You might also like
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument13 pagesBest Practice & Research Clinical Obstetrics and Gynaecologymauricio espinelNo ratings yet
- 2018 A Global Overview of Precision Medicine in Type 2 DiabetesDocument12 pages2018 A Global Overview of Precision Medicine in Type 2 Diabetesguanyulin01No ratings yet
- Diabetes y Patologias OralesDocument11 pagesDiabetes y Patologias OralesMedusa GorgonNo ratings yet
- Gene-Diet Interactions in Complex DiseaseDocument9 pagesGene-Diet Interactions in Complex DiseaseJuan RocaNo ratings yet
- Food-Addiction-Symptomology - Impulsivity - Mood - And-Body-Mass-Ind - 2015 - AppetDocument7 pagesFood-Addiction-Symptomology - Impulsivity - Mood - And-Body-Mass-Ind - 2015 - AppetLaura CasadoNo ratings yet
- Effect of Diet On Type 2 Diabetes Mellitus: A ReviewDocument7 pagesEffect of Diet On Type 2 Diabetes Mellitus: A ReviewTowo RottenNo ratings yet
- Prevention of Obesity and Diabetes in Pregnancy: Is It An Impossible Dream?Document9 pagesPrevention of Obesity and Diabetes in Pregnancy: Is It An Impossible Dream?Anonymous P5efHbeNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleSukmaNo ratings yet
- Distress ExperienceDocument9 pagesDistress ExperienceTengku EltrikanawatiNo ratings yet
- Gestational Diabetes Research PaperDocument16 pagesGestational Diabetes Research Paperapi-251486092No ratings yet
- 51 (A Review of Diabetes Mellitus) JMPR-11-188Document3 pages51 (A Review of Diabetes Mellitus) JMPR-11-188M.Akram TatriNo ratings yet
- Mediterranean Diet and Type 2 Diabetes: Katherine Esposito Dario GiuglianoDocument7 pagesMediterranean Diet and Type 2 Diabetes: Katherine Esposito Dario GiuglianoOctavian BabcinschiNo ratings yet
- Jurnal DM GestasionalDocument18 pagesJurnal DM GestasionalEchi DesnawatiNo ratings yet
- Format PengkajianDocument8 pagesFormat PengkajianHandiniNo ratings yet
- New-Guthrie2015Document10 pagesNew-Guthrie2015Ser Eldrin GarciaNo ratings yet
- Type 2 Diabetes Research PaperDocument8 pagesType 2 Diabetes Research Paperkmffzlvkg100% (1)
- Aisyah GDM ArticleDocument18 pagesAisyah GDM ArticleBesari Md DaudNo ratings yet
- Association of Depression With Newly Diagnosed Type 2 Diabetes Among Adults Aged Between 25 To 60 Years in Karachi, PakistanDocument6 pagesAssociation of Depression With Newly Diagnosed Type 2 Diabetes Among Adults Aged Between 25 To 60 Years in Karachi, PakistanLaeeq R MalikNo ratings yet
- Chung2020 Article PrecisionMedicineInDiabetesACoDocument23 pagesChung2020 Article PrecisionMedicineInDiabetesACoFilipa Figueiredo100% (1)
- Meal Timing, Meal Frequency and Metabolic SyndromeDocument10 pagesMeal Timing, Meal Frequency and Metabolic SyndromebryanleonardoripacontrerasNo ratings yet
- Relationship between Diet Compliance and Knowledge, Motivation, Family Support in Diabetes PatientsDocument12 pagesRelationship between Diet Compliance and Knowledge, Motivation, Family Support in Diabetes PatientsdnoksNo ratings yet
- Classification Pathophysiology Diagnosis and ManagDocument10 pagesClassification Pathophysiology Diagnosis and ManagHeru SetiawanNo ratings yet
- Diabetic AdDocument11 pagesDiabetic AdDebela NanessoNo ratings yet
- KAP Towards DMDocument10 pagesKAP Towards DMHabtamu Wondifraw100% (1)
- Life - Course Model NFBCDocument8 pagesLife - Course Model NFBCShayekh M ArifNo ratings yet
- Ozanne Nongenetic Determinants T2DM 2002Document15 pagesOzanne Nongenetic Determinants T2DM 2002syamsulNo ratings yet
- Rising Rates of Diabetes in the US PopulationDocument3 pagesRising Rates of Diabetes in the US PopulationLavenia JulianiNo ratings yet
- Smith 2015 Epigenetic and Developmental Influences On The Risk of Obesity, Diabetes and MsDocument8 pagesSmith 2015 Epigenetic and Developmental Influences On The Risk of Obesity, Diabetes and MsPaul SimononNo ratings yet
- bvac184Document12 pagesbvac184dravlamfNo ratings yet
- Geriatria Articulo EspecialDocument15 pagesGeriatria Articulo EspecialBonchita BellaNo ratings yet
- Prediabetes Progression and TreatmentDocument8 pagesPrediabetes Progression and TreatmentVimal NishadNo ratings yet
- Relationship Between Gut Microbiota, Probiotics, and Type 2 Diabetes MellitusDocument10 pagesRelationship Between Gut Microbiota, Probiotics, and Type 2 Diabetes MellitusPETERNo ratings yet
- Non Adherence and Its Contributing Factors Among Ambulatory Type Two Diabetic Patients in Bishoftu General Hospital, South East, EthiopiaDocument15 pagesNon Adherence and Its Contributing Factors Among Ambulatory Type Two Diabetic Patients in Bishoftu General Hospital, South East, EthiopiaIjupbs IjupbsNo ratings yet
- International Journal of Health Sciences and Research: Stress and Diabetes MellitusDocument8 pagesInternational Journal of Health Sciences and Research: Stress and Diabetes Mellitusamalia dikaNo ratings yet
- International Journal of Health Sciences and Research: Stress and Diabetes MellitusDocument8 pagesInternational Journal of Health Sciences and Research: Stress and Diabetes MellitusmariahelenaneiNo ratings yet
- Nutrients 11 00459Document6 pagesNutrients 11 00459Paskah DianNo ratings yet
- Diabetes AnnotatedDocument5 pagesDiabetes AnnotatedDavon Richard Walter Van-VeenNo ratings yet
- Diabetes - StatPearls - NCBI BookshelfDocument16 pagesDiabetes - StatPearls - NCBI BookshelfWidad SalsabilaNo ratings yet
- Long Term Complications in Youth Onset Type 2 Diabetes: Original ArticleDocument11 pagesLong Term Complications in Youth Onset Type 2 Diabetes: Original ArticleESPINO DE LA TORRE LUZ ELENANo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument11 pagesBest Practice & Research Clinical Endocrinology & MetabolismM Slamet RiyantoNo ratings yet
- Pandey2012 PatentDocument14 pagesPandey2012 Patentiacob ancutaNo ratings yet
- chronic disease and nutritionDocument11 pageschronic disease and nutritionyrmkc9sykzNo ratings yet
- The Prevention of Type II Diabetes MellitusDocument7 pagesThe Prevention of Type II Diabetes Mellitusapi-736636482No ratings yet
- Anti-Obesity Effects of Polyphenol IntakeDocument24 pagesAnti-Obesity Effects of Polyphenol IntakeHuman ResourcesNo ratings yet
- Efektivitas Konseling DM Dalam Meningkatkan Kepatuhan Dan Pengendalian Gula Darah Pada Diabetes Melitus Tipe 2Document12 pagesEfektivitas Konseling DM Dalam Meningkatkan Kepatuhan Dan Pengendalian Gula Darah Pada Diabetes Melitus Tipe 2AmmarForeverAjaNo ratings yet
- By Guest On 26 April 2018Document8 pagesBy Guest On 26 April 2018silvanaNo ratings yet
- Genetics of Type 2 Diabetes Past Present and FuturDocument12 pagesGenetics of Type 2 Diabetes Past Present and FuturChengwustZhangNo ratings yet
- Clinical and Epidemiological Profile of Diabetes Mellitus in Pregnancy, Isle of Youth, 2008Document6 pagesClinical and Epidemiological Profile of Diabetes Mellitus in Pregnancy, Isle of Youth, 2008nunki aprillitaNo ratings yet
- Estrategias Contra A Diabetes (170pag)Document170 pagesEstrategias Contra A Diabetes (170pag)vicenteNo ratings yet
- Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFDocument15 pagesDifferentiation of Diabetes by Pathophysiology, Natural History, and Prognosis PDFHadi PrasetyoNo ratings yet
- Diabetic Prevention ProjectDocument6 pagesDiabetic Prevention ProjectStephen NdireNo ratings yet
- Jurnal DiabetesDocument50 pagesJurnal DiabetesYusmiyati YusmiyatiNo ratings yet
- Deleterious Dozen DMT2Document18 pagesDeleterious Dozen DMT2cecilia zavala100% (1)
- Obesityasadisease: Jagriti Upadhyay,, Olivia Farr,, Nikolaos Perakakis,, Wael Ghaly,, Christos MantzorosDocument21 pagesObesityasadisease: Jagriti Upadhyay,, Olivia Farr,, Nikolaos Perakakis,, Wael Ghaly,, Christos MantzorosAlejandra RamirezNo ratings yet
- Obesity and Type 2 DiabetesDocument18 pagesObesity and Type 2 DiabetespritaultimardianNo ratings yet
- Información DerechoDocument11 pagesInformación Derechoesteban pugaNo ratings yet
- Sarcopenia As A Little-Recognized Comorbidity of Type II Diabetes Mellitus: A Review of The Diagnosis and TreatmentDocument15 pagesSarcopenia As A Little-Recognized Comorbidity of Type II Diabetes Mellitus: A Review of The Diagnosis and TreatmentBernardo Abel Cedeño VelozNo ratings yet
- Paper AnalysisDocument4 pagesPaper AnalysisLayali MassisNo ratings yet
- IDF Prevention Consensus DMDocument13 pagesIDF Prevention Consensus DMDana GrigorescuNo ratings yet
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalFrom EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalNo ratings yet
- 1400 4345 1 PBDocument6 pages1400 4345 1 PBindah puspitaNo ratings yet
- Siegel 2018Document8 pagesSiegel 2018indah puspitaNo ratings yet
- Ray 2016Document5 pagesRay 2016indah puspitaNo ratings yet
- BMJ k2234 FullDocument9 pagesBMJ k2234 Fullindah puspitaNo ratings yet
- Article 4103126131Document6 pagesArticle 4103126131indah puspitaNo ratings yet
- Alamiri 2015Document9 pagesAlamiri 2015indah puspitaNo ratings yet
- School-Based Nutrition Education Improves Knowledge and BehaviorsDocument10 pagesSchool-Based Nutrition Education Improves Knowledge and Behaviorsindah puspitaNo ratings yet
- Efficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsDocument6 pagesEfficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsthiagoNo ratings yet
- (Edited) N31-G6-SOP-and-Conceptual-FrameworkDocument5 pages(Edited) N31-G6-SOP-and-Conceptual-Frameworkst michael machine shopNo ratings yet
- Safety Data Sheet Conbextra Gp2: Revision Date: 01/01/2020 Revision: 0ADocument8 pagesSafety Data Sheet Conbextra Gp2: Revision Date: 01/01/2020 Revision: 0AAnonymous kRIjqBLkNo ratings yet
- Ensuring Optimal Crash Cart FunctionDocument11 pagesEnsuring Optimal Crash Cart FunctionKarren FernandezNo ratings yet
- External Otitis (OE)Document24 pagesExternal Otitis (OE)Hannah BLissNo ratings yet
- Examination Performance Report Spring 2018 Part 1Document3 pagesExamination Performance Report Spring 2018 Part 1Syed Danish AliNo ratings yet
- Health and Skill Related Components of Physical FitnessDocument6 pagesHealth and Skill Related Components of Physical FitnessJovanne CabaluNo ratings yet
- Ibm India Benefits - Covid-19 Help Line & Doctor Tele-ConsultationDocument4 pagesIbm India Benefits - Covid-19 Help Line & Doctor Tele-ConsultationSushovan NandiNo ratings yet
- Q4 Module 4 Answer Health 10Document3 pagesQ4 Module 4 Answer Health 10Brian MirandaNo ratings yet
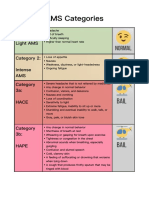
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Assignment On PrincipalDocument10 pagesAssignment On PrincipalmacmohitNo ratings yet
- Causes and Effects of Depression Among StudentsDocument36 pagesCauses and Effects of Depression Among StudentsJustinNo ratings yet
- Prenatal Development and Birth: The Developing Person Through The Life Span Kathleen Stassen Berger - Tenth EditionDocument42 pagesPrenatal Development and Birth: The Developing Person Through The Life Span Kathleen Stassen Berger - Tenth EditionJoel PayneNo ratings yet
- Dien Bali Meeting 11Document5 pagesDien Bali Meeting 11Dien NingsihbaliNo ratings yet
- OHS Management Review Procedure for Pagwin ConstructionDocument4 pagesOHS Management Review Procedure for Pagwin ConstructionDwitikrushna Rout100% (1)
- Tutorial: MODULE: Musculoskeletal System IIDocument3 pagesTutorial: MODULE: Musculoskeletal System IIrishit20% (5)
- Appendix C - Example Subject Areas For DevelopmentDocument4 pagesAppendix C - Example Subject Areas For Developmentpaul machariaNo ratings yet
- World Vision Safe and Prosperous Urban Programming in BasecoDocument14 pagesWorld Vision Safe and Prosperous Urban Programming in BasecoTap TouchNo ratings yet
- PSYCH 7 Course OutlineDocument4 pagesPSYCH 7 Course OutlineJM FranciscoNo ratings yet
- Continuous Insulin InfusionDocument6 pagesContinuous Insulin Infusionbobobo22No ratings yet
- Medical Treatment of Aortic Stenosis: in DepthDocument19 pagesMedical Treatment of Aortic Stenosis: in DepthAlexandra NalgomNo ratings yet
- Reading Unit 3Document2 pagesReading Unit 3estefania aranda jimenezNo ratings yet
- Teks Diskusi PLPGDocument6 pagesTeks Diskusi PLPGKarlonius Bambang PurwantoNo ratings yet
- THE AFFORDABLE ARTHRITIS & OSTEOPOROSIS CUREDocument18 pagesTHE AFFORDABLE ARTHRITIS & OSTEOPOROSIS CURENatalia NeliNo ratings yet
- Medical Certificate for SeafarersDocument1 pageMedical Certificate for SeafarersI Komang Anom Gostap SidhartaNo ratings yet
- My Courses: Home UGRD-PHYED6101-2113T Week 2: Health-Related Fitness Components Prelim Quiz 1Document4 pagesMy Courses: Home UGRD-PHYED6101-2113T Week 2: Health-Related Fitness Components Prelim Quiz 1Miguel Angelo GarciaNo ratings yet
- Theodore Millon On Rosenhan PaperDocument6 pagesTheodore Millon On Rosenhan PaperJuliette WarnesNo ratings yet
- New Harbinger Self-Help Workbook the Mindfulness and Acceptance Workbook for Social Anxiety and Shyness_ Using Acceptance and Commitment Therapy to Free Yourself From Fear and Reclaim Your Life [1st Ed.Document132 pagesNew Harbinger Self-Help Workbook the Mindfulness and Acceptance Workbook for Social Anxiety and Shyness_ Using Acceptance and Commitment Therapy to Free Yourself From Fear and Reclaim Your Life [1st Ed.Wesley Ramalho100% (1)
- Clinical Laboratory Biosafety: Tapeshwar Yadav (Lecturer)Document26 pagesClinical Laboratory Biosafety: Tapeshwar Yadav (Lecturer)Tapeshwar YadavNo ratings yet
- THESIS FinalDocument35 pagesTHESIS FinalAlaine Danica DimaandalNo ratings yet