You might also like
- Medical Surgical Nursing Module 17Document31 pagesMedical Surgical Nursing Module 17weissNo ratings yet
- Medical Surgical Nursing Module 16Document70 pagesMedical Surgical Nursing Module 16weissNo ratings yet
- W1. Pendekatan Sesak Pada AnakDocument32 pagesW1. Pendekatan Sesak Pada Anaksekrekomdik RSPDNo ratings yet
- Shortness of Breath: ER Perspective Shaesta TabassumDocument46 pagesShortness of Breath: ER Perspective Shaesta TabassumAjay DherwaniNo ratings yet
- Medsurg LessonDocument39 pagesMedsurg LessonLara Marie MACALINTALNo ratings yet
- 3.pulmonary Alterations - Part 2Document37 pages3.pulmonary Alterations - Part 2Rawan AlotaibiNo ratings yet
- Dyspnea - DR AllenDocument50 pagesDyspnea - DR AllenalmiraerickaiNo ratings yet
- Oxygenation ProblemsDocument4 pagesOxygenation ProblemsAlec Xavier MirandaNo ratings yet
- Oxygenation Lesson 3Document78 pagesOxygenation Lesson 3Yjah Cheimira ASEBONo ratings yet
- Kegawatan Napas Pada AnakDocument43 pagesKegawatan Napas Pada AnakRaelna SahaarNo ratings yet
- Assessment of Respiratory System: Submitted by Pankaj Singh Rana Nurse Practitioner in Critical Care, SrhuDocument80 pagesAssessment of Respiratory System: Submitted by Pankaj Singh Rana Nurse Practitioner in Critical Care, SrhuMary Christine Estrada CabactulanNo ratings yet
- ASSESSMENT WITH RESPIRATORY DISORDERS and DiagnosticsDocument11 pagesASSESSMENT WITH RESPIRATORY DISORDERS and DiagnosticsErika Mae Sta. MariaNo ratings yet
- Medical TerminologyDocument3 pagesMedical TerminologyLeovelle de GuiaNo ratings yet
- Eko Budiono Pulmonology/Internal Medicine Departement, Faculty of Medicine, Gadjah Mada University Dr. Sardjito Hospital, YogyakartaDocument43 pagesEko Budiono Pulmonology/Internal Medicine Departement, Faculty of Medicine, Gadjah Mada University Dr. Sardjito Hospital, YogyakartaJoshua HendersonNo ratings yet
- BreathlessnessDocument29 pagesBreathlessnessRajveerNo ratings yet
- Assessment Pada Covid-19Document60 pagesAssessment Pada Covid-19FISIOTERAPI TRIMITRANo ratings yet
- Nursing Management of Patient With Respiratory ProblemsDocument151 pagesNursing Management of Patient With Respiratory ProblemsAbirajan100% (2)
- Copd NatsDocument47 pagesCopd NatsKristen Nathany MalapitNo ratings yet
- Pneumonia Study GuideDocument5 pagesPneumonia Study GuideMartha Marty BalintNo ratings yet
- Medical Surgical Nursing Module 14Document31 pagesMedical Surgical Nursing Module 14weissNo ratings yet
- Assessment of Thorax Lungs Lecture 2019 2020Document43 pagesAssessment of Thorax Lungs Lecture 2019 2020Dan Floyd FernandezNo ratings yet
- Evaluation of The Patient With Pulmonary DiseaseDocument57 pagesEvaluation of The Patient With Pulmonary DiseaseJr SparkNo ratings yet
- Lungs and ThoraxDocument9 pagesLungs and ThoraxMaria Mika Ella RetizaNo ratings yet
- Block Q IM Orals ReviewerDocument107 pagesBlock Q IM Orals ReviewerCarl Vin PasionNo ratings yet
- Oxygenation Part 1Document86 pagesOxygenation Part 1Shaira Mae Fangon De GuzmanNo ratings yet
- The Respiratory System (Intro)Document75 pagesThe Respiratory System (Intro)Krestel Saligumba PalanogNo ratings yet
- NCM103 - 2016 - Lecture2 - Response To Altered Respiratory FunctionDocument128 pagesNCM103 - 2016 - Lecture2 - Response To Altered Respiratory FunctionrimeoznekNo ratings yet
- Basic Skills For Clients With Oxygenation ProblemsDocument3 pagesBasic Skills For Clients With Oxygenation ProblemsAlec Xavier MirandaNo ratings yet
- Mengenal Kegawatan Pada AnakDocument45 pagesMengenal Kegawatan Pada Anakyasmin100% (1)
- Obstructive Sleep Apnoea SyndromeDocument72 pagesObstructive Sleep Apnoea SyndromeArjun SainiNo ratings yet
- Bronchitis: Kelompok IDocument14 pagesBronchitis: Kelompok ILinda Permata Sari100% (1)
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocument7 pagesNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNo ratings yet
- Week 5 Respiratory System SB Final-محولDocument121 pagesWeek 5 Respiratory System SB Final-محولWalaa 1998No ratings yet
- Chronic Bronchitis, Emphysema, Bronciectasis - PPT.Document51 pagesChronic Bronchitis, Emphysema, Bronciectasis - PPT.Jumar ValdezNo ratings yet
- Asthma DX Article 1Document16 pagesAsthma DX Article 1Pat Caz SarNo ratings yet
- ARDSDocument53 pagesARDSrani asfiyaNo ratings yet
- Dr. Taufiq - Airway - TaufiqabdullahDocument50 pagesDr. Taufiq - Airway - TaufiqabdullahAziz AzizahNo ratings yet
- Dyspnea in Children - Wahyuni IndawatiDocument20 pagesDyspnea in Children - Wahyuni IndawatiTarmidi MidziNo ratings yet
- PBL 2nd Sem Scenario 1Document164 pagesPBL 2nd Sem Scenario 1stephaniecaronan15No ratings yet
- Chapter 27Document6 pagesChapter 27monster40lbsNo ratings yet
- Oxygenation MethodsDocument9 pagesOxygenation MethodswowsamanthaNo ratings yet
- Medical Surgical (MS) Rle Pulmonary/ Lung AssessmentDocument8 pagesMedical Surgical (MS) Rle Pulmonary/ Lung AssessmentYman Gio BumanglagNo ratings yet
- Cardio AssessmentDocument62 pagesCardio AssessmentPine DrakeNo ratings yet
- Lesson II Gas Exchange DisordersDocument126 pagesLesson II Gas Exchange DisordersYjah Cheimira ASEBONo ratings yet
- Anatomical Findings Upper and Lower AirwaysDocument84 pagesAnatomical Findings Upper and Lower AirwaysIndira HernandezNo ratings yet
- RESPIRATORY SYSTEM Nclex Iloilo 4Document27 pagesRESPIRATORY SYSTEM Nclex Iloilo 4Barangay Centro SurNo ratings yet
- Pleural Conditions, ARF, ARDSDocument48 pagesPleural Conditions, ARF, ARDSJumar ValdezNo ratings yet
- Shortness of Breath NotesDocument7 pagesShortness of Breath NotesChananNo ratings yet
- Neonatal X Ray PDFDocument144 pagesNeonatal X Ray PDFnicuanumybabyNo ratings yet
- Oxygenation Lesson1-2Document85 pagesOxygenation Lesson1-2Yjah Cheimira ASEBONo ratings yet
- 02 Respi EmergenciesDocument133 pages02 Respi EmergenciesLizeil VelardeNo ratings yet
- Funda Notes Nca MidtermDocument9 pagesFunda Notes Nca MidtermAICEL A. ABILNo ratings yet
- Medicine: CardiorespiratoryDocument56 pagesMedicine: CardiorespiratoryWalaa abo foolNo ratings yet
- Nursing Care of Children With Alterations in HealthDocument44 pagesNursing Care of Children With Alterations in HealthAmy Del Carmen50% (2)
- Asthma MeidaDocument17 pagesAsthma MeidaDaffa AlfaiqNo ratings yet
- Dyspnea: CausesDocument7 pagesDyspnea: CausesGetom NgukirNo ratings yet
- Pulmunology FADocument39 pagesPulmunology FAJaankiNo ratings yet
- resp د. وفاءDocument22 pagesresp د. وفاءProf. Wafaa Mohammed Al-AttarNo ratings yet
- Nasal ObstructionDocument25 pagesNasal ObstructionAnshu kumariNo ratings yet
- Medical Surgical Nursing Module 8Document9 pagesMedical Surgical Nursing Module 8weissNo ratings yet
- Medical Surgical Nursing Module 7Document18 pagesMedical Surgical Nursing Module 7weissNo ratings yet
- Medical Surgical Nursing Module 10Document34 pagesMedical Surgical Nursing Module 10weissNo ratings yet
- Medical Surgical Nursing Module 19Document4 pagesMedical Surgical Nursing Module 19weissNo ratings yet
- Medical Surgical Nursing Module 9Document8 pagesMedical Surgical Nursing Module 9weissNo ratings yet
- Medical Surgical Nursing Module 4Document17 pagesMedical Surgical Nursing Module 4weissNo ratings yet
- Medical Surgical Nursing Module 6Document8 pagesMedical Surgical Nursing Module 6weissNo ratings yet
- Cardio TransDocument7 pagesCardio TransweissNo ratings yet
- Medical Surgical Nursing Module 11Document26 pagesMedical Surgical Nursing Module 11weissNo ratings yet
- Medical Surgical Nursing Module 12Document45 pagesMedical Surgical Nursing Module 12weissNo ratings yet
- Pain and Surgery TransDocument44 pagesPain and Surgery TransweissNo ratings yet
- Medical Surgical Nursing Module 14Document31 pagesMedical Surgical Nursing Module 14weissNo ratings yet
- Hand Out For Module 1.5Document17 pagesHand Out For Module 1.5weissNo ratings yet
- Hand-out-For-Module-1.3 or Attire, Surgical Hand Scrubbing, Gowning, Closed Gloving, and InstrumentationDocument26 pagesHand-out-For-Module-1.3 or Attire, Surgical Hand Scrubbing, Gowning, Closed Gloving, and Instrumentationweiss100% (1)
- Hand-out-For-Module-1.4 Pre, Intra, and Post Op Patient CareDocument24 pagesHand-out-For-Module-1.4 Pre, Intra, and Post Op Patient CareweissNo ratings yet
- Ms Pain and Surgery ModulesDocument30 pagesMs Pain and Surgery ModulesweissNo ratings yet
- Module 6A - Phases of Drug Action - Pharmacokinetic-3Document11 pagesModule 6A - Phases of Drug Action - Pharmacokinetic-3weissNo ratings yet
- m1.2 Medsurg Pain and SurgerDocument6 pagesm1.2 Medsurg Pain and SurgerweissNo ratings yet
- Module 14 - Drugs-affecting-the-Respiratory-System-3Document48 pagesModule 14 - Drugs-affecting-the-Respiratory-System-3weissNo ratings yet
- Msn-Pain - SurgeryDocument45 pagesMsn-Pain - SurgeryweissNo ratings yet
- Nur 1210 Skills Module #1 Assessment of NewbornDocument19 pagesNur 1210 Skills Module #1 Assessment of NewbornweissNo ratings yet
- Module 8 NCP and PharmaDocument28 pagesModule 8 NCP and PharmaweissNo ratings yet
- Module 8B - Antimicrobials-3Document39 pagesModule 8B - Antimicrobials-3weissNo ratings yet
- Nur 1210 Skills Module #2 Iv TherapyDocument9 pagesNur 1210 Skills Module #2 Iv TherapyweissNo ratings yet
- Module 2 Drug Names, Forms, and Route of Drug Administration-1Document1 pageModule 2 Drug Names, Forms, and Route of Drug Administration-1weissNo ratings yet
- Module 8 - Case Analysis GuidelinesDocument1 pageModule 8 - Case Analysis GuidelinesweissNo ratings yet
- 14.5 - Fa 8 PharmacologyDocument9 pages14.5 - Fa 8 PharmacologyweissNo ratings yet
- Nur 1210 Pedia Module #2 Alterations in OxygenationsDocument16 pagesNur 1210 Pedia Module #2 Alterations in OxygenationsweissNo ratings yet
- COMPLICATII TARDIVE DUPA INJECTAREA DE ACID HIALURONIC IN SCOP ESTETIC SI MANAGEMENTUL LOR Ro 399Document21 pagesCOMPLICATII TARDIVE DUPA INJECTAREA DE ACID HIALURONIC IN SCOP ESTETIC SI MANAGEMENTUL LOR Ro 399tzupel4No ratings yet
- @MBS MedicalBooksStore 2020 CompressionDocument46 pages@MBS MedicalBooksStore 2020 CompressionTaufikNo ratings yet
- TramadolDocument2 pagesTramadolJordanne EtisNo ratings yet
- Foundations of Operative Surgery An Introduction To Surgical TechniquesDocument165 pagesFoundations of Operative Surgery An Introduction To Surgical TechniquesTeodora-Valeria TolanNo ratings yet
- Cholera (5 5)Document1 pageCholera (5 5)Celestial, Maybelle MarieNo ratings yet
- Emergency Anaesthetic Management To Extensive Thoracic Trauma-Hossam AtefDocument60 pagesEmergency Anaesthetic Management To Extensive Thoracic Trauma-Hossam AtefHossam atefNo ratings yet
- PMLS Lesson 5Document7 pagesPMLS Lesson 5Althea EspirituNo ratings yet
- Haematology Paper 1 - Past PapersDocument9 pagesHaematology Paper 1 - Past Papersmma1976100% (1)
- Case Study of Most Common Communicable DiseasesDocument13 pagesCase Study of Most Common Communicable DiseasesnesjynNo ratings yet
- Parasitology: - IntroductionDocument62 pagesParasitology: - IntroductionHana AliNo ratings yet
- National NORCET Test-9Document106 pagesNational NORCET Test-9SHIVANIINo ratings yet
- Secukinumab: First Global ApprovalDocument10 pagesSecukinumab: First Global ApprovalAri KurniawanNo ratings yet
- Respiratory FailureDocument4 pagesRespiratory FailureMeey Mee100% (1)
- Sports DrinksDocument2 pagesSports DrinksMustofaNo ratings yet
- An Unconscious Patient With A DNR TattooDocument2 pagesAn Unconscious Patient With A DNR TattoonadaNo ratings yet
- Pe 11 Quarter 3 Lesson 1Document17 pagesPe 11 Quarter 3 Lesson 1Donah Kate AlbaNo ratings yet
- DctsDocument30 pagesDctsInuyashayahoo100% (1)
- Defense Medical Epidemiology Database Report - Jan 26, 2022Document41 pagesDefense Medical Epidemiology Database Report - Jan 26, 2022adan_infowars100% (2)
- Pseudofollicular BabaeDocument13 pagesPseudofollicular BabaeOlamide EstherNo ratings yet
- An Approach To A Floppy InfantDocument33 pagesAn Approach To A Floppy InfantayunisallehNo ratings yet
- WEVM Chapter 1Document22 pagesWEVM Chapter 1Manoj KarkiNo ratings yet
- Vitamin and Mineral Supplementation During PregnanDocument4 pagesVitamin and Mineral Supplementation During PregnanEvi RachmawatiNo ratings yet
- +++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchDocument5 pages+++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchEnes ÇakmakNo ratings yet
- Grand Case Presentation InformationDocument7 pagesGrand Case Presentation InformationCristina L. JaysonNo ratings yet
- SupradynDocument5 pagesSupradynashrayagrawalNo ratings yet
- Mental IllnessDocument3 pagesMental IllnessKate EvangelistaNo ratings yet
- Probiotic Supplementation For Prevention of Atopic Dermatitis in Infants and Children: A Systematic Review and Meta AnalysisDocument11 pagesProbiotic Supplementation For Prevention of Atopic Dermatitis in Infants and Children: A Systematic Review and Meta AnalysisGrace Malinda LimopranotoNo ratings yet
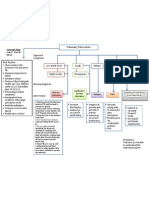
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- PMLSDocument9 pagesPMLSChan ChanNo ratings yet
- The GINA 2019 Asthma Treatment Strategy For Adults and Adolescents 12... Download Scientific DiagramDocument1 pageThe GINA 2019 Asthma Treatment Strategy For Adults and Adolescents 12... Download Scientific DiagramFatih AryaNo ratings yet