You might also like
- Rehabilitation interventions may help muscle strength in multi-organ injuryDocument8 pagesRehabilitation interventions may help muscle strength in multi-organ injurysari murnaniNo ratings yet
- ArticleDocument11 pagesArticletgayuNo ratings yet
- Severity Scoring Systems in The Critically IllDocument5 pagesSeverity Scoring Systems in The Critically Illdefitrananda100% (1)
- Trauma Scoring Systems ExplainedDocument12 pagesTrauma Scoring Systems ExplainedputugunaNo ratings yet
- Scoring Systems in The Critically Ill 2010Document9 pagesScoring Systems in The Critically Ill 2010rosalia dahliasariNo ratings yet
- Internation Classification ICSD III BetaDocument8 pagesInternation Classification ICSD III BetaRikizu HobbiesNo ratings yet
- A Systematic Review - 123659Document8 pagesA Systematic Review - 123659S TNo ratings yet
- Journal or Rheumatology 2021 - Effect of Disease Activity On Organ Damage Progression in SLE, University of Toronto Lupus Clinic CohortDocument7 pagesJournal or Rheumatology 2021 - Effect of Disease Activity On Organ Damage Progression in SLE, University of Toronto Lupus Clinic CohortTengku Reza MaulanaNo ratings yet
- Calculated Decisions E1018 SepsisDocument6 pagesCalculated Decisions E1018 SepsisYitzhak AbisayNo ratings yet
- 490-Article Text-1324-1-10-20180508Document9 pages490-Article Text-1324-1-10-20180508FahmiNo ratings yet
- HshsjneDocument5 pagesHshsjneyunia habsariNo ratings yet
- Laboratory Diagnosis of Autoimmune DiseasesDocument6 pagesLaboratory Diagnosis of Autoimmune DiseasesYustina BubnovaNo ratings yet
- Medical Student HandbookDocument36 pagesMedical Student HandbookJulius AdamsNo ratings yet
- Physical Restraint Use in Adult Patients Presenting To A General Emergency DepartmentDocument10 pagesPhysical Restraint Use in Adult Patients Presenting To A General Emergency DepartmentBeatrizNo ratings yet
- Sellitto 2021Document47 pagesSellitto 2021JudybenavidesNo ratings yet
- Use of The SOFA Score To Assess The Incidence of Organ Dysfunction/failure in Intensive Care Units: Results of A Multicenter, Prospective StudyDocument8 pagesUse of The SOFA Score To Assess The Incidence of Organ Dysfunction/failure in Intensive Care Units: Results of A Multicenter, Prospective StudybayuaaNo ratings yet
- Clinical Scale Rates Blepharospasm SeverityDocument6 pagesClinical Scale Rates Blepharospasm SeveritymysticmdNo ratings yet
- Global Assessment Scale For WILSONDocument10 pagesGlobal Assessment Scale For WILSONneha goelNo ratings yet
- Evaluación Back Pain Peter o SullivanDocument11 pagesEvaluación Back Pain Peter o SullivanAntonio tapiaNo ratings yet
- Outcome in Nuerocritical CareDocument7 pagesOutcome in Nuerocritical CareParvathy R NairNo ratings yet
- PRISM ScoreDocument13 pagesPRISM ScoreTammy Utami DewiNo ratings yet
- Evidence-Based Review) : Report of The Quality Standards Subcommittee of The Practice Parameter: Assessing Patients in A Neurology Practice For Risk of Falls (AnDocument9 pagesEvidence-Based Review) : Report of The Quality Standards Subcommittee of The Practice Parameter: Assessing Patients in A Neurology Practice For Risk of Falls (AnSharan SahotaNo ratings yet
- Fried Frailty Pred Surg Outcomes AmCSurg 10Document8 pagesFried Frailty Pred Surg Outcomes AmCSurg 10edos838No ratings yet
- Relation Between BEST Test & Biodex in StrokeDocument7 pagesRelation Between BEST Test & Biodex in StrokeBassam EsmailNo ratings yet
- Principles and ConceptsDocument83 pagesPrinciples and ConceptsAndrea HernandezNo ratings yet
- Somatoform Autonomic DysfunctionDocument36 pagesSomatoform Autonomic DysfunctionSuhana ShresthaNo ratings yet
- Frailty and AnesthesiaDocument33 pagesFrailty and AnesthesiaRadmila KaranNo ratings yet
- Fall Prediction in Neurological Gait Disorders DifDocument15 pagesFall Prediction in Neurological Gait Disorders DifRudolfGerNo ratings yet
- Lupus Concepte Noi, Bertsias, 2016Document5 pagesLupus Concepte Noi, Bertsias, 2016Maria GarabajiuNo ratings yet
- Functional Gait Disorders: A Sign-Based ApproachDocument8 pagesFunctional Gait Disorders: A Sign-Based ApproachFernando Ortiz CorredorNo ratings yet
- Clinical Medicine Ashok ChandraDocument52 pagesClinical Medicine Ashok ChandraVaishnavi Agrawal100% (1)
- CLASI (Penilaian Keparahan Lupus)Document6 pagesCLASI (Penilaian Keparahan Lupus)fiqaalkasieNo ratings yet
- Batt 2013 - ICU-AW - Clinical Phenotypes and Molecular MechanismsDocument9 pagesBatt 2013 - ICU-AW - Clinical Phenotypes and Molecular MechanismsSebastián Caimanque CortésNo ratings yet
- Ev Estado de ConcienciaDocument18 pagesEv Estado de ConcienciaFabiolaNo ratings yet
- Sindrom Multiple Disfungsi OrganDocument8 pagesSindrom Multiple Disfungsi OrganAdi Nugroho MelyanaNo ratings yet
- Epidemiology of MSK Impairment and DisabilityDocument6 pagesEpidemiology of MSK Impairment and DisabilityMd. Ariful IslamNo ratings yet
- American Thoracic Society DocumentsDocument10 pagesAmerican Thoracic Society DocumentsEviNo ratings yet
- Classification of Diagnostic Tests Used With Osteopathic ManipulationDocument5 pagesClassification of Diagnostic Tests Used With Osteopathic ManipulationAntonioNo ratings yet
- A Study of Migraine Characteristics in Joint Hypermobility Syndrome A.K.A. Ehlers-Danlos Syndrome, Hypermobility TypeDocument11 pagesA Study of Migraine Characteristics in Joint Hypermobility Syndrome A.K.A. Ehlers-Danlos Syndrome, Hypermobility TypeAndrea MorenoNo ratings yet
- Salaffietal (2009) - Assessment Instruments For Patients With Fibromyalgia - Properties, Applications and InterpretationDocument14 pagesSalaffietal (2009) - Assessment Instruments For Patients With Fibromyalgia - Properties, Applications and InterpretationLuciana AraújoNo ratings yet
- The Use of The Edmonton Symptom Assessment Scale (ESAS) Within A Palliative Care Unit in The UKDocument10 pagesThe Use of The Edmonton Symptom Assessment Scale (ESAS) Within A Palliative Care Unit in The UKMika AgustianaNo ratings yet
- Delitto 1995Document16 pagesDelitto 1995Raúl BrizuelaNo ratings yet
- The Rheumatological ExaminationDocument5 pagesThe Rheumatological ExaminationRobles Murillo Carlos Eduardo Augusto 1FNo ratings yet
- Development and Preliminary Validation oDocument10 pagesDevelopment and Preliminary Validation osvuttha6No ratings yet
- 1 PBDocument9 pages1 PBKodam SruthilayaNo ratings yet
- Qol in DialysisDocument6 pagesQol in Dialysism29hereNo ratings yet
- A Clinical Rating Scale For Batten DiseaseDocument6 pagesA Clinical Rating Scale For Batten DiseaseMaferNo ratings yet
- Harrison 2018Document12 pagesHarrison 2018JağğuNo ratings yet
- Chap1 MageeDocument83 pagesChap1 MageeSerenela PiazzaNo ratings yet
- TurkJPhysMedRehab 65 132Document7 pagesTurkJPhysMedRehab 65 132Imam IskandarNo ratings yet
- Art 03 OnoseDocument19 pagesArt 03 OnoseBlink TdmNo ratings yet
- Moccia2021 Article AnomalousSelf-experienceBodyImDocument8 pagesMoccia2021 Article AnomalousSelf-experienceBodyImgerard sansNo ratings yet
- 2010 - Rating Scales For Low Back Pain - Longo Et Al PDFDocument64 pages2010 - Rating Scales For Low Back Pain - Longo Et Al PDFA CNo ratings yet
- Neurologic DisordersDocument3 pagesNeurologic Disordersjojimar08No ratings yet
- Sarcopenia ESPEN 2022Document9 pagesSarcopenia ESPEN 2022Tarafainy BasalamahNo ratings yet
- Katzan Et AlDocument9 pagesKatzan Et Alemsutton02No ratings yet
- Combining Orthopedic Special Tests To ImDocument6 pagesCombining Orthopedic Special Tests To ImVladislav KotovNo ratings yet
- 00130478-202105000-00013 Improving "Neuro Checks" in Neonatal ICU and PICU Is A Serial Neurologic Assessment in PediatricsDocument3 pages00130478-202105000-00013 Improving "Neuro Checks" in Neonatal ICU and PICU Is A Serial Neurologic Assessment in PediatricsYo MeNo ratings yet
- Systemic Inflammatory Response SyndromeDocument16 pagesSystemic Inflammatory Response SyndromeRas RosarioNo ratings yet
- RCM - Volume 3 - Issue 2 - Pages 69-72Document4 pagesRCM - Volume 3 - Issue 2 - Pages 69-72valfreNo ratings yet
- 2022 Society of Critical Care Medicine Clinical.15Document37 pages2022 Society of Critical Care Medicine Clinical.15diegorojasNo ratings yet
- IndianJRespirCare7267-7691804 212158Document6 pagesIndianJRespirCare7267-7691804 212158valfreNo ratings yet
- Management of Cardiogenic Shock: Clinical UpdateDocument10 pagesManagement of Cardiogenic Shock: Clinical Updatewelly natanael pNo ratings yet
- Altas Dosis de Vasopresores LeerDocument11 pagesAltas Dosis de Vasopresores LeervalfreNo ratings yet
- Extubacion y RXDocument4 pagesExtubacion y RXvalfreNo ratings yet
- R-07 Behaviour Policy (1536) PDFDocument1 pageR-07 Behaviour Policy (1536) PDFAmerNo ratings yet
- Principles of PharmacologyDocument9 pagesPrinciples of PharmacologybencleeseNo ratings yet
- FCPS 1 Radiology + AnswersDocument25 pagesFCPS 1 Radiology + AnswersZahid Qamar100% (2)
- Drug Presentation On: Aminoven: Submitted To Submitted byDocument6 pagesDrug Presentation On: Aminoven: Submitted To Submitted byShilpi SinghNo ratings yet
- Fungal ClassificationDocument109 pagesFungal ClassificationMirza Shaharyar BaigNo ratings yet
- How to Don and Doff Sterile Gloves SafelyDocument32 pagesHow to Don and Doff Sterile Gloves SafelyCoreen Mangaoang83% (6)
- ABYIP-2023 TemplateDocument3 pagesABYIP-2023 Templatejomar88% (26)
- 849 FullDocument13 pages849 FullAnsuf WicaksonoNo ratings yet
- Social Work ResearchDocument15 pagesSocial Work ResearchSuresh Murugan78% (9)
- NutritionDocument4 pagesNutritionAlisahNo ratings yet
- Dental MaterialDocument2 pagesDental MaterialDela martha0% (1)
- Flow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlDocument4 pagesFlow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlAndreea DiaconuNo ratings yet
- Abnoramal ECGDocument20 pagesAbnoramal ECGImmanuelNo ratings yet
- Case Studies For PharmacyDocument3 pagesCase Studies For PharmacyMahima Sindhi50% (2)
- 서초구 고교기출 4회차Document7 pages서초구 고교기출 4회차ᄋᄋNo ratings yet
- 7 (0) - ICBD 2014-The International Criteria For Behçet's DiseaseDocument10 pages7 (0) - ICBD 2014-The International Criteria For Behçet's Diseasekueiying.suNo ratings yet
- LFD CommunityDocument2 pagesLFD CommunityKryza B. CASTILLONo ratings yet
- PE 10 LAS Quarter 3Document20 pagesPE 10 LAS Quarter 3Dennis100% (1)
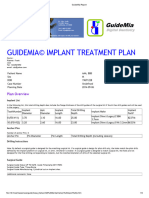
- GuideMia Sample Report - EnglishDocument9 pagesGuideMia Sample Report - Englishzhiao liuNo ratings yet
- Name:Muhammad Mustafa REG NO.12397 Assighment:Behavioural Science Topic:Conflict ManagementDocument15 pagesName:Muhammad Mustafa REG NO.12397 Assighment:Behavioural Science Topic:Conflict Managementmustafa wazirNo ratings yet
- How To Know If U Need Ortho TTDocument3 pagesHow To Know If U Need Ortho TTSubhajit SahaNo ratings yet
- Lyon, G. R., Shaywitz, S. E., & Shaywitz, B. A. (2003) - A Definition of Dyslexia. Annals of Dyslexia, 53 (1), 1-14 PDFDocument14 pagesLyon, G. R., Shaywitz, S. E., & Shaywitz, B. A. (2003) - A Definition of Dyslexia. Annals of Dyslexia, 53 (1), 1-14 PDFCharitini PetridouNo ratings yet
- A Patient 'S Guide To Refractive SurgeryDocument7 pagesA Patient 'S Guide To Refractive SurgeryJon HinesNo ratings yet
- Medication Booklet and TicketDocument3 pagesMedication Booklet and TicketCayanne ChuaNo ratings yet
- 6Document11 pages6UgaugaaNo ratings yet
- The Zone Issue 27Document16 pagesThe Zone Issue 27Jeff Clay GarciaNo ratings yet
- Kauswagan Central Elementary promotes health and wellnessDocument31 pagesKauswagan Central Elementary promotes health and wellnessMayMay SaturNo ratings yet
- Fundamentals of Nursing1Document51 pagesFundamentals of Nursing1Charles Gerard B. BeluanNo ratings yet
- Colonic Irrigation: Holistic Cleansing and DetoxificationDocument5 pagesColonic Irrigation: Holistic Cleansing and DetoxificationVijaya RaniNo ratings yet
- Registrar:: Section 3C: ISO 14001 Audit Criteria (Significant Environmental Aspects)Document1 pageRegistrar:: Section 3C: ISO 14001 Audit Criteria (Significant Environmental Aspects)Tathiana GarcíaNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)