You might also like
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineDocument26 pagesDr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineJose Fernando PereiraNo ratings yet
- Cross Connection ManualDocument122 pagesCross Connection ManualHESuarezNo ratings yet
- Genius Insight APP User Manual 2.1Document51 pagesGenius Insight APP User Manual 2.1Jain SumeetNo ratings yet
- 6379 Topper 21 129 510 2 2192 Gaseous State Up201612091655 1481282727 7964Document47 pages6379 Topper 21 129 510 2 2192 Gaseous State Up201612091655 1481282727 7964BhootNo ratings yet
- A Marketing Plan of Jack Fruites JuiceDocument25 pagesA Marketing Plan of Jack Fruites JuiceNazrul Islam100% (3)
- Gases & The Kinetic-Molecular TheoryDocument20 pagesGases & The Kinetic-Molecular TheoryAshley Marie ChildersNo ratings yet
- Worksheet GasesDocument6 pagesWorksheet GasesakladffjaNo ratings yet
- Vietnam Studies Base Development in South Vietnam 1965-1970Document175 pagesVietnam Studies Base Development in South Vietnam 1965-1970Bob Andrepont100% (2)
- Chapter 5 - Pricing Forwards and Futures (S.V.)Document39 pagesChapter 5 - Pricing Forwards and Futures (S.V.)flippy23No ratings yet
- Physics II - EngineeringG PDFDocument110 pagesPhysics II - EngineeringG PDFRami JarrarNo ratings yet
- Oracle Applications 11i: Bill of MaterialsDocument79 pagesOracle Applications 11i: Bill of Materialssaqi22No ratings yet
- Gas LawsDocument42 pagesGas LawsCharmy Delos Reyes AtabayNo ratings yet
- Gas Laws Worksheetsand SolutionsDocument9 pagesGas Laws Worksheetsand SolutionskjgfsogkpsNo ratings yet
- SM 11Document245 pagesSM 11Paulo Gomes de Souza50% (2)
- GLWS9Document6 pagesGLWS9Vince HernándezNo ratings yet
- Physical, Inorganic & Organic Chem QnsDocument45 pagesPhysical, Inorganic & Organic Chem QnsMarvin NdashimyeNo ratings yet
- Gas LawsDocument69 pagesGas LawsXandra CallantaNo ratings yet
- Gas Laws I SP 1617 (PreAP)Document3 pagesGas Laws I SP 1617 (PreAP)Nikhil Singh100% (1)
- AP Chemistry Chapter 10Document87 pagesAP Chemistry Chapter 10Debalina DassNo ratings yet
- States of MatterDocument6 pagesStates of MatterSiddhant KarmarkarNo ratings yet
- Tutorial 9 - CHM420 - Sept 2020Document2 pagesTutorial 9 - CHM420 - Sept 2020Hai AwakNo ratings yet
- Worksheet - 2 (Gas Laws, Density, Molar Mass)Document4 pagesWorksheet - 2 (Gas Laws, Density, Molar Mass)Jose Ruben SortoNo ratings yet
- Worksheet On GAS LAWS and STOICHIOMETRYDocument2 pagesWorksheet On GAS LAWS and STOICHIOMETRYKenneth ComabigNo ratings yet
- Academy For Foun Dation Education in Math & Scien CeDocument5 pagesAcademy For Foun Dation Education in Math & Scien CeprabhakarmetNo ratings yet
- Gaseous State DPP - 5 & 6Document2 pagesGaseous State DPP - 5 & 6kan PadmasreeNo ratings yet
- Extra Exercise Chapter 5Document7 pagesExtra Exercise Chapter 5Veshal RameshNo ratings yet
- Assignment 1 ThermodynamicsDocument1 pageAssignment 1 ThermodynamicsMarvin BayanayNo ratings yet
- Tutorial 6Document3 pagesTutorial 6DanielNo ratings yet
- Physical Chemistry 1 Prob SetDocument8 pagesPhysical Chemistry 1 Prob SetArrianne Jaye MataNo ratings yet
- Ideal Gases ProblemsDocument2 pagesIdeal Gases ProblemsAngel Ruben Peraza GuadarramaNo ratings yet
- Chemistry 5.2-5.5Document4 pagesChemistry 5.2-5.5Arthur AguijonNo ratings yet
- Decomposição Do Clorato de PotássioDocument5 pagesDecomposição Do Clorato de PotássioVitorArrudaNo ratings yet
- Ideal Gas LawsDocument43 pagesIdeal Gas LawsRenz FerrerNo ratings yet
- Gas Laws Problem Set (Edited)Document2 pagesGas Laws Problem Set (Edited)Kurt Bidua0% (1)
- Ideal Gas LawDocument1 pageIdeal Gas LawLarry BugaringNo ratings yet
- Gas Laws in Anesth Machine-2Document77 pagesGas Laws in Anesth Machine-2Ravikiran SuryanarayanamurthyNo ratings yet
- Intervention in General Chemistry 1Document2 pagesIntervention in General Chemistry 1Arnold PaombongNo ratings yet
- Problem Set Gases Due After Midterm ExamDocument8 pagesProblem Set Gases Due After Midterm ExamMorsid LipolesNo ratings yet
- Exp 15 Molecular Weight Determination of VaporDocument7 pagesExp 15 Molecular Weight Determination of Vapor25edwardslNo ratings yet
- Garg Study Centre: Gaseous StateDocument2 pagesGarg Study Centre: Gaseous StateveerlocusNo ratings yet
- Acetylene Reduction AssayDocument2 pagesAcetylene Reduction AssayGregorius Baskara Aji Nugraha50% (2)
- Class XI Assignment States of MatterDocument2 pagesClass XI Assignment States of MatterCheryl ChaudhariNo ratings yet
- Cpp-Gaseous State - RGVDocument2 pagesCpp-Gaseous State - RGVGauri KabraNo ratings yet
- Gasometric AssaysDocument8 pagesGasometric AssaysKalidhas YogarajanNo ratings yet
- Chapter 5 Gases HW QuestionsDocument2 pagesChapter 5 Gases HW QuestionsChristopher BullNo ratings yet
- Gas LawsDocument13 pagesGas LawsVenkatNo ratings yet
- Gaseous StateDocument12 pagesGaseous StateRaju Singh0% (1)
- U8 hw-18Document5 pagesU8 hw-18api-368121935No ratings yet
- Activities in Science 10 For 4th GradingDocument2 pagesActivities in Science 10 For 4th GradingAE LLANo ratings yet
- Exc 7 Gas SM 09Document3 pagesExc 7 Gas SM 09Tushar AgrawalNo ratings yet
- Tugas #1 OKDocument2 pagesTugas #1 OKfitriNo ratings yet
- Tutorial Sheet 4 - GASES. CH 110 2022Document1 pageTutorial Sheet 4 - GASES. CH 110 2022Bonaventure MasekoNo ratings yet
- 4.ideal GasDocument27 pages4.ideal GasSam KumarNo ratings yet
- Gas LawsDocument2 pagesGas LawsRaleen GenerNo ratings yet
- Tutorial 6Document2 pagesTutorial 6Anis AzwaNo ratings yet
- 9th+class Gas+laws Chmistry+material+ (CMD)Document11 pages9th+class Gas+laws Chmistry+material+ (CMD)Karthik NNo ratings yet
- Chapter 10 Powerpoint - Student VersionDocument95 pagesChapter 10 Powerpoint - Student VersionAnj LTNo ratings yet
- Gas LawsDocument3 pagesGas LawsZynn Margarette DenostaNo ratings yet
- Boyles LawDocument4 pagesBoyles LawJaneNo ratings yet
- AP Chemistry Fr3 Test BankDocument9 pagesAP Chemistry Fr3 Test BankzeustamNo ratings yet
- Chapter 11 - Gas LawsDocument55 pagesChapter 11 - Gas Lawsjim tannerNo ratings yet
- Tutorial Gaseous State CHM131Document2 pagesTutorial Gaseous State CHM131asyhqnaNo ratings yet
- Chapter 6Document18 pagesChapter 6NurhayatiNo ratings yet
- Pysical QuestionsDocument1 pagePysical QuestionsBrainport SageNo ratings yet
- 9 - Unit 6 - WS - Gases Laws ReviewDocument2 pages9 - Unit 6 - WS - Gases Laws ReviewAdam BurnettNo ratings yet
- Chapter 5 Gases Homework1Document3 pagesChapter 5 Gases Homework1Mary JewelNo ratings yet
- Thegaslawscomplete 120227061412 Phpapp01Document51 pagesThegaslawscomplete 120227061412 Phpapp01Bustami Muhammad Sidik100% (1)
- Stiffener and DoublerDocument70 pagesStiffener and DoublerJayNo ratings yet
- Performing Arts Medicine Ostwald PFDocument6 pagesPerforming Arts Medicine Ostwald PFBruni LopezNo ratings yet
- Foxboro™ SCADA SCD6000 RTU Architectural Overview - 41h8g7Document18 pagesFoxboro™ SCADA SCD6000 RTU Architectural Overview - 41h8g7Muhd Nu'man HNo ratings yet
- Lemuel Ticman Clarif Meeting No. 1Document3 pagesLemuel Ticman Clarif Meeting No. 1Vholts Villa VitugNo ratings yet
- Innovative Teaching Manual: Submitted byDocument7 pagesInnovative Teaching Manual: Submitted byPrasant NatarajanNo ratings yet
- Cloud Computing Dissertation PDFDocument7 pagesCloud Computing Dissertation PDFCollegePapersHelpManchester100% (1)
- The Planning Process in Clothing ManufactureDocument9 pagesThe Planning Process in Clothing ManufactureTANYA TANYANo ratings yet
- New Mazda Cars Singapore Car Prices & Listing - SgcarmartDocument1 pageNew Mazda Cars Singapore Car Prices & Listing - SgcarmartdnanevermoreNo ratings yet
- P3F30 en M C004 WebDocument368 pagesP3F30 en M C004 WebdyjimenezNo ratings yet
- Hypoelastic ModelDocument12 pagesHypoelastic Modelhalil yıldırımNo ratings yet
- The Seven Tools of Causal Inference,: With Reflections On Machine LearningDocument7 pagesThe Seven Tools of Causal Inference,: With Reflections On Machine LearningdkNo ratings yet
- My First Inspiration By: Jose RizalDocument5 pagesMy First Inspiration By: Jose RizalMavic Jaictin Bagondol SemaNo ratings yet
- I.The Importance of The NewspaperDocument8 pagesI.The Importance of The Newspaperngo9287No ratings yet
- Separation and Quantification of LignansDocument9 pagesSeparation and Quantification of Lignanskhusnan fadliNo ratings yet
- Evolving Your View of Thermodilution: Volumeview SetDocument4 pagesEvolving Your View of Thermodilution: Volumeview Setalejandro sanche mejoradaNo ratings yet
- Properties of Gastric JuiceDocument17 pagesProperties of Gastric Juicejyoti kunduNo ratings yet
- Vektor Ablerex-800L - 1000L-TearsheetDocument1 pageVektor Ablerex-800L - 1000L-TearsheetJhonSitanalaNo ratings yet
- Biological Molecule (Nucleid Acids) ObjDocument5 pagesBiological Molecule (Nucleid Acids) ObjYing ShuangNo ratings yet
- Acid Gas Comp 120 MMSCFD 3 Mol% H2SDocument1 pageAcid Gas Comp 120 MMSCFD 3 Mol% H2SGreg EverettNo ratings yet
- Worksheet Partial in DerivativesDocument2 pagesWorksheet Partial in DerivativesVanessa HardjadinataNo ratings yet
- TM 2 Fundamentals of Organic Chemistry 7th Edition by John McMurryDocument15 pagesTM 2 Fundamentals of Organic Chemistry 7th Edition by John McMurrysukma AsaNo ratings yet
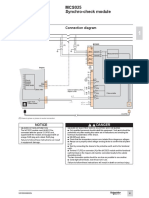
- MCS025 Synchro-Check Module: InstallationDocument1 pageMCS025 Synchro-Check Module: Installationوسام وسامNo ratings yet