You might also like
- Medical Surgical Nursing Module 14Document31 pagesMedical Surgical Nursing Module 14weissNo ratings yet
- Medical Surgical Nursing Module 4Document17 pagesMedical Surgical Nursing Module 4weissNo ratings yet
- Ms Pain and Surgery ModulesDocument30 pagesMs Pain and Surgery ModulesweissNo ratings yet
- MSN Communicable DiseaseDocument29 pagesMSN Communicable DiseaseLuis LazaroNo ratings yet
- Medical Surgical Nursing Module 7Document18 pagesMedical Surgical Nursing Module 7weissNo ratings yet
- Medical Surgical Nursing Module 9Document8 pagesMedical Surgical Nursing Module 9weissNo ratings yet
- Medical Surgical Nursing Module 6Document8 pagesMedical Surgical Nursing Module 6weissNo ratings yet
- Medical Surgical Nursing Module 8Document9 pagesMedical Surgical Nursing Module 8weissNo ratings yet
- Cte #2: Matrix of Communicable DiseasesDocument7 pagesCte #2: Matrix of Communicable Diseasesjoannamae molagaNo ratings yet
- Medical Surgical Nursing Module 11Document26 pagesMedical Surgical Nursing Module 11weissNo ratings yet
- Hand Out For Module 1.5Document17 pagesHand Out For Module 1.5weissNo ratings yet
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- Hand-out-For-Module-1.3 or Attire, Surgical Hand Scrubbing, Gowning, Closed Gloving, and InstrumentationDocument26 pagesHand-out-For-Module-1.3 or Attire, Surgical Hand Scrubbing, Gowning, Closed Gloving, and Instrumentationweiss100% (1)
- Intracranial Hypertension or Increased ICPDocument11 pagesIntracranial Hypertension or Increased ICPRomina Irish MatutinoNo ratings yet
- Med Surg 2 - 1 Review of Anatomy and Physiology of The GIT and Accessory OrgansDocument8 pagesMed Surg 2 - 1 Review of Anatomy and Physiology of The GIT and Accessory OrgansMaxinne RoseñoNo ratings yet
- Trans 1 Medication Administration 1Document23 pagesTrans 1 Medication Administration 1Germin CesaNo ratings yet
- Pain and Surgery TransDocument44 pagesPain and Surgery TransweissNo ratings yet
- Maternal and Child Health Nursing Reviewer Compiled by NURSEHOOMANDocument122 pagesMaternal and Child Health Nursing Reviewer Compiled by NURSEHOOMANL Rean Carmelle MAGALLONESNo ratings yet
- Nursing Care of Clients With Upper Airway or Respiratory DisordersDocument6 pagesNursing Care of Clients With Upper Airway or Respiratory DisordersLuna MarieNo ratings yet
- Roller Bandages: Head BandageDocument9 pagesRoller Bandages: Head BandageNicole AlemaniaNo ratings yet
- Cholinergics & AnticholinergicsDocument7 pagesCholinergics & AnticholinergicsKimberly MunsayacNo ratings yet
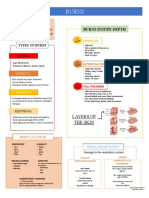
- BurnsDocument3 pagesBurnsCerezo, Cherrieus Ann C.No ratings yet
- Health Assessment LectureDocument48 pagesHealth Assessment LectureJade Buri100% (1)
- Nanoparticle Drug Delivery System: Apt. Fitri Wulandari, M.Clin - PharmDocument18 pagesNanoparticle Drug Delivery System: Apt. Fitri Wulandari, M.Clin - PharmDian GabriellaNo ratings yet
- Psych ReportDocument80 pagesPsych ReportPaul Carlo GonzalesNo ratings yet
- NCM 116 Medical Surgical ReviewerDocument18 pagesNCM 116 Medical Surgical ReviewerClark Evan PillonarNo ratings yet
- Infectious Disease Awareness In, Mogadishu, SomaliaDocument7 pagesInfectious Disease Awareness In, Mogadishu, Somaliashafie Mohamed AliNo ratings yet
- Cell Ab Midterm MesiDocument7 pagesCell Ab Midterm MesiSamantha VeraNo ratings yet
- Medical Surgical Nursing Module 12Document45 pagesMedical Surgical Nursing Module 12weissNo ratings yet
- 2 - BPE - Eye ExaminationDocument50 pages2 - BPE - Eye ExaminationZauhar NurdildayevaNo ratings yet
- Pneumo Tot MergedDocument103 pagesPneumo Tot MergedAndra BauerNo ratings yet
- Assessment of The Eyes STUDENTDocument7 pagesAssessment of The Eyes STUDENTRolandNo ratings yet
- Assignment Anatomy 1 Lower Limb FolioDocument46 pagesAssignment Anatomy 1 Lower Limb FolioAmelia JupirinNo ratings yet
- Assessing Level of Consciouness Activity - StudentDocument2 pagesAssessing Level of Consciouness Activity - Studentapi-651287771No ratings yet
- Hand-out-For-Module-1.4 Pre, Intra, and Post Op Patient CareDocument24 pagesHand-out-For-Module-1.4 Pre, Intra, and Post Op Patient CareweissNo ratings yet
- Electrolytes (3607)Document11 pagesElectrolytes (3607)JennNo ratings yet
- Lec-4 Upper and Lower Git DisordersDocument101 pagesLec-4 Upper and Lower Git DisordersSaher YasinNo ratings yet
- Skin, Hair, Nails Assessment NotesDocument6 pagesSkin, Hair, Nails Assessment NotesRolandNo ratings yet
- Pharma NotesDocument18 pagesPharma Notesseanne kskwkwkaNo ratings yet
- PEDIA Review TransesDocument12 pagesPEDIA Review TransesJennie KimNo ratings yet
- Assessing AbdomenDocument7 pagesAssessing AbdomenJa DimasNo ratings yet
- PharmaDocument6 pagesPharmaLovely AmadoNo ratings yet
- Learning: St. Mary'S College of Tagum, IncDocument37 pagesLearning: St. Mary'S College of Tagum, IncAlyssa Gaile EspirituNo ratings yet
- Pharmacotherapy of ArrythmiasDocument68 pagesPharmacotherapy of ArrythmiasABREHAM BUKULONo ratings yet
- The Respiratory System and Its DisordersDocument16 pagesThe Respiratory System and Its DisordersZea Leyan J. LopezNo ratings yet
- Week 4 - Drugs Acting On The Immune SystemDocument16 pagesWeek 4 - Drugs Acting On The Immune SystemDino MicaNo ratings yet
- Anatomy of The Lower Extremity - Hirsch TextbookDocument546 pagesAnatomy of The Lower Extremity - Hirsch TextbookAkash ShahNo ratings yet
- Pe (Hurdles & Javelin)Document20 pagesPe (Hurdles & Javelin)Cyrus FernzNo ratings yet
- Sas#3 - Ite 303-SiaDocument11 pagesSas#3 - Ite 303-SiaFranzh Lawrence BataanNo ratings yet
- Anatomy - Physiology (Chapter 6 - Skeletal System)Document39 pagesAnatomy - Physiology (Chapter 6 - Skeletal System)Avi ZychNo ratings yet
- Fluids and Renal DisorderDocument139 pagesFluids and Renal DisorderLhara MañoNo ratings yet
- Otosclerosis and Menieres DiseaseDocument5 pagesOtosclerosis and Menieres DiseaseYoko Mae YanoNo ratings yet
- Brunnstrom's Movement TherapyDocument81 pagesBrunnstrom's Movement TherapyAjju NagarNo ratings yet
- PulseDocument13 pagesPulseArdi EroNo ratings yet
- Nur 111 Session 3 Sas 1Document8 pagesNur 111 Session 3 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- A Systematic Review On Dementia CareDocument5 pagesA Systematic Review On Dementia CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Msn-Pain - SurgeryDocument45 pagesMsn-Pain - SurgeryweissNo ratings yet
- Central Nervous System Examination: Overview & PurposeDocument5 pagesCentral Nervous System Examination: Overview & PurposebismahNo ratings yet
- Sas 21Document4 pagesSas 21Sistine Rose LabajoNo ratings yet
- TONSILITIS AND ADENOIDITIS - Baldoza.E.Document9 pagesTONSILITIS AND ADENOIDITIS - Baldoza.E.Monette Abalos MendovaNo ratings yet
- Medical Surgical Nursing Module 8Document9 pagesMedical Surgical Nursing Module 8weissNo ratings yet
- Medical Surgical Nursing Module 10Document34 pagesMedical Surgical Nursing Module 10weissNo ratings yet
- Medical Surgical Nursing Module 17Document31 pagesMedical Surgical Nursing Module 17weissNo ratings yet
- Medical Surgical Nursing Module 9Document8 pagesMedical Surgical Nursing Module 9weissNo ratings yet
- Medical Surgical Nursing Module 6Document8 pagesMedical Surgical Nursing Module 6weissNo ratings yet
- Cardio TransDocument7 pagesCardio TransweissNo ratings yet
- Medical Surgical Nursing Module 11Document26 pagesMedical Surgical Nursing Module 11weissNo ratings yet
- Medical Surgical Nursing Module 12Document45 pagesMedical Surgical Nursing Module 12weissNo ratings yet
- Pain and Surgery TransDocument44 pagesPain and Surgery TransweissNo ratings yet
- Medical Surgical Nursing Module 16Document70 pagesMedical Surgical Nursing Module 16weissNo ratings yet
- Medical Surgical Nursing Module 15Document73 pagesMedical Surgical Nursing Module 15weissNo ratings yet
- Hand Out For Module 1.5Document17 pagesHand Out For Module 1.5weissNo ratings yet
- Hand-out-For-Module-1.3 or Attire, Surgical Hand Scrubbing, Gowning, Closed Gloving, and InstrumentationDocument26 pagesHand-out-For-Module-1.3 or Attire, Surgical Hand Scrubbing, Gowning, Closed Gloving, and Instrumentationweiss100% (1)
- Hand-out-For-Module-1.4 Pre, Intra, and Post Op Patient CareDocument24 pagesHand-out-For-Module-1.4 Pre, Intra, and Post Op Patient CareweissNo ratings yet
- Module 6A - Phases of Drug Action - Pharmacokinetic-3Document11 pagesModule 6A - Phases of Drug Action - Pharmacokinetic-3weissNo ratings yet
- m1.2 Medsurg Pain and SurgerDocument6 pagesm1.2 Medsurg Pain and SurgerweissNo ratings yet
- Module 14 - Drugs-affecting-the-Respiratory-System-3Document48 pagesModule 14 - Drugs-affecting-the-Respiratory-System-3weissNo ratings yet
- Msn-Pain - SurgeryDocument45 pagesMsn-Pain - SurgeryweissNo ratings yet
- Nur 1210 Skills Module #1 Assessment of NewbornDocument19 pagesNur 1210 Skills Module #1 Assessment of NewbornweissNo ratings yet
- Module 8 NCP and PharmaDocument28 pagesModule 8 NCP and PharmaweissNo ratings yet
- Module 8B - Antimicrobials-3Document39 pagesModule 8B - Antimicrobials-3weissNo ratings yet
- Nur 1210 Skills Module #2 Iv TherapyDocument9 pagesNur 1210 Skills Module #2 Iv TherapyweissNo ratings yet
- Module 2 Drug Names, Forms, and Route of Drug Administration-1Document1 pageModule 2 Drug Names, Forms, and Route of Drug Administration-1weissNo ratings yet
- Module 8 - Case Analysis GuidelinesDocument1 pageModule 8 - Case Analysis GuidelinesweissNo ratings yet
- 14.5 - Fa 8 PharmacologyDocument9 pages14.5 - Fa 8 PharmacologyweissNo ratings yet
- Nur 1210 Pedia Module #2 Alterations in OxygenationsDocument16 pagesNur 1210 Pedia Module #2 Alterations in OxygenationsweissNo ratings yet
- 11 Lung PathologyDocument7 pages11 Lung PathologycarlgangcaNo ratings yet
- Acute Respiratory Distress SyndromeDocument14 pagesAcute Respiratory Distress SyndromeAila BarbaNo ratings yet
- Nbme 16 AnsDocument17 pagesNbme 16 Ansnithin shenoi0% (1)
- Pre TestDocument4 pagesPre TestEnzoNo ratings yet
- AtherosclerosisDocument7 pagesAtherosclerosisAna MarieNo ratings yet
- AECOPD GuidelineDocument8 pagesAECOPD GuidelineRonlie RonneyNo ratings yet
- Antibiotic Guideline BIRDEM 2021.pdf Version 1Document92 pagesAntibiotic Guideline BIRDEM 2021.pdf Version 1Imran Khan100% (6)
- DRUG STUDY Bronchitis CorsigaDocument8 pagesDRUG STUDY Bronchitis CorsigaKasandra Dawn Moquia BerisoNo ratings yet
- PLAB Recall 2019-2020Document247 pagesPLAB Recall 2019-2020Shahriar Ahmed Sujoy100% (1)
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- DOH Annual CalendarDocument6 pagesDOH Annual Calendarclarisse_1124No ratings yet
- Pediatric Nursing QuestionsDocument8 pagesPediatric Nursing QuestionsLouie A. Gallego50% (2)
- 8 InfectiousDocument113 pages8 InfectiousLeng IlyNo ratings yet
- USMLE Flashcards: Microbiology and Immunology - Side by SideDocument196 pagesUSMLE Flashcards: Microbiology and Immunology - Side by SideMedSchoolStuff0% (1)
- Pneumonia PathoDocument38 pagesPneumonia PathoIvan Michael IcaoNo ratings yet
- IMCI Flip ChartDocument30 pagesIMCI Flip ChartChrizelle Esperanzate Florentino50% (2)
- A Case of Achalasia Causing Aspiration PneumoniaDocument5 pagesA Case of Achalasia Causing Aspiration PneumoniafannyNo ratings yet
- G.R. No. 187474: Government Service Insurance System V. Marilou AlcarazDocument2 pagesG.R. No. 187474: Government Service Insurance System V. Marilou AlcarazRuss TuazonNo ratings yet
- Community Health Nursing Handout PDFDocument27 pagesCommunity Health Nursing Handout PDFEarl Cordero100% (1)
- National ExamDocument55 pagesNational Examabel100% (1)
- Asthma Bronchiolitis P Nemo NiaDocument64 pagesAsthma Bronchiolitis P Nemo NiainyesuaNo ratings yet
- Symptoms of PneumoniaDocument4 pagesSymptoms of PneumoniaAndeariesa DarmansiusNo ratings yet
- Pediatrics, Geriatrics and Clinical MicrobiologyDocument15 pagesPediatrics, Geriatrics and Clinical MicrobiologySelvakumardxbNo ratings yet
- The Value of Chest Ultrasonography Applications in The Respiratory ICUDocument6 pagesThe Value of Chest Ultrasonography Applications in The Respiratory ICUHeru SigitNo ratings yet
- Aspiration Pneumonitis and PneumoniaDocument2 pagesAspiration Pneumonitis and PneumoniaAza Patullah ZaiNo ratings yet
- Chronic Airspace DiseasesDocument31 pagesChronic Airspace DiseasesAnkita ShahNo ratings yet
- Safari - 12 May 2020 10.04Document1 pageSafari - 12 May 2020 10.04tenun witaNo ratings yet
- History TakingDocument180 pagesHistory TakingDers100% (1)
- 337d PDFDocument8 pages337d PDFEka MeylianaNo ratings yet
- Resistencia ClorhexidinaDocument30 pagesResistencia ClorhexidinaVlady78No ratings yet