You might also like
- Breast Cancer 1Document35 pagesBreast Cancer 1Tamalika GhosalNo ratings yet
- Penis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPenis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Breast Edema: Causes, Imaging Findings and ManagementDocument258 pagesBreast Edema: Causes, Imaging Findings and ManagementMartin AmoresNo ratings yet
- Breast Diseases: Detection and Physical ExamDocument22 pagesBreast Diseases: Detection and Physical ExamnicewanNo ratings yet
- Embryology and Functional Anatomy of The BreastDocument20 pagesEmbryology and Functional Anatomy of The BreastseidkeNo ratings yet
- Breast DiseasesDocument47 pagesBreast DiseasesDR/ AL-saifiNo ratings yet
- Pathology and Management of Benign Breast DiseasesDocument58 pagesPathology and Management of Benign Breast DiseasesisuhuNo ratings yet
- BreastDocument27 pagesBreastRasha HelmyNo ratings yet
- Ana211 Breast and Lymphatic DrainageDocument4 pagesAna211 Breast and Lymphatic DrainageKalu ComforterNo ratings yet
- Surgical Anatomy of The Breast T-HAZEM - CompressedDocument28 pagesSurgical Anatomy of The Breast T-HAZEM - CompressedmohamedhazemelfollNo ratings yet
- The BreastDocument199 pagesThe BreastI.k sidneyNo ratings yet
- BREAST-Dr-Japagat 2Document130 pagesBREAST-Dr-Japagat 2Aanand MandalNo ratings yet
- Assessing Breasts and Lymphatic SystemDocument5 pagesAssessing Breasts and Lymphatic SystemGiselle EstoquiaNo ratings yet
- Ca BreastDocument64 pagesCa Breastadina.batajuNo ratings yet
- Embryonic Breast Development and MalformationsDocument96 pagesEmbryonic Breast Development and MalformationsSalim Mwiti NabeaNo ratings yet
- The Breasts - Structure - Vasculature - TeachMeAnatomyDocument4 pagesThe Breasts - Structure - Vasculature - TeachMeAnatomywzt2001No ratings yet
- Breast Lumps GuideDocument55 pagesBreast Lumps GuideUmar AzlanNo ratings yet
- BREAST DISORDER GUIDEDocument102 pagesBREAST DISORDER GUIDESuryooNo ratings yet
- Unit 1 - Breast Anatomy and PhysiologyDocument50 pagesUnit 1 - Breast Anatomy and PhysiologyClyde R.OrtegaNo ratings yet
- 4 1Document265 pages4 1sillypoloNo ratings yet
- BreastDocument158 pagesBreastRichard AlboroNo ratings yet
- AnatDocument45 pagesAnatRinxas VerinxtNo ratings yet
- Lec#17 Benign Breast ConditionsDocument67 pagesLec#17 Benign Breast ConditionsBalqees abusahuonNo ratings yet
- Breast: Baconga, KeziahDocument153 pagesBreast: Baconga, KeziahPaul Valdez100% (2)
- Patho5-2 - Breast (Dr. Yanez)Document10 pagesPatho5-2 - Breast (Dr. Yanez)Miguel Cuevas DolotNo ratings yet
- Breast Anatomy and Development GuideDocument8 pagesBreast Anatomy and Development Guidekamie155No ratings yet
- 1.anatomi MammaeDocument15 pages1.anatomi MammaeKatou Jeffrey ShigehitoNo ratings yet
- VIII. Anatomy and PhysiologyDocument5 pagesVIII. Anatomy and PhysiologyTrixie Al MarieNo ratings yet
- Prof Galal Surgical-Oncology-notes 2023Document57 pagesProf Galal Surgical-Oncology-notes 2023Sara AbdoNo ratings yet
- Ca BreastDocument92 pagesCa BreastKirubakaran Saraswathy PattabiramanNo ratings yet
- Open Breast Disorders (Benign and Malignant) DoneDocument117 pagesOpen Breast Disorders (Benign and Malignant) Donereema.saleh123No ratings yet
- Path o PhysiologyDocument11 pagesPath o PhysiologyKimm Charmaine RodriguezNo ratings yet
- The BreastsDocument20 pagesThe BreastsAmeer MattaNo ratings yet
- Mammary Gland Structure and DevelopmentDocument22 pagesMammary Gland Structure and DevelopmentAaronMaroonFiveNo ratings yet
- OR Write UPDocument10 pagesOR Write UPMimiberNo ratings yet
- Breast ExaminationDocument16 pagesBreast Examinationjackfruit5887No ratings yet
- Focus Data Action Response SDocument5 pagesFocus Data Action Response SMeynard AndresNo ratings yet
- MastectomyDocument52 pagesMastectomyCogie SalvadorNo ratings yet
- Congenital Abnormalities of The UterusDocument7 pagesCongenital Abnormalities of The Uterusمحمود الموسويNo ratings yet
- Breast Cancer by Professor B. T. UgwuDocument16 pagesBreast Cancer by Professor B. T. UgwuMusaNo ratings yet
- Breast: 1 EtymologyDocument13 pagesBreast: 1 EtymologynathanNo ratings yet
- Davao Doctors College Total Abdominal Hysterectomy PaperDocument19 pagesDavao Doctors College Total Abdominal Hysterectomy PaperHazel Endaya0% (1)
- Case Discussion Ductal CADocument27 pagesCase Discussion Ductal CASimon Peter MollanedaNo ratings yet
- Tabark Radhi - Benign Breast NeoplasmDocument19 pagesTabark Radhi - Benign Breast NeoplasmAhmed AliNo ratings yet
- AnatomicallyDocument3 pagesAnatomicallyAjayDeep NallabothulaNo ratings yet
- Case Study About Cervical CancerDocument11 pagesCase Study About Cervical CancerJisel-Apple Bulan100% (1)
- Breast anatomy overviewDocument59 pagesBreast anatomy overviewgina2535100% (1)
- 41 Female Reproductive AnatomyDocument14 pages41 Female Reproductive Anatomyruaa firasNo ratings yet
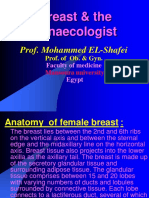
- Breast & The Gynaecologist: Prof. Mohammed EL-ShafeiDocument17 pagesBreast & The Gynaecologist: Prof. Mohammed EL-ShafeiAhmed BassettNo ratings yet
- 5 6057345046456304562Document490 pages5 6057345046456304562DK DeepakNo ratings yet
- Upper Limb BreastDocument40 pagesUpper Limb BreastewijayapalaNo ratings yet
- Case Study MastectomyDocument26 pagesCase Study MastectomyIcheAnne Nilay100% (2)
- Colposcopy CourseDocument50 pagesColposcopy CourseNam Le100% (1)
- Understanding Hysterectomy: A Guide to the Surgical ProcedureDocument22 pagesUnderstanding Hysterectomy: A Guide to the Surgical ProcedureGinger Enireht HTaibNo ratings yet
- Mammography. NotesDocument9 pagesMammography. Notescorrainnejimenez.24No ratings yet
- LP Tumor Mamae OkDocument13 pagesLP Tumor Mamae OkDiban namiNo ratings yet
- Breast: Anatomy & PhysiologyDocument6 pagesBreast: Anatomy & PhysiologyironNo ratings yet
- Breast Anatomy With Clinical CorrelationDocument27 pagesBreast Anatomy With Clinical CorrelationDionix Cruz100% (2)
- Student Name: ALI HASSAN RAZA STUDENT I D: 2018304027Document6 pagesStudent Name: ALI HASSAN RAZA STUDENT I D: 2018304027Sayed AsifNo ratings yet
- Bascon postoperativeNCP DischargeplanDocument4 pagesBascon postoperativeNCP DischargeplanLacangan, Thea YvonneNo ratings yet
- For Mock DefenseDocument9 pagesFor Mock DefenseLacangan, Thea YvonneNo ratings yet
- Group 5 BSN 3aDocument12 pagesGroup 5 BSN 3aLacangan, Thea YvonneNo ratings yet
- Ecs TableDocument1 pageEcs TableLacangan, Thea YvonneNo ratings yet
- Review Related LiteraturesDocument2 pagesReview Related LiteraturesLacangan, Thea YvonneNo ratings yet
- 03 OR Case Study For October 17 - 18Document1 page03 OR Case Study For October 17 - 18Lacangan, Thea YvonneNo ratings yet
- Case 3 - Question 3Document2 pagesCase 3 - Question 3Lacangan, Thea YvonneNo ratings yet
- Duty ScheduleDocument1 pageDuty ScheduleLacangan, Thea YvonneNo ratings yet
- Research Title Proposal 2Document4 pagesResearch Title Proposal 2Lacangan, Thea YvonneNo ratings yet
- Rizal's Teachers at Ateneo de Municipal and USTDocument7 pagesRizal's Teachers at Ateneo de Municipal and USTLacangan, Thea YvonneNo ratings yet
- Multiple Myeloma ReportDocument21 pagesMultiple Myeloma ReportLacangan, Thea YvonneNo ratings yet
- Effects of Sex Ed on Teen PregnancyDocument11 pagesEffects of Sex Ed on Teen PregnancyLacangan, Thea YvonneNo ratings yet
- Research Title ProposalDocument15 pagesResearch Title ProposalLacangan, Thea YvonneNo ratings yet
- Mask offDocument4 pagesMask offLacangan, Thea YvonneNo ratings yet
- Impact of COVID-19 Vaccination Requirement in Employment on Willingness to WorkDocument2 pagesImpact of COVID-19 Vaccination Requirement in Employment on Willingness to WorkLacangan, Thea YvonneNo ratings yet
- ResearchDocument3 pagesResearchLacangan, Thea YvonneNo ratings yet
- Research Study 1 QuestionnairesDocument2 pagesResearch Study 1 QuestionnairesLacangan, Thea YvonneNo ratings yet
- Educational System in Ateneo - Group 1 1Document13 pagesEducational System in Ateneo - Group 1 1Lacangan, Thea YvonneNo ratings yet
- eThink Training UC StudentsDocument5 pageseThink Training UC StudentsLacangan, Thea YvonneNo ratings yet
- Fluid and Electrolyte - 2022Document147 pagesFluid and Electrolyte - 2022Lacangan, Thea YvonneNo ratings yet
- Module 2 - Fluid and ElectrolytesDocument3 pagesModule 2 - Fluid and ElectrolytesLacangan, Thea YvonneNo ratings yet
- Oncology:: Nursing Management in Cancer CareDocument39 pagesOncology:: Nursing Management in Cancer CareRika Mae DiamosNo ratings yet
- NSTP102 Chapter 2Document19 pagesNSTP102 Chapter 2Lacangan, Thea YvonneNo ratings yet
- Anti Parkinsonism AgentsDocument16 pagesAnti Parkinsonism AgentsLacangan, Thea YvonneNo ratings yet
- Salazar Medicine TicketDocument1 pageSalazar Medicine TicketLacangan, Thea YvonneNo ratings yet
- Final Presentation of Cose Credo - Muscle RelaxantsDocument21 pagesFinal Presentation of Cose Credo - Muscle RelaxantsLacangan, Thea YvonneNo ratings yet
- NCM 107 LectureDocument1 pageNCM 107 LectureLacangan, Thea YvonneNo ratings yet
- Group 2Document7 pagesGroup 2Lacangan, Thea YvonneNo ratings yet
- Case Study - LacanganDocument5 pagesCase Study - LacanganLacangan, Thea YvonneNo ratings yet
- CHANCROIDDocument27 pagesCHANCROIDnfacmaNo ratings yet
- Jama Zhou 2023 It 230012 1694198870.80806Document2 pagesJama Zhou 2023 It 230012 1694198870.80806William TapiaNo ratings yet
- Acquired Coagulation DisordersDocument11 pagesAcquired Coagulation DisordersAli AhmedNo ratings yet
- 4209 ArticleText 15346 1 10 202101142020Document15 pages4209 ArticleText 15346 1 10 202101142020Selmitha SariNo ratings yet
- Antimicrobial Susceptibility Testing PDFDocument19 pagesAntimicrobial Susceptibility Testing PDFdatitoxNo ratings yet
- 641 1769 1 PBDocument8 pages641 1769 1 PBHira DamayantiNo ratings yet
- Zirconnia Knife Edge PDFDocument6 pagesZirconnia Knife Edge PDFMuaiyed Buzayan AkremyNo ratings yet
- Recurrence of Pulmonary Intravascular BRDocument79 pagesRecurrence of Pulmonary Intravascular BRMikmik bay BayNo ratings yet
- Heart and Neck Vessels AssDocument5 pagesHeart and Neck Vessels AssJayson OlileNo ratings yet
- UltramageDocument12 pagesUltramagegi vrgsNo ratings yet
- Group1 Week8298Document54 pagesGroup1 Week8298ABEGAIL BALLORANNo ratings yet
- List of Empanelled Hospitals Updated 01032023Document24 pagesList of Empanelled Hospitals Updated 01032023ARIZ HAMIDNo ratings yet
- 18 OctDocument82 pages18 OctAseel AlsheeshNo ratings yet
- Kl355, KTD (Optha) : Allopathy Post Graduate Doct RsDocument54 pagesKl355, KTD (Optha) : Allopathy Post Graduate Doct RsKirti Raj0% (1)
- Medication Errors: 12 Questions Patients Should Ask Their Doctors and PharmacistsDocument30 pagesMedication Errors: 12 Questions Patients Should Ask Their Doctors and PharmacistsVero YosaNo ratings yet
- Two New Loci for Systemic Lupus Erythematosus IdentifiedDocument2 pagesTwo New Loci for Systemic Lupus Erythematosus IdentifiedPratidina Dwinda HENo ratings yet
- She Drug StudyDocument23 pagesShe Drug StudyShella DechavezNo ratings yet
- Obesity Powerpoint G-5Document14 pagesObesity Powerpoint G-5cheryl tubliganNo ratings yet
- Summary of Teachers TrainedDocument7 pagesSummary of Teachers TrainedkrishnaNo ratings yet
- Krisis HipertensiDocument29 pagesKrisis HipertensiMuarifNo ratings yet
- Scope of Nursing CareersDocument33 pagesScope of Nursing Careersmaria jacobNo ratings yet
- Trichinella Spiralis and Enterobius VermicularisDocument24 pagesTrichinella Spiralis and Enterobius VermicularisJoseph Christian Bielgo CuaNo ratings yet
- Methods You Can Overcome Plus Deal With DepressionDocument2 pagesMethods You Can Overcome Plus Deal With DepressionGunnWinstead6No ratings yet
- SWIFS Office of The Medical Examiner General Policy and Procedures, 128 Pages (01.03.2008)Document128 pagesSWIFS Office of The Medical Examiner General Policy and Procedures, 128 Pages (01.03.2008)jac_blakeNo ratings yet
- A Case Study On Septic ShockDocument51 pagesA Case Study On Septic ShockKeThSantibanNo ratings yet
- Government of KeralaDocument9 pagesGovernment of KeralaMubashirNo ratings yet
- MKSAP13-Pulmonary Medicine and Critical CareDocument85 pagesMKSAP13-Pulmonary Medicine and Critical CaresarfirazNo ratings yet
- Present Perfect + ILLNESSESDocument4 pagesPresent Perfect + ILLNESSESEdyta MichalakNo ratings yet
- WBC MorphologyDocument47 pagesWBC MorphologyMuhammad ZakriaNo ratings yet
- Lang 2020Document8 pagesLang 2020Asmaa GamalNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)