You might also like
- NCMB 316: Week 1 Course Unit 1Document3 pagesNCMB 316: Week 1 Course Unit 1Armand Bong Santiago100% (1)
- Diagnostic Imaging ProceduresDocument6 pagesDiagnostic Imaging ProceduresMichaela JapsayNo ratings yet
- De Sagun, Leila Camille, A. NCMB312-RLE BSN3Y1-1B Course Task #1Document1 pageDe Sagun, Leila Camille, A. NCMB312-RLE BSN3Y1-1B Course Task #1Carl SantosNo ratings yet
- QuestionDocument6 pagesQuestiontravelbeeNo ratings yet
- CHN - NCPDocument2 pagesCHN - NCPfhengNo ratings yet
- Week 9: Course Task-Case Analysis Renal DisordersDocument4 pagesWeek 9: Course Task-Case Analysis Renal DisordersBELTRAN, JEANNE MAURICENo ratings yet
- Philippine Health Agenda 2016-2022 GoalsDocument32 pagesPhilippine Health Agenda 2016-2022 GoalsCaren Gelarzo50% (2)
- HIV Case Study: Priority Nursing Diagnoses and CareDocument3 pagesHIV Case Study: Priority Nursing Diagnoses and CarechoobiNo ratings yet
- Professional AdjustmentDocument22 pagesProfessional AdjustmentArgee Alonsabe100% (1)
- Nursing Care PlanDocument10 pagesNursing Care PlanmariasomorayNo ratings yet
- Yanga - NCP, Drug Study, FdarDocument7 pagesYanga - NCP, Drug Study, Fdar3amabelle arevaloNo ratings yet
- Assessing and reassuring an elderly postoperative patientDocument1 pageAssessing and reassuring an elderly postoperative patientNestor CabacunganNo ratings yet
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- Nursing Information SystemDocument2 pagesNursing Information SystemkcarpioNo ratings yet
- 51 100Document18 pages51 100Jaessa Feliciano100% (1)
- Kabiven: (Amino Acids, Electrolytes, Dextrose and Lipid Injectable Emulsion), For Intravenous UseDocument24 pagesKabiven: (Amino Acids, Electrolytes, Dextrose and Lipid Injectable Emulsion), For Intravenous UseDivine Mercy De JulianNo ratings yet
- Don Mariano Marcos Memorial State University Nursing CaseDocument9 pagesDon Mariano Marcos Memorial State University Nursing CaseJoselyn M. LachicaNo ratings yet
- Unang Yakap: Why Moms Should Include It in Their Birth PlansDocument3 pagesUnang Yakap: Why Moms Should Include It in Their Birth PlansTyron ChuaNo ratings yet
- Ra 10344Document6 pagesRa 10344Lrac KangNo ratings yet
- LG Case StudyDocument5 pagesLG Case StudyKevzNo ratings yet
- Quiz LeukemiaDocument4 pagesQuiz LeukemiaHanna La MadridNo ratings yet
- Managing Hypertension to Prevent ComplicationsDocument10 pagesManaging Hypertension to Prevent ComplicationsArabylle Maranca AbuelNo ratings yet
- HemodialysisDocument2 pagesHemodialysisjustin_saneNo ratings yet
- SAS #14 - Decent Work Employment - Transcultural NursingDocument9 pagesSAS #14 - Decent Work Employment - Transcultural NursingBless O DumagoNo ratings yet
- Week 1 - Ms1 Course Task Cu1Document1 pageWeek 1 - Ms1 Course Task Cu1jaira magbanuaNo ratings yet
- CetirizineDocument2 pagesCetirizinelintangNo ratings yet
- Course Task Week 7 314 RleDocument1 pageCourse Task Week 7 314 RleAngie BaylonNo ratings yet
- Nausea and Vomiting Nausea and VomitingDocument6 pagesNausea and Vomiting Nausea and VomitingTHERESA CLAIRE ENCINARESNo ratings yet
- Evaluating Family Health ProgramsDocument4 pagesEvaluating Family Health ProgramsDummy AccountNo ratings yet
- Nebulization Nursing Procedure at Ateneo de Zamboanga UniversityDocument9 pagesNebulization Nursing Procedure at Ateneo de Zamboanga UniversityMitzi BelamideNo ratings yet
- PointersDocument49 pagesPointersStephanie Villanueva AdvinculaNo ratings yet
- Physiobiologic Bases and Behavior Neuroscience: Biology and BehaviorDocument25 pagesPhysiobiologic Bases and Behavior Neuroscience: Biology and BehaviorKeith AquinoNo ratings yet
- Psychopathology of DepressionDocument3 pagesPsychopathology of DepressionAnanyaNo ratings yet
- Republic ActDocument36 pagesRepublic ActjanNo ratings yet
- Phases of The COPAR ProcessDocument8 pagesPhases of The COPAR ProcessmerlNo ratings yet
- Patient's ProfileDocument4 pagesPatient's ProfileSnowhite NeymarNo ratings yet
- History and Assessment & Anatomy and Physiology of BurnsDocument10 pagesHistory and Assessment & Anatomy and Physiology of BurnsRina MaeNo ratings yet
- Types of ShocksDocument33 pagesTypes of Shocksmark OrpillaNo ratings yet
- Pharmaco TherapeuticsDocument19 pagesPharmaco TherapeuticsJareena BegumNo ratings yet
- Involving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialDocument10 pagesInvolving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialAngel MayNo ratings yet
- ActemraDocument7 pagesActemraLinda KvastadNo ratings yet
- Chest Pain Care PlanDocument2 pagesChest Pain Care Planapi-545292605No ratings yet
- Myocardial Infarction (Diseases For Oral Revalida)Document12 pagesMyocardial Infarction (Diseases For Oral Revalida)Suzette PipoNo ratings yet
- Telemedicine framework for COVIDDocument3 pagesTelemedicine framework for COVIDAngela NeriNo ratings yet
- Nursing Diagnosis - Saliva Test For HIVDocument3 pagesNursing Diagnosis - Saliva Test For HIVMarsha AngelieNo ratings yet
- SucralfateDocument3 pagesSucralfateViziteu AlexandraNo ratings yet
- Acute Head InjuryDocument5 pagesAcute Head InjuryRitesh KumarNo ratings yet
- Pharmacological Sheet for SupermanDocument17 pagesPharmacological Sheet for SupermanIngrid NicolasNo ratings yet
- NCPDocument10 pagesNCPbabycheska08No ratings yet
- Stages of Labor ADocument14 pagesStages of Labor AMaria Angela Viray100% (1)
- ValvularDocument2 pagesValvularJulia Rae Delos SantosNo ratings yet
- NCPDocument9 pagesNCPLeolene Grace BautistaNo ratings yet
- Hirschprungs DiseaseDocument26 pagesHirschprungs DiseaseAndrian PramanaNo ratings yet
- DRUG StudyDocument4 pagesDRUG StudyMaica LectanaNo ratings yet
- Nursing ExamDocument11 pagesNursing ExamGunan DwynethNo ratings yet
- Anti Tetanus Serum IDocument2 pagesAnti Tetanus Serum IRobby EffendyNo ratings yet
- Scribd 020922 Case Study-Oncology A&kDocument2 pagesScribd 020922 Case Study-Oncology A&kKellie DNo ratings yet
- 2 AppendicitisDocument9 pages2 AppendicitisPavi MuruganathanNo ratings yet
- Clinical Replacement Student Packet-2Document12 pagesClinical Replacement Student Packet-2ida50% (2)
- ERCP Procedure Guide SummaryDocument7 pagesERCP Procedure Guide SummaryFachrur RodjiNo ratings yet
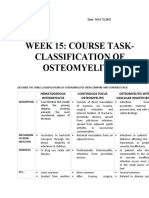
- OSTEOMYELITISDocument2 pagesOSTEOMYELITISArmand Bong Santiago100% (1)
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
- Week 1 Critical Care Nursing. SlideDocument80 pagesWeek 1 Critical Care Nursing. SlideArmand Bong SantiagoNo ratings yet
- NCMB317: Week 2 RLE Theories in The Care Patients With Maladaptive BehaviorDocument5 pagesNCMB317: Week 2 RLE Theories in The Care Patients With Maladaptive BehaviorArmand Bong Santiago100% (1)
- NCBM317: Week 15Document2 pagesNCBM317: Week 15Armand Bong Santiago100% (2)
- NCMB317 LECTURE Cu 3 Week 3 Lec SchizophreniaDocument3 pagesNCMB317 LECTURE Cu 3 Week 3 Lec SchizophreniaArmand Bong Santiago100% (1)
- NCMB317: RupturedDocument12 pagesNCMB317: RupturedArmand Bong Santiago100% (1)
- NCMB317: Shared Psychotic DisorderDocument21 pagesNCMB317: Shared Psychotic DisorderArmand Bong Santiago100% (1)
- NCMB 317: Mental Health and IllnessDocument52 pagesNCMB 317: Mental Health and IllnessArmand Bong SantiagoNo ratings yet
- NCMB 317 AdhdDocument14 pagesNCMB 317 AdhdArmand Bong Santiago100% (1)
- NCMB317 AutismDocument1 pageNCMB317 AutismArmand Bong Santiago100% (1)
- Case StudyDocument16 pagesCase StudyArmand Bong Santiago100% (1)
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- NCMB316 Week 7 InfographicsDocument2 pagesNCMB316 Week 7 InfographicsArmand Bong Santiago100% (1)
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- NCMB 316 (Case Study Cholecystitis Cholelithiasis Disease)Document27 pagesNCMB 316 (Case Study Cholecystitis Cholelithiasis Disease)Armand Bong Santiago100% (2)
- NCMB316 Cu1 DiscussionDocument1 pageNCMB316 Cu1 DiscussionArmand Bong Santiago100% (1)
- NCMB316 Week 7: Course Unit 6Document5 pagesNCMB316 Week 7: Course Unit 6Armand Bong SantiagoNo ratings yet
- 1 EcotourismDocument83 pages1 EcotourismAkshay JainNo ratings yet
- My Favourite Teacher Essay Below AverageDocument1 pageMy Favourite Teacher Essay Below AverageRajaboy Raja100% (1)
- ALS Metallurgy - Gold Extraction ProcessDocument8 pagesALS Metallurgy - Gold Extraction ProcessalxmalagaNo ratings yet
- Magnetic Effects of Current PDFDocument32 pagesMagnetic Effects of Current PDFAdarshNo ratings yet
- Acc702 - Cost and Management Accounting 1. Assignment 1 - QuestionairesDocument4 pagesAcc702 - Cost and Management Accounting 1. Assignment 1 - QuestionairesLyle BulletzNo ratings yet
- 100 Allowed FoodDocument2 pages100 Allowed Foodv_sharonNo ratings yet
- Project Management Using Critical Path Method (CPM) - Apragmatic StudyDocument11 pagesProject Management Using Critical Path Method (CPM) - Apragmatic StudyNizam HasniNo ratings yet
- Reaction to Bonifacio: Ang Unang Pangulo (2014) filmDocument2 pagesReaction to Bonifacio: Ang Unang Pangulo (2014) filmJose Mari King0% (1)
- Opm MashupDocument1 pageOpm MashupABELLA, HAROLD A.No ratings yet
- Injera Production and Export Business PlanDocument50 pagesInjera Production and Export Business PlanTumim84% (44)
- The Innovator's Secret WeaponDocument9 pagesThe Innovator's Secret WeaponNaval VaswaniNo ratings yet
- Importance of Value Education in Life and SchoolsDocument2 pagesImportance of Value Education in Life and SchoolsRomel Jordias BregiraNo ratings yet
- Finale 2005b - (Holly Mass of ST Peter DamianDocument6 pagesFinale 2005b - (Holly Mass of ST Peter DamianArmelNo ratings yet
- Liquidity and Profitability AnalysisDocument100 pagesLiquidity and Profitability Analysisjoel john100% (1)
- Conditions of Contract For: ConstructionDocument30 pagesConditions of Contract For: Constructionvladimir100% (2)
- Problems of Education in The 21st Century, Vol. 76, No. 3, 2018Document137 pagesProblems of Education in The 21st Century, Vol. 76, No. 3, 2018Scientia Socialis, Ltd.No ratings yet
- Handbook Qeeg Chapter 10Document27 pagesHandbook Qeeg Chapter 10Tergantung WaktuNo ratings yet
- Dawn Ullmann - ReferenceDocument1 pageDawn Ullmann - Referenceapi-418750957No ratings yet
- High risk patient dental questionsDocument3 pagesHigh risk patient dental questionsFoysal SirazeeNo ratings yet
- Acefyl SPP - 03 Dec 2010Document54 pagesAcefyl SPP - 03 Dec 2010maliakbar111No ratings yet
- Case Study EntDocument22 pagesCase Study Entnurul syafiqah yahyaNo ratings yet
- Louvre Plan Information EnglishDocument2 pagesLouvre Plan Information EnglishMehak GoyalNo ratings yet
- Leontine O'Gorman, RSCJDocument4 pagesLeontine O'Gorman, RSCJuptickdarter0rNo ratings yet
- Karmila Kristina Paladang, Siane Indriani, Kurnia P. S DirgantoroDocument11 pagesKarmila Kristina Paladang, Siane Indriani, Kurnia P. S DirgantoroDaniel DikmanNo ratings yet
- Classwork Natural Selection WorksheetDocument2 pagesClasswork Natural Selection WorksheetGarnetNo ratings yet
- In Partial Fulfilment of The Requirements in Research Methods ClassDocument10 pagesIn Partial Fulfilment of The Requirements in Research Methods ClasstaniatotsNo ratings yet
- Managing Cervical Spondylosis With Homeopathy TreatmentDocument2 pagesManaging Cervical Spondylosis With Homeopathy TreatmentDocco360No ratings yet
- Gang Rape Jokes by ViceralDocument1 pageGang Rape Jokes by ViceralimmissgeniusNo ratings yet
- Study Plan - PharmD Curriculum ReformDocument23 pagesStudy Plan - PharmD Curriculum ReformRayonesh RayanaNo ratings yet
- Macro PerspectiveDocument3 pagesMacro PerspectiveMARITONI MEDALLANo ratings yet