You might also like
- Cerebrovascular Accident or Stroke: By: Thalia Nicole SanchezDocument19 pagesCerebrovascular Accident or Stroke: By: Thalia Nicole SanchezMaesy LorenaNo ratings yet
- Family Medicine EORDocument159 pagesFamily Medicine EORAndrew BowmanNo ratings yet
- Basic Interior Design RulesDocument25 pagesBasic Interior Design RulesMadalina-Irina Tanaselea100% (2)
- Cerebrovascular DiseaseDocument54 pagesCerebrovascular Diseaselisaagustina100% (1)
- Cardiovascular System ExaminationDocument67 pagesCardiovascular System ExaminationJaaydev100% (1)
- Cerebrovascular Accident (Stroke) : - Large Artery Thromboses Are - Small Penetrating EmboliDocument7 pagesCerebrovascular Accident (Stroke) : - Large Artery Thromboses Are - Small Penetrating EmboliKimberly Joy GregorioNo ratings yet
- Focus 3 2nd Word StoreDocument19 pagesFocus 3 2nd Word StoreSvetlana Bykovshchenko-Tymoshok0% (1)
- Stroke RehabilitationDocument57 pagesStroke RehabilitationWahyu FajarNo ratings yet
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Mathematics of Neural Networks. Models, Algorithms and Applications (PDFDrive)Document423 pagesMathematics of Neural Networks. Models, Algorithms and Applications (PDFDrive)Roy RoyzNo ratings yet
- Hemorrhagic Stroke: Darpen Subhashbhai Mori Group 2, MD 3BDocument13 pagesHemorrhagic Stroke: Darpen Subhashbhai Mori Group 2, MD 3BDarpen MoriNo ratings yet
- Neurorehabilitation 1Document439 pagesNeurorehabilitation 1Duncan D'AmicoNo ratings yet
- Pediatric StrokeDocument90 pagesPediatric StrokeJanaki SethuramanNo ratings yet
- 1 - Rehabilitasi Medik Pada Penderita StrokeDocument55 pages1 - Rehabilitasi Medik Pada Penderita StrokeKrisma susantiNo ratings yet
- Neurology (Cerebrovascular Disease)Document69 pagesNeurology (Cerebrovascular Disease)Mahadhir AkmalNo ratings yet
- Cerebrovascular Accident StrokeDocument3 pagesCerebrovascular Accident StrokeLuis LazaroNo ratings yet
- L2 Hemiplegia and Cerebrovascular Insufficiency (Word)Document7 pagesL2 Hemiplegia and Cerebrovascular Insufficiency (Word)Ashraf NabilNo ratings yet
- Neurological Emergencies d10Document60 pagesNeurological Emergencies d10Diana NurulNo ratings yet
- StrokeDocument113 pagesStrokeSheila SantosNo ratings yet
- ShockDocument1 pageShockWong Liang TungNo ratings yet
- Cerebrovascular Disease: Cva & TbiDocument19 pagesCerebrovascular Disease: Cva & TbiKC MutiaNo ratings yet
- Intracranial HemorrhageDocument75 pagesIntracranial HemorrhageDea DNo ratings yet
- NeuroDocument25 pagesNeurosmpco02No ratings yet
- Stroke Syndromes: Hemiparesis (Faciobrachiocrural Weakness)Document7 pagesStroke Syndromes: Hemiparesis (Faciobrachiocrural Weakness)eko aNo ratings yet
- Cerebrovascular DisordersDocument23 pagesCerebrovascular Disordersbpt2No ratings yet
- Pathology of The CnsDocument38 pagesPathology of The Cnscy lifeNo ratings yet
- Stroke School Brockville Part 3Document39 pagesStroke School Brockville Part 3Gautam KhannaNo ratings yet
- Thalamus Infarct and Clinical PresentationDocument19 pagesThalamus Infarct and Clinical PresentationShin yeeNo ratings yet
- Neuropathology of Aging and DementiaDocument46 pagesNeuropathology of Aging and DementiaDetty NoviantyNo ratings yet
- StrokeDocument27 pagesStrokeJASON KO CHIA SHENGNo ratings yet
- Subarachnoid Haemorrhage (SAH)Document11 pagesSubarachnoid Haemorrhage (SAH)shofianarNo ratings yet
- Neurologic EmergenciesDocument13 pagesNeurologic EmergenciesRENEROSE TORRESNo ratings yet
- Mrs. Keerthana.B Assistant Professor, MSN, PSG ConDocument42 pagesMrs. Keerthana.B Assistant Professor, MSN, PSG ConKeerthana BNo ratings yet
- Stroke PathoDocument15 pagesStroke PathoWiljohn de la CruzNo ratings yet
- Stroke: Dr. Alberto CampodónicoDocument17 pagesStroke: Dr. Alberto CampodónicoJohn Domínguez MedinaNo ratings yet
- Stroke: Nivedita MPT (Neuro)Document27 pagesStroke: Nivedita MPT (Neuro)MenakaNo ratings yet
- NotesDocument1 pageNotesnavkkirangillNo ratings yet
- NS 2 - Developmental Diseases of The Nervous System v2023.02Document49 pagesNS 2 - Developmental Diseases of The Nervous System v2023.02t4gjzhpfjcNo ratings yet
- Intracerebral Hemorrhage, Brain - Flores PDFDocument12 pagesIntracerebral Hemorrhage, Brain - Flores PDFMichael AngNo ratings yet
- Cerebrovascular Disease: Departemen Neurologi Fakultas Kedokteran Universitas Islam Sumatera UtaraDocument48 pagesCerebrovascular Disease: Departemen Neurologi Fakultas Kedokteran Universitas Islam Sumatera UtaraismihabNo ratings yet
- Dr. Endang Elisawaty SpsDocument33 pagesDr. Endang Elisawaty SpsacepNo ratings yet
- Modul Demensia Aging PresentasiDocument43 pagesModul Demensia Aging PresentasiAtika Putri PratiwiNo ratings yet
- Cerebrovascular DiseasesDocument69 pagesCerebrovascular Diseaseshuda dotNo ratings yet
- Subarachnoid Haemorrhage (SAH) : Shofiana Rahmawati 30101407329 Advisor: Dr. Dria Anggraeny S, SP - RadDocument11 pagesSubarachnoid Haemorrhage (SAH) : Shofiana Rahmawati 30101407329 Advisor: Dr. Dria Anggraeny S, SP - RadSepti Dwi SUlistyowatiNo ratings yet
- Neuroradiology Sah and StrokeDocument81 pagesNeuroradiology Sah and StrokeJujhar BoparaiNo ratings yet
- Seminar On Management of StrokeDocument54 pagesSeminar On Management of Stroke7762n9qsntNo ratings yet
- 02.08.13 Carpenter Case Presenation 1Document23 pages02.08.13 Carpenter Case Presenation 1zaimmuhtarNo ratings yet
- 5 Major Stroke Syndromes: Recognition, Action & OutcomesDocument43 pages5 Major Stroke Syndromes: Recognition, Action & OutcomesweezerNo ratings yet
- SyncopeDocument67 pagesSyncopenosloba31No ratings yet
- Heart Failure Idi SidoarjoDocument111 pagesHeart Failure Idi SidoarjoIka Kusuma WardhaniNo ratings yet
- Neurology Shelf Exam Review - Part 3.newDocument12 pagesNeurology Shelf Exam Review - Part 3.newyogurtNo ratings yet
- Head Trauma DR Petra SPBSDocument64 pagesHead Trauma DR Petra SPBSAlessia Wyneini TirzaNo ratings yet
- Cerebellar ExaminationDocument5 pagesCerebellar ExaminationRie Aoyama-Wang100% (1)
- Criterii de Acces Prioritar CradiologieDocument2 pagesCriterii de Acces Prioritar Cradiologievasarhely imolaNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Dementia Recentupdates 130920080812 Phpapp01Document58 pagesDementia Recentupdates 130920080812 Phpapp01SantanuNo ratings yet
- Compiled Stroke RehabDocument121 pagesCompiled Stroke RehabJeel MohtaNo ratings yet
- Ems StrokeDocument29 pagesEms StrokeaathulNo ratings yet
- English Task in Nursing 2 SondaDocument4 pagesEnglish Task in Nursing 2 SondayulisulistiyoNo ratings yet
- sr-SP-Latn Otkazivanje Srca I Cirkulatorni ŠokDocument5 pagessr-SP-Latn Otkazivanje Srca I Cirkulatorni ŠokInes Subotić JakopanecNo ratings yet
- Stroke: Abyot From Harrison, DR Belachew and DR Yared HandoutDocument32 pagesStroke: Abyot From Harrison, DR Belachew and DR Yared HandoutashuNo ratings yet
- Detailed Lesson Plan (DLP) Format Instructional Plan (Iplan) Republic of The Philippines Department of Education Region Vii, Central VisayasDocument5 pagesDetailed Lesson Plan (DLP) Format Instructional Plan (Iplan) Republic of The Philippines Department of Education Region Vii, Central VisayasalexNo ratings yet
- Permanent Monitoring - Looking at Lifetime Reservoir DynamicsDocument15 pagesPermanent Monitoring - Looking at Lifetime Reservoir Dynamicsnoorul786No ratings yet
- Help Seeking As A Self-Regulated Learning Strategy: January 2013Document14 pagesHelp Seeking As A Self-Regulated Learning Strategy: January 2013Agus PratomoNo ratings yet
- LAT111 Lec Notes 9Document6 pagesLAT111 Lec Notes 9boy andrioNo ratings yet
- Flight of The Bumble Bow - Violin IDocument1 pageFlight of The Bumble Bow - Violin IEver Joaco FANo ratings yet
- Wise, Bolls, & Schaefer, 2008Document17 pagesWise, Bolls, & Schaefer, 2008Robert DumitruNo ratings yet
- Major Development Programs and Personalities in The PhilippinesDocument9 pagesMajor Development Programs and Personalities in The Philippinesjoan7casillano7tegerNo ratings yet
- Self-Study Worksheet III Isomerism ANSWERSDocument2 pagesSelf-Study Worksheet III Isomerism ANSWERSkjjkimkmkNo ratings yet
- An Empirical Analysis of Money Demand Function in Nepal: Birendra Bahadur BudhaDocument17 pagesAn Empirical Analysis of Money Demand Function in Nepal: Birendra Bahadur BudhaIsmith PokhrelNo ratings yet
- Presentation By:: Ahmad Ali (829) & Fahad NawazDocument16 pagesPresentation By:: Ahmad Ali (829) & Fahad NawazAhmad AliNo ratings yet
- Krok 1 Physiology 18Document1 pageKrok 1 Physiology 18Sandeep KumarNo ratings yet
- East 43rd Street-Alan BattersbyDocument102 pagesEast 43rd Street-Alan BattersbyVic Thor MoralonsoNo ratings yet
- EN Infonote Frese ALPHA CartridgeDocument2 pagesEN Infonote Frese ALPHA CartridgededeerlandNo ratings yet
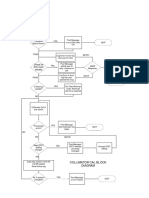
- Check For Dirty Mylar Window: Collimator Cal Block DiagramDocument1 pageCheck For Dirty Mylar Window: Collimator Cal Block DiagramMai Thanh SơnNo ratings yet
- The Electrifying Nikola Tesla!: A Biographical Sketch by Keith BechtolDocument29 pagesThe Electrifying Nikola Tesla!: A Biographical Sketch by Keith BechtolNithin ChandranNo ratings yet
- Advertising & The End of The World Study GuideDocument25 pagesAdvertising & The End of The World Study Guideschole60No ratings yet
- English: Quarter 2, Wk.3 - Module 1 Give The Appropriate Communicative Styles For Various SituationsDocument11 pagesEnglish: Quarter 2, Wk.3 - Module 1 Give The Appropriate Communicative Styles For Various SituationsRyan Custodio MarcosNo ratings yet
- 301 enDocument263 pages301 enFedja NetjasovNo ratings yet
- 07 Subject Verb AgreementDocument14 pages07 Subject Verb AgreementMehak SrivastavaNo ratings yet
- SADI Notes S10 11 - StephDocument38 pagesSADI Notes S10 11 - StephKhagesh JoshNo ratings yet
- Lecture 4:sampling and Reconstruction: - Sampling - Data Reconstruction (Hold) - Reading: Chapter 3 of The TextbookDocument15 pagesLecture 4:sampling and Reconstruction: - Sampling - Data Reconstruction (Hold) - Reading: Chapter 3 of The TextbookmumtazNo ratings yet
- University of Okara: 4th Merit List Department:School of Law Admissions:FALL 2020Document2 pagesUniversity of Okara: 4th Merit List Department:School of Law Admissions:FALL 2020Saghar Asi AwanNo ratings yet
- Procedure SDI TestDocument2 pagesProcedure SDI TestChairul ImamNo ratings yet
- Brain Activity During Second Language Processing (ERP)Document7 pagesBrain Activity During Second Language Processing (ERP)Su AjaNo ratings yet
- EE5630 - EE5660 - Exam - Main - FinalDocument5 pagesEE5630 - EE5660 - Exam - Main - FinalMadalin PetrachiNo ratings yet
- WellSpa Io HUT3 NDADocument3 pagesWellSpa Io HUT3 NDAardiNo ratings yet