You might also like
- Induction of Fuzzy Rules and Membership Functions From Training Examples'Document15 pagesInduction of Fuzzy Rules and Membership Functions From Training Examples'حسين شنيقيNo ratings yet
- Research Resiliency Through Lean LabsDocument6 pagesResearch Resiliency Through Lean LabswiredfrombackNo ratings yet
- Ten Key Considerations For The Successful Implementation and Adoption of Large-Scale Health Information TechnologyDocument5 pagesTen Key Considerations For The Successful Implementation and Adoption of Large-Scale Health Information TechnologyYoona LimNo ratings yet
- Generating Uncertain Fuzzy Logic Rules From SurveysDocument6 pagesGenerating Uncertain Fuzzy Logic Rules From SurveysÄkshãy SaçhånNo ratings yet
- 1 s2.0 S2212827112002119 MainDocument6 pages1 s2.0 S2212827112002119 Mainamin farajNo ratings yet
- Skills and Competencies For Resilience in Manufacturing Systems: A Systematic Literature ReviewDocument10 pagesSkills and Competencies For Resilience in Manufacturing Systems: A Systematic Literature ReviewIJAERS JOURNALNo ratings yet
- Considering The Business System 'S Complexity With A Network ApproachDocument17 pagesConsidering The Business System 'S Complexity With A Network Approachplayjake18No ratings yet
- Evaluating organizational resilience in QuebecDocument7 pagesEvaluating organizational resilience in QuebecakhilNo ratings yet
- A Generic Framework For Prognostics of Complex SystemsAerospaceDocument27 pagesA Generic Framework For Prognostics of Complex SystemsAerospaceClovis NetoNo ratings yet
- Tremblay Et Al 2010 Effluent Decontamination Systems Addressing The Challenges of Planning Designing Testing andDocument11 pagesTremblay Et Al 2010 Effluent Decontamination Systems Addressing The Challenges of Planning Designing Testing andAntonio Osante LeyvaNo ratings yet
- The RESOLVE PCOM Implementation StrategyDocument9 pagesThe RESOLVE PCOM Implementation StrategycharmyshkuNo ratings yet
- A Belief Rulebased Environmental Responsibility Assessment For Small and Mediumsized EnterpriseDocument7 pagesA Belief Rulebased Environmental Responsibility Assessment For Small and Mediumsized Enterprisenia divaNo ratings yet
- Puter System ValidationDocument65 pagesPuter System ValidationAzza ShoukrNo ratings yet
- Literature Review of Work Environment, Training and Health Safety Factors Analysis in Increasing ProductivityDocument4 pagesLiterature Review of Work Environment, Training and Health Safety Factors Analysis in Increasing ProductivityPipe GonzalezNo ratings yet
- Cues and Cue-Based Processing: Implications For System SafetyDocument7 pagesCues and Cue-Based Processing: Implications For System SafetyJavier Alejandro RodriguezNo ratings yet
- 5bbb PDFDocument6 pages5bbb PDFRick RanteNo ratings yet
- Managing The Information System Life Cycle in Construction and ManufacturingDocument5 pagesManaging The Information System Life Cycle in Construction and ManufacturingShankar CNo ratings yet
- System Performance Prognostic: Context, Issues and RequirementsDocument7 pagesSystem Performance Prognostic: Context, Issues and Requirementsmy_scribd_2010No ratings yet
- TMP 2 DEEDocument13 pagesTMP 2 DEEFrontiersNo ratings yet
- CFIR Based On User FeedbackDocument16 pagesCFIR Based On User Feedbackdivya gosainNo ratings yet
- Hofstede1978e Poverty of Management Control PhilosophyDocument13 pagesHofstede1978e Poverty of Management Control PhilosophyВладимир ДружининNo ratings yet
- 10 1016@j Jmsy 2020 07 008Document19 pages10 1016@j Jmsy 2020 07 008Doua AhmadNo ratings yet
- Autonomic ComputingDocument11 pagesAutonomic ComputingklsjjNo ratings yet
- Towards Sustainable Hydrogen Production. an Integrated Approach for Energy Sector. Journal of Cleaner Prod. 2024Document18 pagesTowards Sustainable Hydrogen Production. an Integrated Approach for Energy Sector. Journal of Cleaner Prod. 2024alyson rodriguesNo ratings yet
- Quantifying The Effectiveness of Alarm Management Systems Through Human Factors StudeisDocument12 pagesQuantifying The Effectiveness of Alarm Management Systems Through Human Factors StudeisBhavaNo ratings yet
- Machine Learning For Predictive Maintenance: A Multiple Classifier ApproachDocument9 pagesMachine Learning For Predictive Maintenance: A Multiple Classifier ApproachBruno RibeiroNo ratings yet
- Safety and Health at Work: Leif Jarle GressgårdDocument7 pagesSafety and Health at Work: Leif Jarle GressgårdRayanNo ratings yet
- s13012-022-01245-0Document16 pagess13012-022-01245-0Bung HerryNo ratings yet
- Aircraft System Safety: Assessments for Initial Airworthiness CertificationFrom EverandAircraft System Safety: Assessments for Initial Airworthiness CertificationNo ratings yet
- Field Study, Field Experiment, and Macroergonomic Analysis of Structure (MAS) MethodsDocument5 pagesField Study, Field Experiment, and Macroergonomic Analysis of Structure (MAS) MethodsZahra WiniadestaNo ratings yet
- A Systemic Methodology For Risk Management in Healthcare SectorDocument14 pagesA Systemic Methodology For Risk Management in Healthcare SectorLydia WanjikuNo ratings yet
- Patterns For Self-Adaptation in Cyber-Physical SystemsDocument38 pagesPatterns For Self-Adaptation in Cyber-Physical SystemsHargyo NugrohoNo ratings yet
- Commitment Issues in Delegation ProcessDocument13 pagesCommitment Issues in Delegation ProcessAli SameerNo ratings yet
- Educating To Achieve Healthy Open Source Ecosystems: Simone Da Silva Amorim John D. McgregorDocument6 pagesEducating To Achieve Healthy Open Source Ecosystems: Simone Da Silva Amorim John D. McgregorIvanilse Calderon RibeiroNo ratings yet
- Using Soft Systems Methodology As A Systemic Approach To Safety Performance EvaluationDocument9 pagesUsing Soft Systems Methodology As A Systemic Approach To Safety Performance EvaluationAhmad FajriNo ratings yet
- The Resilient Potential Behaviours in An Internal Medicine DepartmentDocument18 pagesThe Resilient Potential Behaviours in An Internal Medicine DepartmentDaniel fabian Sánchez henaoNo ratings yet
- Formal Verification of Fraud Resilience in A Crowdsourci - 2023 - Computers - SeDocument26 pagesFormal Verification of Fraud Resilience in A Crowdsourci - 2023 - Computers - SeAkashah ArshadNo ratings yet
- MosGabriel Essay OverviewforIIS PDFDocument24 pagesMosGabriel Essay OverviewforIIS PDFVasile SentimentNo ratings yet
- Automated Norm Synthesis in An Agent-Based PlanninDocument9 pagesAutomated Norm Synthesis in An Agent-Based PlanninJhonatan AlvesNo ratings yet
- (1998) Enabling The Implementation of Evidence-Based PracticeDocument10 pages(1998) Enabling The Implementation of Evidence-Based PracticecharmyshkuNo ratings yet
- Model-Driven Approach for Privacy ManagementDocument9 pagesModel-Driven Approach for Privacy ManagementHernan AvilaNo ratings yet
- An Approach To Modular and Testable Security Models of Real-World Health-Care ApplicationsDocument10 pagesAn Approach To Modular and Testable Security Models of Real-World Health-Care ApplicationsLola MakeupNo ratings yet
- TOC Implementation in A Medium-Scale Manufacturing System With Diverse Product RootingDocument18 pagesTOC Implementation in A Medium-Scale Manufacturing System With Diverse Product RootingNurlanNo ratings yet
- Design of Systems For Productivity and Well BeingDocument7 pagesDesign of Systems For Productivity and Well Beingcindy briceño garciaNo ratings yet
- Group Policy and Group Policy ObjectsDocument5 pagesGroup Policy and Group Policy ObjectsEphraimNo ratings yet
- Machine Learning For Predictive Maintenance A Multiple Classifier ApproachDocument10 pagesMachine Learning For Predictive Maintenance A Multiple Classifier ApproachWilliam OrtizNo ratings yet
- Integration Conceptual Framework of Quality Manage PDFDocument7 pagesIntegration Conceptual Framework of Quality Manage PDFaji hafid laksanaNo ratings yet
- Barna 1Document27 pagesBarna 1Daniel Hernández ViteNo ratings yet
- ISC Process Safety Competency GuidanceDocument28 pagesISC Process Safety Competency GuidancekokykarkarNo ratings yet
- Bbs Preventive ToolsDocument6 pagesBbs Preventive ToolsEmmanuelNo ratings yet
- UntitledDocument49 pagesUntitledCesar FasanandoNo ratings yet
- 2012 Tinga MBFA BookDocument78 pages2012 Tinga MBFA BookRushil RamroepNo ratings yet
- Jurnal MantekDocument14 pagesJurnal MantekFarhan AzhariNo ratings yet
- Qual Health Care-1998-Kitson-149-58Document11 pagesQual Health Care-1998-Kitson-149-58AFelipe CortésNo ratings yet
- Safety in The OilfieldDocument5 pagesSafety in The OilfieldNasser YahaNo ratings yet
- Стаття - 03 - 2021 - tsopa - elaboration of an Integral System of Company ManagementDocument6 pagesСтаття - 03 - 2021 - tsopa - elaboration of an Integral System of Company Managementpalmash1961No ratings yet
- How Do Software Architectural Practices Impact Onopen Source Ecosystem Health?COMPLETODocument8 pagesHow Do Software Architectural Practices Impact Onopen Source Ecosystem Health?COMPLETOChristina von Flach Garcia ChavezNo ratings yet
- Exploration of Success Factors of Information System: KeywordsDocument10 pagesExploration of Success Factors of Information System: KeywordsWendelynn Giannina AngNo ratings yet
- Bearings Accelerated Degradation PlatformDocument8 pagesBearings Accelerated Degradation PlatformEQ GMNo ratings yet
- Safety Management: An IntroductionDocument3 pagesSafety Management: An IntroductionNailesh MahetaNo ratings yet
- Why You Need To Be A Systems Thinker in Health CareDocument3 pagesWhy You Need To Be A Systems Thinker in Health CareBhavik PrajapatiNo ratings yet
- 1020 3397 2020 2608 872 876 EngDocument5 pages1020 3397 2020 2608 872 876 EngBhavik PrajapatiNo ratings yet
- Systems Thinkingfor HSS2009Document113 pagesSystems Thinkingfor HSS2009Bhavik PrajapatiNo ratings yet
- Systems Research and Behavioral Science - 2016 - Kapp - A Conceptual Framework For A Systems Thinking Approach To USDocument13 pagesSystems Research and Behavioral Science - 2016 - Kapp - A Conceptual Framework For A Systems Thinking Approach To USBhavik PrajapatiNo ratings yet
- SpathKelly Ch3-B87c108eDocument16 pagesSpathKelly Ch3-B87c108eBhavik PrajapatiNo ratings yet
- Systems Thinking Theory and Practice The Case of VW Corporate CrisisDocument18 pagesSystems Thinking Theory and Practice The Case of VW Corporate CrisisBhavik PrajapatiNo ratings yet
- Systems 08 00014 v2Document19 pagesSystems 08 00014 v2Bhavik PrajapatiNo ratings yet
- System Thinking Rich Picture CATWOE and Root Definition ReportDocument9 pagesSystem Thinking Rich Picture CATWOE and Root Definition ReportBhavik PrajapatiNo ratings yet
- Cocacola Case Study Systems ThinkingDocument6 pagesCocacola Case Study Systems ThinkingBhavik Prajapati0% (1)
- 6984-Article Text-31533-1-10-20200630Document4 pages6984-Article Text-31533-1-10-20200630Bhavik PrajapatiNo ratings yet
- HospitalDocument17 pagesHospitalBhavik PrajapatiNo ratings yet
- Mastering Your Day as a Product ManagerDocument38 pagesMastering Your Day as a Product ManagerBhavik PrajapatiNo ratings yet
- White Paper Product Management As A Leadership RoleDocument16 pagesWhite Paper Product Management As A Leadership RoleBhavik PrajapatiNo ratings yet
- Management - Vol 5 - Issue 1 - Article - 5Document5 pagesManagement - Vol 5 - Issue 1 - Article - 5Bhavik PrajapatiNo ratings yet
- Introduction to the Key Concepts of Product ManagementDocument71 pagesIntroduction to the Key Concepts of Product ManagementBhavik PrajapatiNo ratings yet
- Sports Injury Assessment PDFDocument43 pagesSports Injury Assessment PDFPatricia Andrea Acevedo ArancibiaNo ratings yet
- Reversible Dementia and DeliriumDocument65 pagesReversible Dementia and Deliriummpm8471No ratings yet
- Lindlahr's BookDocument537 pagesLindlahr's BookRajendra Nath100% (1)
- Effort Changes of Lower Complete Denture Material Caused by ReliningDocument4 pagesEffort Changes of Lower Complete Denture Material Caused by ReliningChusnul ChotimahNo ratings yet
- Prevalence of Dysmenorrhea Among Medical StudentsDocument3 pagesPrevalence of Dysmenorrhea Among Medical StudentsNovia ambarwatiNo ratings yet
- Abbreviations and SymbolsDocument73 pagesAbbreviations and Symbolsruzana1396No ratings yet
- ECG BasicsDocument34 pagesECG BasicsBeaCeeNo ratings yet
- International Ayurvedic Medical Journal: CharacterizedDocument4 pagesInternational Ayurvedic Medical Journal: CharacterizedDrHassan Ahmed ShaikhNo ratings yet
- Nose-Report (Part) The Morinaga Milk Arsenic Poisoning Incident 50 Years On A Report Outlining The Implementation Status of The Victims Relief ProjectDocument17 pagesNose-Report (Part) The Morinaga Milk Arsenic Poisoning Incident 50 Years On A Report Outlining The Implementation Status of The Victims Relief ProjectAmanda NguyenNo ratings yet
- Cymbalta (Duloxetine HCL) Patient Information - Side Effects and Drug Images at RxlistDocument7 pagesCymbalta (Duloxetine HCL) Patient Information - Side Effects and Drug Images at Rxlisteiad-mahmoudNo ratings yet
- RIG WASH For BargesDocument5 pagesRIG WASH For BargesUnokhogie EmmanuelNo ratings yet
- Obstetrics / Gynaecological Infections: Indications First Line AlternateDocument2 pagesObstetrics / Gynaecological Infections: Indications First Line AlternateAli ShanNo ratings yet
- Text Atlas of Podiatric DermatologyDocument163 pagesText Atlas of Podiatric Dermatologyanupam75path100% (8)
- Dr. Vera CruzDocument9 pagesDr. Vera CruzPatrick John BatolNo ratings yet
- Ethical Issues in HelthcareDocument12 pagesEthical Issues in HelthcareTajirul HaqueNo ratings yet
- Art Deco AssignmentDocument20 pagesArt Deco AssignmentAmerNo ratings yet
- Allen's Keynotes Materia MedicaDocument138 pagesAllen's Keynotes Materia Medicasunnyjamiel100% (8)
- National List of Essential Medicines - Nepal, Fourth Revision, 2009Document40 pagesNational List of Essential Medicines - Nepal, Fourth Revision, 2009Suresh DhunganaNo ratings yet
- Technical Guide For The Elaboration of Monographs EDQMDocument72 pagesTechnical Guide For The Elaboration of Monographs EDQMppiccoliniNo ratings yet
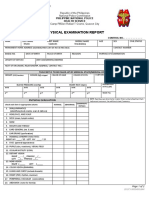
- PNP HS MS Form Physical ExamDocument2 pagesPNP HS MS Form Physical Examlara michelleNo ratings yet
- Abs Bench 500 Manual 3esDocument15 pagesAbs Bench 500 Manual 3esmaremotusNo ratings yet
- SinusitisDocument19 pagesSinusitisinnyNo ratings yet
- Aki & CKDDocument61 pagesAki & CKDChengzhi KhorNo ratings yet
- The US Pharmacy Benefit Management (PBM) Industry Report: 2013 Edition - New Report by Koncept AnalyticsDocument10 pagesThe US Pharmacy Benefit Management (PBM) Industry Report: 2013 Edition - New Report by Koncept AnalyticsKoncept AnalyticsNo ratings yet
- UAE HospitalsDocument20 pagesUAE Hospitalsswati_progNo ratings yet
- Role of Noni in Kidney Diseases: Pre-Renal CRFDocument9 pagesRole of Noni in Kidney Diseases: Pre-Renal CRFputhrimathiNo ratings yet
- Medicinal Chemistry: AnalgesicsDocument6 pagesMedicinal Chemistry: AnalgesicsAlishba MushtaqNo ratings yet
- Jjpaf ApplicationDocument6 pagesJjpaf ApplicationCharles LeeNo ratings yet
- Cranial Nerves V, Vii, Viii, Ix, X, Xi, Xii: DR Nan Ommar FMHS, UnimasDocument32 pagesCranial Nerves V, Vii, Viii, Ix, X, Xi, Xii: DR Nan Ommar FMHS, UnimasMerriNo ratings yet
- Poor Water QualityDocument18 pagesPoor Water QualityjeysamNo ratings yet