You might also like
- Berklee Intro Music Therapy PDFDocument17 pagesBerklee Intro Music Therapy PDFTheodore VaillantNo ratings yet
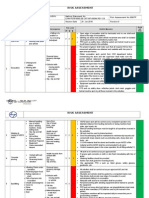
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Hazards of Nitrogen AsphyxiationDocument10 pagesHazards of Nitrogen AsphyxiationRaja Senthil NathanNo ratings yet
- Spina BifidaDocument29 pagesSpina Bifidaann dimcoNo ratings yet
- Spina BifidaDocument11 pagesSpina BifidaheiyuNo ratings yet
- DocumentDocument12 pagesDocumentJon Saiman0% (1)
- Errata 1Document9 pagesErrata 1Doc AhsanNo ratings yet
- Tung DocumentreviewDocument8 pagesTung DocumentreviewRodrigo Bittencourt100% (3)
- Lec 4 Principles of Health Financing PDFDocument6 pagesLec 4 Principles of Health Financing PDFRem Alfelor100% (1)
- Study To Access The Knowledge Under Five Mothers Regarding Prevention of Malnutrition in Ankuli Berhampur Ganjam OdishaDocument59 pagesStudy To Access The Knowledge Under Five Mothers Regarding Prevention of Malnutrition in Ankuli Berhampur Ganjam OdishaPabhat Kumar100% (2)
- Neural Tube Defects: Dr.M.G.Kartheeka Fellow in Neonatology Cloudnine, OARDocument36 pagesNeural Tube Defects: Dr.M.G.Kartheeka Fellow in Neonatology Cloudnine, OARM G KARTHEEKANo ratings yet
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- Pediatric RehabDocument32 pagesPediatric RehabRainy DaysNo ratings yet
- No. 44. Neural Tube DefectsDocument11 pagesNo. 44. Neural Tube DefectsenriqueNo ratings yet
- DiscursoDocument21 pagesDiscursoLeslye SimbañaNo ratings yet
- Bahan Ajar Iv Spina BifidaDocument7 pagesBahan Ajar Iv Spina Bifidaanon_800290919No ratings yet
- Medscape Spina BifidaDocument25 pagesMedscape Spina Bifidarica dhamayantiNo ratings yet
- Neural Tube Defects: Group 1Document28 pagesNeural Tube Defects: Group 1imneverwrong2492100% (1)
- Spinal DisDocument32 pagesSpinal DisAkmal Niam FirdausiNo ratings yet
- MedBack MyelomeningoceleDocument3 pagesMedBack MyelomeningoceleJulia Rei Eroles IlaganNo ratings yet
- Fetal Surgery Spina BifidaDocument12 pagesFetal Surgery Spina BifidaAvicenna Shafhan ArfiNo ratings yet
- SpinaBifida ManagementDocument4 pagesSpinaBifida ManagementDimple GoyalNo ratings yet
- Spinal DysraphismDocument2 pagesSpinal DysraphismkhadzxNo ratings yet
- Spina Bifida Guide: Types, Causes & Nursing CareDocument5 pagesSpina Bifida Guide: Types, Causes & Nursing CareJulliza Joy PandiNo ratings yet
- MyelodysplasiaDocument12 pagesMyelodysplasiaJhon AlefeNo ratings yet
- Review Article: Spina Bifida: Pathogenesis, Mechanisms, and Genes in Mice and HumansDocument30 pagesReview Article: Spina Bifida: Pathogenesis, Mechanisms, and Genes in Mice and Humansrosandi sabollaNo ratings yet
- Spina Bifida General Dental PracticeDocument5 pagesSpina Bifida General Dental PracticerambuanggieNo ratings yet
- Neural Tube DefectsDocument12 pagesNeural Tube Defectsdaniel_1592No ratings yet
- Myelomeningocele - StatPearls - NCBI BookshelfDocument13 pagesMyelomeningocele - StatPearls - NCBI BookshelfEmmanuel Andrew Dela CruzNo ratings yet
- Neurogenic BladderDocument8 pagesNeurogenic BladderrafendyfendyNo ratings yet
- 2011 32 109 Holly A. Zywicke and Curtis J. Rozzelle: Pediatrics in ReviewDocument10 pages2011 32 109 Holly A. Zywicke and Curtis J. Rozzelle: Pediatrics in ReviewNavine NalechamiNo ratings yet
- Syndromic Craniosynostosis 19pDocument6 pagesSyndromic Craniosynostosis 19pAnna Karolinne NascimentoNo ratings yet
- Neural Tube DefectDocument13 pagesNeural Tube Defectrittika dasNo ratings yet
- Interdisciplinary Neurosurgery: Jimmy Ntimbani, Adrian Kelly, Patrick Lekgwara TDocument4 pagesInterdisciplinary Neurosurgery: Jimmy Ntimbani, Adrian Kelly, Patrick Lekgwara TKunni MardhiyahNo ratings yet
- Interdisciplinary Neurosurgery: Jimmy Ntimbani, Adrian Kelly, Patrick LekgwaraDocument4 pagesInterdisciplinary Neurosurgery: Jimmy Ntimbani, Adrian Kelly, Patrick LekgwaraAndres Eduardo GranadosNo ratings yet
- Neural Tube DefectsDocument15 pagesNeural Tube DefectsadriricaldeNo ratings yet
- 10.1007@s00381 020 04746 9Document12 pages10.1007@s00381 020 04746 9Alvaro Perez HenriquezNo ratings yet
- Espina BífidaDocument18 pagesEspina BífidaDamary Cifuentes ReyesNo ratings yet
- Lumbar Spinal Stenosis: Devin K. Binder, M.D., PH.D, Meic H. Schmidt, M.D., and Philip R. Weinstein, M.DDocument10 pagesLumbar Spinal Stenosis: Devin K. Binder, M.D., PH.D, Meic H. Schmidt, M.D., and Philip R. Weinstein, M.DYerni DaeliNo ratings yet
- Folic Acid and Neural Tube DefectsDocument127 pagesFolic Acid and Neural Tube DefectsarquivoslivrosNo ratings yet
- Spina Bifida Brochure 508compDocument20 pagesSpina Bifida Brochure 508compfsaajaNo ratings yet
- Acog Practice Bullet In: Neural Tube DefectsDocument12 pagesAcog Practice Bullet In: Neural Tube DefectsSILVIA GAONANo ratings yet
- Caringforthechildwith Spinabifida: Brandon G. Rocque,, Betsy D. Hopson,, Jeffrey P. BlountDocument13 pagesCaringforthechildwith Spinabifida: Brandon G. Rocque,, Betsy D. Hopson,, Jeffrey P. Blountyoussef alaouiNo ratings yet
- CP ResearchDocument13 pagesCP ResearchReinaJazzIslaNo ratings yet
- CPDocument10 pagesCPAnonymous vnv6QFNo ratings yet
- Notes On Spinal DysraphismDocument3 pagesNotes On Spinal DysraphismMicaela GarciaNo ratings yet
- Spina BifidaDocument33 pagesSpina BifidaRegine Prongoso DagumanpanNo ratings yet
- 324-Article Text-681-1-10-20220531Document11 pages324-Article Text-681-1-10-20220531Violine MartaliaNo ratings yet
- Spina Bifida - Pediatrics - MSD Manual Professional EditionDocument4 pagesSpina Bifida - Pediatrics - MSD Manual Professional EditionTONY GO AWAYNo ratings yet
- NIH Public Access: Author ManuscriptDocument14 pagesNIH Public Access: Author ManuscriptMeirani RizdaputriNo ratings yet
- ArticleDocument9 pagesArticleMaría José TvNo ratings yet
- J Child Neurol 2001 Fennell 58 63Document6 pagesJ Child Neurol 2001 Fennell 58 63Elena GatoslocosNo ratings yet
- Davis 2003Document9 pagesDavis 2003Apotik ApotekNo ratings yet
- Antenatal Diagnosis ofDocument6 pagesAntenatal Diagnosis ofnskhldNo ratings yet
- 1 PBDocument7 pages1 PBsahrirNo ratings yet
- 18 Ben20hamouda SfarDocument6 pages18 Ben20hamouda SfarGiovanni AtaideNo ratings yet
- Positional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery CliniDocument8 pagesPositional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery Clinilaljadeff12No ratings yet
- Spinalbifida 121213120324 Phpapp02Document28 pagesSpinalbifida 121213120324 Phpapp02Silvana María Espinoza CuadrosNo ratings yet
- Case Report: A Case of Caudal Regression Syndrome: Walking or Sitting?Document5 pagesCase Report: A Case of Caudal Regression Syndrome: Walking or Sitting?LisnainiMuchlisNo ratings yet
- Pattern of Encephaloceles A Case SeriesDocument4 pagesPattern of Encephaloceles A Case SeriesSayyid Hakam PerkasaNo ratings yet
- Approach To MacrocephalyDocument15 pagesApproach To MacrocephalywarunkumarNo ratings yet
- Neural Tube Defects and Folate: Case Far From Closed: ReviewsDocument8 pagesNeural Tube Defects and Folate: Case Far From Closed: ReviewsGeomar LaraNo ratings yet
- Segmental Costovertebral Malformations: Association With Neural Tube Defects. Report of 3 Cases and Review of The LiteratureDocument11 pagesSegmental Costovertebral Malformations: Association With Neural Tube Defects. Report of 3 Cases and Review of The LiteraturemusdalifahNo ratings yet
- Journal of Diagnostic Medical Sonography 2010 Moore 286 9Document4 pagesJournal of Diagnostic Medical Sonography 2010 Moore 286 9Hanarisha Putri AzkiaNo ratings yet
- Down's Syndrome and Spina BifidaDocument23 pagesDown's Syndrome and Spina BifidaKajal KaliaNo ratings yet
- Seminars in Fetal & Neonatal Medicine: N. Scott AdzickDocument6 pagesSeminars in Fetal & Neonatal Medicine: N. Scott AdzickTatiana Benito RojasNo ratings yet
- Alwahab2017 Article OccipitalMeningoencephaloceleC PDFDocument4 pagesAlwahab2017 Article OccipitalMeningoencephaloceleC PDFOvamelia JulioNo ratings yet
- Disorders of the Spinal Cord in ChildrenFrom EverandDisorders of the Spinal Cord in ChildrenMichael PikeNo ratings yet
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Media Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty SiraitDocument15 pagesMedia Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty Siraitnimas ayu kusumaningrumNo ratings yet
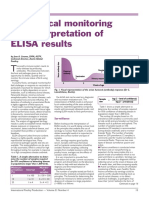
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- UKHO Survey Specification Acoustic V3 Jul18Document102 pagesUKHO Survey Specification Acoustic V3 Jul18Iqbal FauzanNo ratings yet
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- Concussionspaper 1Document6 pagesConcussionspaper 1api-350027909No ratings yet
- 270 lbs. man's 6-meal diet and workout planDocument10 pages270 lbs. man's 6-meal diet and workout planYuuki XDNo ratings yet
- Guide To Patient Support and Regional Cancer ServicesDocument76 pagesGuide To Patient Support and Regional Cancer Servicesgiovanna2004No ratings yet
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- Melidiosis FDocument24 pagesMelidiosis FVyramuthu AtputhanNo ratings yet
- Introduction To The Alpaca andDocument9 pagesIntroduction To The Alpaca andMai Chi PhạmNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- VGEC 2024_Thư mời hội nghịDocument8 pagesVGEC 2024_Thư mời hội nghịkhongquantam101010No ratings yet
- Nurs 5019 - Soap Note 41-60 Year OldDocument7 pagesNurs 5019 - Soap Note 41-60 Year Oldapi-308904543100% (1)
- Theory Critique of Boundaries in MarriageDocument8 pagesTheory Critique of Boundaries in MarriagepatrickakingNo ratings yet
- Ethics of Blood TransfusionDocument6 pagesEthics of Blood TransfusionHo Yong WaiNo ratings yet
- Plant Tissue Culture Media PDFDocument3 pagesPlant Tissue Culture Media PDFTitan Biotech100% (1)
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet