You might also like
- Common Disorde Rs in ChildrenDocument172 pagesCommon Disorde Rs in Childrenblacklilha100% (1)
- Communicable DiseasesDocument101 pagesCommunicable DiseasesKira100% (4)
- Lesson 13 - Diabetes, Cancer and Heart DiseaseDocument28 pagesLesson 13 - Diabetes, Cancer and Heart DiseaseAlejandro GuerreroNo ratings yet
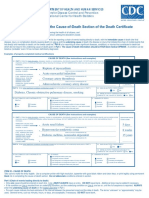
- Instructions For Completing The Cause of Death Section On Death Certificate PDFDocument2 pagesInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoNo ratings yet
- Bronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)Document29 pagesBronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)HimanshiNo ratings yet
- A. WOC Acute Lungs Oedem.: Gangguan Perfusi JaringanDocument1 pageA. WOC Acute Lungs Oedem.: Gangguan Perfusi Jaringanrizki vitaNo ratings yet
- Swollen Lymph Nodes (Glands) : What Are Lymph Nodes? What Do They Do?Document8 pagesSwollen Lymph Nodes (Glands) : What Are Lymph Nodes? What Do They Do?AisyahNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Biostat ManualDocument97 pagesBiostat ManualTwaha R. Kabandika100% (1)
- Acute EpiglottisDocument20 pagesAcute EpiglottissuciNo ratings yet
- Croup: Dr. Shveta Sethi Narula A.P. MicrobiologyDocument14 pagesCroup: Dr. Shveta Sethi Narula A.P. Microbiology12. Akshit AtwalNo ratings yet
- CD Integu 1Document5 pagesCD Integu 1gwen manalonNo ratings yet
- Munity Acquired PneumoniaDocument4 pagesMunity Acquired PneumoniaDIVEN SolvonNo ratings yet
- Pulmonary Tuberculosis: Survive Inside The MacrophagesDocument6 pagesPulmonary Tuberculosis: Survive Inside The MacrophagesDIVEN SolvonNo ratings yet
- Typhoid and Dengue PPT by Shefali RanaDocument47 pagesTyphoid and Dengue PPT by Shefali RanariyaNo ratings yet
- File 18586Document6 pagesFile 18586Mohammed MuthanaNo ratings yet
- Typhidot Is A: Medical Test Elisa Igm Igg Antibodies Outer Membrane Protein Salmonella TyphiDocument5 pagesTyphidot Is A: Medical Test Elisa Igm Igg Antibodies Outer Membrane Protein Salmonella TyphiDecember TwoNo ratings yet
- Referat Demam TifoidDocument30 pagesReferat Demam TifoidBening IrhamnaNo ratings yet
- Stridor: Anas ObeidDocument43 pagesStridor: Anas ObeidAnas ObiedNo ratings yet
- 02 Respi EmergenciesDocument133 pages02 Respi EmergenciesLizeil VelardeNo ratings yet
- Croup, Bronchiolitis and Pneumonia Diagnosis and ManagementDocument43 pagesCroup, Bronchiolitis and Pneumonia Diagnosis and ManagementHaider Nadhem AL-rubaiNo ratings yet
- CcroupDocument53 pagesCcroupOlivia BernadiNo ratings yet
- Education and Practice: Approach To A Child With Recurrent PneumoniaDocument7 pagesEducation and Practice: Approach To A Child With Recurrent PneumoniaGd SuarantaNo ratings yet
- Food IntoxicationDocument34 pagesFood IntoxicationMuqtadir “The Ruler” KuchikiNo ratings yet
- Acute Air Way Emergencies: Adisu B, MDDocument45 pagesAcute Air Way Emergencies: Adisu B, MDMelkamu TulbakeNo ratings yet
- Pneumonia PPT NewDocument22 pagesPneumonia PPT NewOsuri MapitigamaNo ratings yet
- Pneumonia BedsideDocument4 pagesPneumonia BedsideMAJ BEAU S PICCIO MCNo ratings yet
- A. Infectious ProcessDocument22 pagesA. Infectious ProcessKyla Malapit GarvidaNo ratings yet
- Communicable Disease Lectures 2Document2 pagesCommunicable Disease Lectures 2Sheana TmplNo ratings yet
- BronchopneumoniDocument23 pagesBronchopneumonisyarifah naziraNo ratings yet
- 02 Acute Airway ObstructionDocument3 pages02 Acute Airway Obstructioncharmainemargaret.parreno.medNo ratings yet
- Clinical Case 7Document7 pagesClinical Case 7Beni KelnerNo ratings yet
- Document (3)Document7 pagesDocument (3)p4b5No ratings yet
- Name: Carlo M. Yao Bachelor of Science in NursingDocument33 pagesName: Carlo M. Yao Bachelor of Science in Nursingcarlo24_briggsNo ratings yet
- Chapter 27 - Lower Respiratory ProblemsDocument10 pagesChapter 27 - Lower Respiratory Problemsjosie teehNo ratings yet
- DENGUE CONTROL PROGRAM: Prevention, Symptoms, TreatmentDocument23 pagesDENGUE CONTROL PROGRAM: Prevention, Symptoms, TreatmentERMIAS, ZENDY I.No ratings yet
- Meningococalmeningitis: Presented by Class 6 B Community Medicine DepartmentDocument41 pagesMeningococalmeningitis: Presented by Class 6 B Community Medicine DepartmentMohamed AhmedNo ratings yet
- MK BronchiolitisDocument6 pagesMK BronchiolitisMoses Jr Kazevu100% (1)
- Git T13 2024Document17 pagesGit T13 2024myarjddbzNo ratings yet
- TB SYMPTOMS CAUSES TREATMENTDocument19 pagesTB SYMPTOMS CAUSES TREATMENTLhealene MacanasNo ratings yet
- Laryngitis by DR - Ahmed.a.al-Zubiadi F.I.C.M.SDocument17 pagesLaryngitis by DR - Ahmed.a.al-Zubiadi F.I.C.M.SRini A. PujaDaraNo ratings yet
- DengueDocument4 pagesDengueAdrian Jake LiuNo ratings yet
- MeaslesDocument2 pagesMeasleskyeriaNo ratings yet
- Whooping CoughDocument25 pagesWhooping CoughchkiershadiNo ratings yet
- Croup (Laryngotracheobronchitis) : EtiologyDocument13 pagesCroup (Laryngotracheobronchitis) : EtiologyOmar mohamedNo ratings yet
- BRONCHOPNEUMONIA: AN OVERVIEWDocument18 pagesBRONCHOPNEUMONIA: AN OVERVIEWMANEESH MANINo ratings yet
- Typhoid Fever: Presented by Abhinay Sharma BhugooDocument44 pagesTyphoid Fever: Presented by Abhinay Sharma Bhugooabhinay_1712No ratings yet
- Pediatric Nursing Review Course: Epiglottitis, Bronchiolitis, PneumoniaDocument2 pagesPediatric Nursing Review Course: Epiglottitis, Bronchiolitis, PneumoniaDoctor In-ProgressNo ratings yet
- Pertussis: Is Highly Contagious Respiratory DiseaseDocument20 pagesPertussis: Is Highly Contagious Respiratory DiseaseCharlz ZipaganNo ratings yet
- ChestDocument46 pagesChestNokatNo ratings yet
- Infections of the Larynx: Causes, Symptoms and TreatmentsDocument57 pagesInfections of the Larynx: Causes, Symptoms and TreatmentsDrravikumar BhandariNo ratings yet
- Felső Légúti FertőzésekDocument20 pagesFelső Légúti FertőzésekKondász Antal Gábor MedNo ratings yet
- Lestospira Interrogans GRP 5 1Document3 pagesLestospira Interrogans GRP 5 1Raiden EiNo ratings yet
- Otitis MediaDocument42 pagesOtitis MediaUchyIntamNo ratings yet
- PedrosDocument24 pagesPedroslorella_abejuelaNo ratings yet
- Group 1Document20 pagesGroup 1Emily BalmesNo ratings yet
- Pneumonia: Episode OverviewDocument9 pagesPneumonia: Episode Overviewsamfarmer333No ratings yet
- Diphtheria HandoutsDocument8 pagesDiphtheria HandoutsRachelle Mae DimayugaNo ratings yet
- Chemotherapy ComplicationDocument21 pagesChemotherapy ComplicationDr ZakaryaNo ratings yet
- Physical Education 12 Pneumonia: To Be Reported By: Alawi, Lhamiah M. Casano, Diana Elizabeth C. Kinoshita, Ryou GDocument21 pagesPhysical Education 12 Pneumonia: To Be Reported By: Alawi, Lhamiah M. Casano, Diana Elizabeth C. Kinoshita, Ryou GRyou KinoshitaNo ratings yet
- Oxygen Saturation (If Available) : IagnosisDocument3 pagesOxygen Saturation (If Available) : Iagnosisrezairfan221No ratings yet
- Indications For BronchosDocument2 pagesIndications For BronchosRanjith KumarNo ratings yet
- Peri TonsilLar AbscessDocument6 pagesPeri TonsilLar Abscessrivan90No ratings yet
- Typhoid Fever: By, Arathy DarvinDocument35 pagesTyphoid Fever: By, Arathy DarvinJaina JoseNo ratings yet
- Peste Des Petits RuminantsDocument6 pagesPeste Des Petits RuminantsKenesaNo ratings yet
- To Improve and Empower Its Work AbilityDocument2 pagesTo Improve and Empower Its Work Abilitygwen manalonNo ratings yet
- SISON - Synchronous Class Lecture 13Document2 pagesSISON - Synchronous Class Lecture 13gwen manalonNo ratings yet
- Act 3 - SSCDocument1 pageAct 3 - SSCgwen manalonNo ratings yet
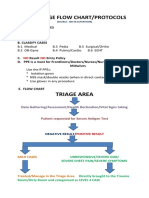
- Idh Triage Flow ChartDocument2 pagesIdh Triage Flow Chartgwen manalonNo ratings yet
- 8 PHYSIOLOGIC CHANGES IN AGING AFFECTING VARIOUS SYSTEMS 2nd PartDocument9 pages8 PHYSIOLOGIC CHANGES IN AGING AFFECTING VARIOUS SYSTEMS 2nd Partgwen manalonNo ratings yet
- Communicable Disease Terminologies and Chain of InfectionDocument8 pagesCommunicable Disease Terminologies and Chain of Infectiongwen manalonNo ratings yet
- 7 Physiologic Changes in Aging Affecting Various SystemsDocument5 pages7 Physiologic Changes in Aging Affecting Various Systemsgwen manalonNo ratings yet
- 8 DotsDocument44 pages8 DotsjyuldipNo ratings yet
- Yl IRIDOCYCLITISDocument14 pagesYl IRIDOCYCLITISNafisa FariddputryNo ratings yet
- Toxoplasmosis Lesson PlanDocument18 pagesToxoplasmosis Lesson PlanDoubt MudendaNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- Report for Vuyyooru Harish Kumar ReddyDocument5 pagesReport for Vuyyooru Harish Kumar ReddyKiran ReddyNo ratings yet
- RETINOPATIDocument31 pagesRETINOPATIAnonymous JWxpPiJfNo ratings yet
- Bell's Palsy - Symptoms and Causes - Mayo ClinicDocument6 pagesBell's Palsy - Symptoms and Causes - Mayo ClinicRoxan PacsayNo ratings yet
- Autoimmune Hemolytic AnemiaDocument4 pagesAutoimmune Hemolytic AnemiaSamuel WibowoNo ratings yet
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Document1 pageDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Janna Mae Canubida Lapitan-MañacapNo ratings yet
- Mental Health Nursing II UNITDocument14 pagesMental Health Nursing II UNITbemina jaNo ratings yet
- Concept Map RSVDocument1 pageConcept Map RSVNoemi GabayNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary Detailsmanoj jainNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: © 2017 John Wiley & Sons LTDDocument6 pagesIntestinal Tuberculosis: A Diagnostic Challenge: © 2017 John Wiley & Sons LTDLily SmithNo ratings yet
- Kochs Postulates Fulfilled For SARS VirusDocument2 pagesKochs Postulates Fulfilled For SARS VirusYoshef Arieka, SKM, MKesNo ratings yet
- Final 2022 Epidemiology Course OutlineDocument13 pagesFinal 2022 Epidemiology Course OutlineGlaneisia Mitchell100% (1)
- Lysosomal Storage DisordersDocument6 pagesLysosomal Storage DisordersRoscelie KhoNo ratings yet
- CertificateDocument1 pageCertificateSOFIKUL HUUSAINNo ratings yet
- Reymark L Bald Pe Interview Narrative ReportDocument3 pagesReymark L Bald Pe Interview Narrative ReportReymark BaldoNo ratings yet
- Diagnosis and Management of Bacterial ConjunctivitisDocument6 pagesDiagnosis and Management of Bacterial ConjunctivitisJonathan JoseNo ratings yet
- Herpes Zoster (Shingles/Acute Posterior Ganglionitis)Document13 pagesHerpes Zoster (Shingles/Acute Posterior Ganglionitis)Shawn Michael SwayzeNo ratings yet
- Heat Stroke: Production Synergy Boosters IncDocument6 pagesHeat Stroke: Production Synergy Boosters IncGilbert A MercadoNo ratings yet
- Personal Hygiene and Life Expectancy Improvements Since 1850 Historic and Epidemiologic Associations PDFDocument4 pagesPersonal Hygiene and Life Expectancy Improvements Since 1850 Historic and Epidemiologic Associations PDFMarko MojsilovićNo ratings yet
- Medical Certificate DetailsDocument3 pagesMedical Certificate DetailsJubel SherifNo ratings yet
- Atypical BacteriaDocument38 pagesAtypical BacteriaKiwanuka KawukiNo ratings yet
- Handwahing DetailsDocument2 pagesHandwahing DetailsLee ShaneNo ratings yet