB316Document23 pagesNCMB316: Compilation Finals in NCMB316Armand Bong Santiago100% (1)
- NCMB316 Week 7 InfographicsDocument2 pagesNCMB316 Week 7 InfographicsArmand Bong Santiago100% (1)
- NCMB316 Week 7: Course Unit 6Document5 pagesNCMB316 Week 7: Course Unit 6Armand Bong SantiagoNo ratings yet
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- NCMB316 Cu1 DiscussionDocument1 pageNCMB316 Cu1 DiscussionArmand Bong Santiago100% (1)
- NCMB 316 (Case Study Cholecystitis Cholelithiasis Disease)Document27 pagesNCMB 316 (Case Study Cholecystitis Cholelithiasis Disease)Armand Bong Santiago100% (2)
- Review of The Korean Medicine Studies For Attention Deficit Hyperactivity Disorder (ADHD) in ChildrenDocument13 pagesReview of The Korean Medicine Studies For Attention Deficit Hyperactivity Disorder (ADHD) in Childrenchaitanya gNo ratings yet
- ABCs of Psychiatric MedicinesDocument41 pagesABCs of Psychiatric Medicines아이닠텓No ratings yet
- DB01 Drug ClassificationDocument20 pagesDB01 Drug ClassificationMayank TewatiaNo ratings yet
- ADHD Research PaperDocument38 pagesADHD Research PaperCastillo AdrianNo ratings yet
- 3rd International CongressDocument158 pages3rd International CongressPaladiciuc DanielNo ratings yet
- 17Document35 pages17Gwen PhamNo ratings yet
- Drug StudyDocument1 pageDrug StudyZia CaldozaNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Psychotropic MedicationsDocument17 pagesPsychotropic MedicationsMJ Torralba100% (1)
- Kihlstrom GeneralPsych Sum12 SyllabusDocument12 pagesKihlstrom GeneralPsych Sum12 SyllabusM. David yosoofNo ratings yet
- Chapter 20 - Child and Adolescent DisordersDocument4 pagesChapter 20 - Child and Adolescent Disordersdensu4uNo ratings yet
- Case Study PP - AdhdDocument21 pagesCase Study PP - Adhdapi-482726932100% (1)
- Alternative DietDocument31 pagesAlternative Dietiri_balNo ratings yet
- CNS Drugs TextDocument27 pagesCNS Drugs TextTina TalmadgeNo ratings yet
- Psychiatric Disorders of Childhood PDFDocument55 pagesPsychiatric Disorders of Childhood PDFJenny Wong100% (1)
- The Terror of Pediatric Medicine DR SircusDocument338 pagesThe Terror of Pediatric Medicine DR SircusJustiniano Delfin100% (2)
- Dopamine Serotonin Interactions in Attention Deficit Hyperactivity Disorder ADHDDocument30 pagesDopamine Serotonin Interactions in Attention Deficit Hyperactivity Disorder ADHDpcfernandezdiazNo ratings yet
- Drug Fact Sheet: Amphetamines AmphetaminesDocument1 pageDrug Fact Sheet: Amphetamines AmphetaminesEvandro Ricardo GomesNo ratings yet
- DexmethylphenidateDocument2 pagesDexmethylphenidateaparna_losariNo ratings yet
- Package Leaflet: Information For The User: Important Things You Need To Know About Your MedicineDocument11 pagesPackage Leaflet: Information For The User: Important Things You Need To Know About Your MedicineMaría Virginia Armas RodríguezNo ratings yet
- ADHD and More - Olympic Gold Medalist Michael Phelps and ADHDDocument6 pagesADHD and More - Olympic Gold Medalist Michael Phelps and ADHDsamir249No ratings yet
- MethylphenidateDocument9 pagesMethylphenidateSiegfried CristoforNo ratings yet
- Psychiatric Medication BasicsDocument16 pagesPsychiatric Medication BasicsCarmen HollidayNo ratings yet
- Nursing Exam Cram Sheet For The NCLEX-RN: 1. Test Information 5. ABG ValuesDocument9 pagesNursing Exam Cram Sheet For The NCLEX-RN: 1. Test Information 5. ABG ValuesGee Angela ZozobradoNo ratings yet
- Ritalin and Other Methylphenidate Containing Drugs Drugs The Straight FactsDocument107 pagesRitalin and Other Methylphenidate Containing Drugs Drugs The Straight Factsppappi12100% (5)
- JBC-Article-Vol-14-Issue-2 5-What You Should Know About Attention Deficit Disorder-WelchDocument6 pagesJBC-Article-Vol-14-Issue-2 5-What You Should Know About Attention Deficit Disorder-WelchtghsilvaNo ratings yet
- Central Nervous System StimulantsDocument33 pagesCentral Nervous System StimulantsShweta KateNo ratings yet
- LC-MS/MS Assay of Methylphenidate: Stability and Pharmacokinetics in HumanDocument6 pagesLC-MS/MS Assay of Methylphenidate: Stability and Pharmacokinetics in HumanasdgasdfasdfassdfasdfNo ratings yet
- The Scutellaria Flavone, Oroxylin A, Improves Attention-DeficitDocument8 pagesThe Scutellaria Flavone, Oroxylin A, Improves Attention-DeficitGregory AssonitisNo ratings yet
- Methylphenidate For ADHD: Information For Parents and CarersDocument2 pagesMethylphenidate For ADHD: Information For Parents and CarersMaría Virginia Armas RodríguezNo ratings yet