You might also like
- Clinical Laboratory Analysis - 2020 - Tao - Research and Discussion On The Evaluation Scheme of Reagent Lot To LotDocument9 pagesClinical Laboratory Analysis - 2020 - Tao - Research and Discussion On The Evaluation Scheme of Reagent Lot To LotLorena Ek MaciasNo ratings yet
- Analytical Evaluation of a Procalcitonin ImmunoassayDocument5 pagesAnalytical Evaluation of a Procalcitonin ImmunoassayneofherNo ratings yet
- Evaluation of Electrochemiluminescence Immunoassay PDFDocument12 pagesEvaluation of Electrochemiluminescence Immunoassay PDFajit jambhekarNo ratings yet
- Comparative Biological Data and Clinical Trial Design for CT-P10 and RTXDocument20 pagesComparative Biological Data and Clinical Trial Design for CT-P10 and RTXniajaplaniNo ratings yet
- Mller Bardorff2000Document9 pagesMller Bardorff2000Daniel ChaNo ratings yet
- K 052017Document8 pagesK 052017Adittya69No ratings yet
- Control Charts in Clinical LabsDocument8 pagesControl Charts in Clinical LabsLuisNo ratings yet
- Development of an LC-MS/MS Method for Quantitation of Deoxyglycychloxazol in Rat PlasmaDocument6 pagesDevelopment of an LC-MS/MS Method for Quantitation of Deoxyglycychloxazol in Rat Plasmajkc collegeNo ratings yet
- Mose Et Al 2015Document7 pagesMose Et Al 2015Nanda apriliantoNo ratings yet
- Practica 12 - Control de Calidad Externo Prueba Susceptibilidad A Drogas TBCDocument5 pagesPractica 12 - Control de Calidad Externo Prueba Susceptibilidad A Drogas TBCFredy Miguel Risco OrmeñoNo ratings yet
- Beriault 2015Document1 pageBeriault 2015Fouad RahiouyNo ratings yet
- Pre-Column Derivatization Method For DeterminingDocument7 pagesPre-Column Derivatization Method For DeterminingKuanNo ratings yet
- Poredjenje Mindray BC-5180 Vs Sysmex XN-1000Document6 pagesPoredjenje Mindray BC-5180 Vs Sysmex XN-1000Miroslav TomovicNo ratings yet
- IndikopublicationDocument8 pagesIndikopublicationKalai SelvanNo ratings yet
- Frid Lund 2016Document20 pagesFrid Lund 2016DoyoxNo ratings yet
- Cardiovascular Therapeutics - 2018 - Yuan - The Incidence of Atrial Fibrillation With Trastuzumab Treatment A SystematicDocument7 pagesCardiovascular Therapeutics - 2018 - Yuan - The Incidence of Atrial Fibrillation With Trastuzumab Treatment A SystematicOttofianus Hewick KalangiNo ratings yet
- Epilepsia - 2009 - La Marca - A New Rapid Micromethod For The Assay of Phenobarbital From Dried Blood Spots by LC TandemDocument5 pagesEpilepsia - 2009 - La Marca - A New Rapid Micromethod For The Assay of Phenobarbital From Dried Blood Spots by LC TandemWaode RahmahNo ratings yet
- The Radiolytic Studies of Ceftriaxone in The Solid State: AbstractDocument6 pagesThe Radiolytic Studies of Ceftriaxone in The Solid State: AbstractWinona DavinaNo ratings yet
- Barsanti-Innes The Oncologist - 2016Document8 pagesBarsanti-Innes The Oncologist - 2016Liz BethNo ratings yet
- Clinical ChemistryDocument19 pagesClinical Chemistrythrowawy100% (2)
- 10.1002@cam4.2284Document11 pages10.1002@cam4.2284Ricardo MarquesNo ratings yet
- Critical Value ReportingDocument7 pagesCritical Value Reportingjorguey100% (1)
- Serum Protein Profiles in Myasthenia Gravis: Ann Thorac SurgDocument8 pagesSerum Protein Profiles in Myasthenia Gravis: Ann Thorac SurgtotoedahNo ratings yet
- A UPLC-MS-MS Method For The Simultaneous Quantification of First-Line Antituberculars in Plasma and in PBMCsDocument4 pagesA UPLC-MS-MS Method For The Simultaneous Quantification of First-Line Antituberculars in Plasma and in PBMCservano1969No ratings yet
- A Novel Risk Analysis of Clinical Reference Dosimetry Based On Failure Modes and Effects AnalysisDocument7 pagesA Novel Risk Analysis of Clinical Reference Dosimetry Based On Failure Modes and Effects AnalysisMichelle LEINo ratings yet
- Shungo Imai Bs Takehiro Yamada PHD Kumiko Kasashi PHD Masaki Kobayashi PHD Ken Iseki PHDDocument7 pagesShungo Imai Bs Takehiro Yamada PHD Kumiko Kasashi PHD Masaki Kobayashi PHD Ken Iseki PHDMutiara SeptianiNo ratings yet
- UV Spectrophotometeric Analytical Method Development and Validation For The Determination of Telmisartan in Pharmaceutical Drug and Drug Formulation Tablet Dosage FormDocument6 pagesUV Spectrophotometeric Analytical Method Development and Validation For The Determination of Telmisartan in Pharmaceutical Drug and Drug Formulation Tablet Dosage FormEditor IJTSRDNo ratings yet
- AMP AssayValidation FinalDocument12 pagesAMP AssayValidation FinalMario Salinas100% (1)
- Dosimetric Verification of Radiotherapy Treatment Planning Systems: Results of IAEA Pilot StudyDocument10 pagesDosimetric Verification of Radiotherapy Treatment Planning Systems: Results of IAEA Pilot StudyOscar Javier GarciaNo ratings yet
- Tse 2014Document5 pagesTse 2014Ke XuNo ratings yet
- (ORI) Yucel Et Al. 2017. 53-1475821436Document5 pages(ORI) Yucel Et Al. 2017. 53-1475821436anisahfauziyyahNo ratings yet
- J Applied Clin Med Phys - 2020 - Mehrens - Survey Results of 3D CRT and IMRT Quality Assurance PracticeDocument7 pagesJ Applied Clin Med Phys - 2020 - Mehrens - Survey Results of 3D CRT and IMRT Quality Assurance Practicephutycharm15No ratings yet
- Standardized Laboratory Monitoring With Use of Isotretinoin in Acne - Hansen2016Document6 pagesStandardized Laboratory Monitoring With Use of Isotretinoin in Acne - Hansen2016Blu Punto ArtNo ratings yet
- 1_Relmacabtagene autoleucel (relma-cel) CD19 CAR-T therapy for adults with heavily pretreated relapsed or refractory large B-cell lymphoma in ChinaDocument13 pages1_Relmacabtagene autoleucel (relma-cel) CD19 CAR-T therapy for adults with heavily pretreated relapsed or refractory large B-cell lymphoma in ChinaFaras ArinalNo ratings yet
- 2829 FullDocument2 pages2829 FullSulaiman RasyidNo ratings yet
- Optical and Mechanical Clot Detection Methodologies A Comparison Study For Routine Coagulation TestingDocument5 pagesOptical and Mechanical Clot Detection Methodologies A Comparison Study For Routine Coagulation TestingEsther Jara GarcíaNo ratings yet
- Key Sunitinib-Related Biomarkers For Renal Cell CarcinomaDocument14 pagesKey Sunitinib-Related Biomarkers For Renal Cell CarcinomaDaniel CastanNo ratings yet
- 2 Ijmpsapr20172Document6 pages2 Ijmpsapr20172TJPRC PublicationsNo ratings yet
- Evaluation and Performance Characteristics of The Coagulation System ACL TOP Analyzer - HemosIL ReagentsDocument10 pagesEvaluation and Performance Characteristics of The Coagulation System ACL TOP Analyzer - HemosIL ReagentsEsther Jara GarcíaNo ratings yet
- LP 2 12 Establishing Your Functional Assay kKsuCj2SDocument116 pagesLP 2 12 Establishing Your Functional Assay kKsuCj2SogangaNo ratings yet
- Evaluation of critical laboratory values and communication protocolDocument2 pagesEvaluation of critical laboratory values and communication protocolTalent SackareNo ratings yet
- Jfda 27 01 323Document9 pagesJfda 27 01 323Mohamed Medhat AliNo ratings yet
- Organosys Ltd.,Noida For Type II Diabetes. First of All, Preclinical Tests Were Carried OutDocument5 pagesOrganosys Ltd.,Noida For Type II Diabetes. First of All, Preclinical Tests Were Carried OutSalman QureshiNo ratings yet
- Muhammad YounasDocument4 pagesMuhammad YounasHamid IqbalNo ratings yet
- Ablación Con Etanol QuistesDocument15 pagesAblación Con Etanol Quistesjessica MárquezNo ratings yet
- Research Articel (ESC)Document8 pagesResearch Articel (ESC)artaNo ratings yet
- Ijarcce 47Document7 pagesIjarcce 47talha42103No ratings yet
- 39708-Article Text-251234-3-10-20230319Document7 pages39708-Article Text-251234-3-10-20230319isamatias01No ratings yet
- COMPARATIVE BIOEQUIVALENCE STUDY CIMETIDINE GENERIC PROPRIETARY TABLETSDocument2 pagesCOMPARATIVE BIOEQUIVALENCE STUDY CIMETIDINE GENERIC PROPRIETARY TABLETSمحمد الفاتحNo ratings yet
- Anti-MCV Antibodies Diagnose Rheumatoid ArthritisDocument17 pagesAnti-MCV Antibodies Diagnose Rheumatoid ArthritisReda RamzyNo ratings yet
- 1 s2.0 S2667145X22000426 MainDocument12 pages1 s2.0 S2667145X22000426 MainHanane Mohammed BirkudarNo ratings yet
- Introduction To Lateral Flow Speedy Test DiagnosticsDocument3 pagesIntroduction To Lateral Flow Speedy Test DiagnosticsryalasfycoNo ratings yet
- CRP in Serum by NephelometryDocument13 pagesCRP in Serum by NephelometryFadlan HafizhNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument12 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNAL100% (1)
- A3 FullDocument2 pagesA3 FullApotik ApotekNo ratings yet
- Real World Effectiveness and Safety of Rituximab in The Treatment of Rheumatoid Arthritis: A Single Center Experience in TaiwanDocument9 pagesReal World Effectiveness and Safety of Rituximab in The Treatment of Rheumatoid Arthritis: A Single Center Experience in TaiwanTengku M Ridho AnharNo ratings yet
- Asam Traneksamat MelasmaDocument14 pagesAsam Traneksamat MelasmaFitrianidilaNo ratings yet
- Application and Optimization of Reference Change Values For Delta Checks in Clinical LaboratoryDocument8 pagesApplication and Optimization of Reference Change Values For Delta Checks in Clinical Laboratorymahmouda100No ratings yet
- A Novel Triple Therapy For ITP Using Hgh-Dose Dexamethasone, Low Dose Rituximab, and Cyclosporine (TT4)Document5 pagesA Novel Triple Therapy For ITP Using Hgh-Dose Dexamethasone, Low Dose Rituximab, and Cyclosporine (TT4)AdiNo ratings yet
- Afd 100526 037Document12 pagesAfd 100526 037Theresia Lumban GaolNo ratings yet
- CE Standard Brief Big Picture Chart Updated Sep 18Document25 pagesCE Standard Brief Big Picture Chart Updated Sep 18Theresia Lumban GaolNo ratings yet
- Briefing TemplateDocument8 pagesBriefing TemplateTheresia Lumban GaolNo ratings yet
- Pricelist 2022Document5 pagesPricelist 2022Theresia Lumban GaolNo ratings yet
- Nursing managers' perspectives on sick leave absencesDocument8 pagesNursing managers' perspectives on sick leave absencesTheresia Lumban GaolNo ratings yet
- Orientation AIDET Rev0614Document28 pagesOrientation AIDET Rev0614Theresia Lumban GaolNo ratings yet
- 4-H DawsonDocument31 pages4-H DawsonTheresia Lumban GaolNo ratings yet
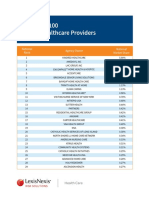
- Combined Top 100 Home Health and Hospice Rankings PDFDocument8 pagesCombined Top 100 Home Health and Hospice Rankings PDFTheresia Lumban GaolNo ratings yet
- SHP The PresentationDocument170 pagesSHP The PresentationTheresia Lumban GaolNo ratings yet
- (Deck) Partnership VoucherDocument16 pages(Deck) Partnership VoucherTheresia Lumban GaolNo ratings yet
- Work Placement Manual - Vet NursingDocument9 pagesWork Placement Manual - Vet NursingTheresia Lumban GaolNo ratings yet
- Company Profile Dekoruma For Business 2022Document31 pagesCompany Profile Dekoruma For Business 2022Theresia Lumban GaolNo ratings yet
- @NeoPlex COVID-19 Technical Information 20200324 - Rev1Document17 pages@NeoPlex COVID-19 Technical Information 20200324 - Rev1Theresia Lumban GaolNo ratings yet
- SHA's COVID-19 Community Surge PlanDocument23 pagesSHA's COVID-19 Community Surge PlanTheresia Lumban GaolNo ratings yet
- 2018-03-16 n2 Care at HomeDocument28 pages2018-03-16 n2 Care at HomeTheresia Lumban GaolNo ratings yet
- 0 R2f CH TRN Slides (WPSC) (v5-201118) (1) - 1630669999Document65 pages0 R2f CH TRN Slides (WPSC) (v5-201118) (1) - 1630669999Theresia Lumban GaolNo ratings yet
- The Cyanide MonographDocument647 pagesThe Cyanide MonographarribacampeonNo ratings yet
- E. Borjesson, Et Al. New Methods For Determinatios of Glyphosate and (Aminomenthyl) Phosphonic Acid in Water and SoilDocument10 pagesE. Borjesson, Et Al. New Methods For Determinatios of Glyphosate and (Aminomenthyl) Phosphonic Acid in Water and SoilmariNo ratings yet
- Validation of A Stability-Indicating RP-HPLC MethodDocument9 pagesValidation of A Stability-Indicating RP-HPLC MethodSELLAMI OmarNo ratings yet
- PDA: A Global Association: Proposed Revisions ToDocument38 pagesPDA: A Global Association: Proposed Revisions ToGrine FaroukNo ratings yet
- Evaluation of Certain Veterinary Drug Residues in Food: WHO Technical Report SeriesDocument130 pagesEvaluation of Certain Veterinary Drug Residues in Food: WHO Technical Report Seriesfaisal abbasNo ratings yet
- (INS-TG-EN) Ichroma Tn-I Plus - Rev.01 - 180404Document4 pages(INS-TG-EN) Ichroma Tn-I Plus - Rev.01 - 180404nam7124119100% (2)
- BR PlasmaQuant 9100 Series enDocument8 pagesBR PlasmaQuant 9100 Series enLucas AmorimNo ratings yet
- JPBAS 1 (2) 3chitralekha SainiDocument7 pagesJPBAS 1 (2) 3chitralekha SainiHarish KakraniNo ratings yet
- ASTM D2622-SulfurDocument12 pagesASTM D2622-SulfurBima Dzufakar100% (2)
- Certificate of Analysis: PassedDocument2 pagesCertificate of Analysis: PassedmwgageNo ratings yet
- Analysis Ascorbic Acid Citric Acid Benzoic Acid in Orange JuiceDocument12 pagesAnalysis Ascorbic Acid Citric Acid Benzoic Acid in Orange JuiceHuong Nguyen100% (1)
- Spectraa 50/55/110/220: VarianDocument16 pagesSpectraa 50/55/110/220: Varianrichard limNo ratings yet
- Determining Sulphur in Steel by ICP-AESDocument8 pagesDetermining Sulphur in Steel by ICP-AESngobaochanNo ratings yet
- Verification of spectrophotometric method for nitrate analysisDocument7 pagesVerification of spectrophotometric method for nitrate analysisBayu WiyantokoNo ratings yet
- Analytica 03 00027 v2Document12 pagesAnalytica 03 00027 v2Jesús SilvaNo ratings yet
- Sucrose/D-Glucose: Test-Combination For 22 Determinations EachDocument6 pagesSucrose/D-Glucose: Test-Combination For 22 Determinations EachVeronica DrgNo ratings yet
- Introduction to Spectrophotometry: Principles, Techniques and ApplicationsDocument19 pagesIntroduction to Spectrophotometry: Principles, Techniques and Applicationsabhinav_ramana100% (1)
- Validation of Analytical Methods - PRIMERDocument76 pagesValidation of Analytical Methods - PRIMERkchoksi2011100% (1)
- 1.method ValidationDocument4 pages1.method ValidationKalaivani VNo ratings yet
- A Validated RPHPLC Method For Simultaneous Estimation of Bronopol in Lactulose Solution UspDocument9 pagesA Validated RPHPLC Method For Simultaneous Estimation of Bronopol in Lactulose Solution Uspsunaina agarwalNo ratings yet
- 526Document49 pages526AlexSNo ratings yet
- Usp Diapositivas 1220 Ciclo de Vida EstadisticaDocument121 pagesUsp Diapositivas 1220 Ciclo de Vida EstadisticaROBINNo ratings yet
- Bhel UtDocument14 pagesBhel UtAnonymous 6k4VeeRNo ratings yet
- RP-HPLC Method Development and Validation of Dapagliflozin in Bulk and Tablet FormulationDocument6 pagesRP-HPLC Method Development and Validation of Dapagliflozin in Bulk and Tablet FormulationSriram NagarajanNo ratings yet
- Ijppr 2021Document16 pagesIjppr 2021Smita NayakNo ratings yet
- Analytical Method Development by High Performance Liquid ChromatographyDocument9 pagesAnalytical Method Development by High Performance Liquid ChromatographyEditor IJTSRDNo ratings yet
- SIGNAL To NOISE RATIO - Modern Practice of Gas ChromatographyDocument2 pagesSIGNAL To NOISE RATIO - Modern Practice of Gas Chromatographyanon_687115068No ratings yet
- Spectrophotometric Determination and Commercial Formulation Oftebuconazole Fungicide After Derivatization 2150 3494 1000133Document4 pagesSpectrophotometric Determination and Commercial Formulation Oftebuconazole Fungicide After Derivatization 2150 3494 1000133lox agencyNo ratings yet
- Design and Statistical Analysis of Method Transfer Studies For Biotechnology ProductsDocument27 pagesDesign and Statistical Analysis of Method Transfer Studies For Biotechnology ProductsDarshan PatelNo ratings yet
- CelicoxibDocument8 pagesCelicoxibDavid Raju GollapudiNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)