You might also like
- LEC 5 RBC METABOLISM AND Membrane StructureDocument30 pagesLEC 5 RBC METABOLISM AND Membrane StructureFrancis ValdezNo ratings yet
- Blood and Lymph (Autosaved)Document46 pagesBlood and Lymph (Autosaved)Shaikh SaqibNo ratings yet
- Physiology Lecture 2: RBC S Characteristics, Function and FormationDocument20 pagesPhysiology Lecture 2: RBC S Characteristics, Function and FormationdarkboiNo ratings yet
- Normocytic Normochromic AnemiaDocument18 pagesNormocytic Normochromic AnemiaElaizha PagulayanNo ratings yet
- Chapter 17 - Blood: J.F. Thompson, Ph.D. & J.R. Schiller, Ph.D. & G. Pitts, PH.DDocument50 pagesChapter 17 - Blood: J.F. Thompson, Ph.D. & J.R. Schiller, Ph.D. & G. Pitts, PH.Dghisma ocvintiaNo ratings yet
- RBC DISORDERS StudentsDocument84 pagesRBC DISORDERS Studentskimberly abianNo ratings yet
- Mtap 2 HematologyDocument15 pagesMtap 2 HematologyNaomi NicoleNo ratings yet
- Haemolytic Anaemia: DR Nurul Fahmiza Tumiran P109273Document55 pagesHaemolytic Anaemia: DR Nurul Fahmiza Tumiran P109273Nurul FahmizaNo ratings yet
- Chapter 10 BloodDocument3 pagesChapter 10 BloodinitaygracileshayneNo ratings yet
- Hematologic SystemDocument33 pagesHematologic SystemSteffanie TalaueNo ratings yet
- Anemia 2024Document50 pagesAnemia 2024b9p6vmfnc4No ratings yet
- BLOOD Update-1Document56 pagesBLOOD Update-1ahmadfadi343No ratings yet
- S7L01 - BloodDocument49 pagesS7L01 - BloodSuad WarsameNo ratings yet
- Between The Erythrocytes and PlasmaDocument5 pagesBetween The Erythrocytes and Plasmajonette carataoNo ratings yet
- Red Cell.1Document25 pagesRed Cell.1Jude ChinecheremNo ratings yet
- Blood and LymphaticDocument4 pagesBlood and LymphaticCKNo ratings yet
- BloodDocument5 pagesBloodChelsie NicoleNo ratings yet
- Sânge de Sâng Întrebă Și HemoglobinăDocument2 pagesSânge de Sâng Întrebă Și HemoglobinăAurelia AlexandraNo ratings yet
- Test Your Knowledge. True or FalseDocument11 pagesTest Your Knowledge. True or Falsejelly beanNo ratings yet
- Human Anatomy & Physiology Blood: By: Lawrence G. GamboaDocument11 pagesHuman Anatomy & Physiology Blood: By: Lawrence G. GamboaLawrenceNo ratings yet
- Week 1 Blood Student Notes 1Document12 pagesWeek 1 Blood Student Notes 1pham vanNo ratings yet
- Cardiovascular System - BloodDocument8 pagesCardiovascular System - BloodVernice LopezNo ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Red Blood Cell BiochemistryDocument19 pagesRed Blood Cell BiochemistryPrincewill SeiyefaNo ratings yet
- Blood Performs A Number of Functions Dealing WithDocument52 pagesBlood Performs A Number of Functions Dealing Withعلي العراقي فاديNo ratings yet
- Ilmu Kesehatan Anak: Judul Materi: Pendekatan Anemia Pada AnakDocument103 pagesIlmu Kesehatan Anak: Judul Materi: Pendekatan Anemia Pada AnakDhanin WitedjaNo ratings yet
- Hemato 1Document56 pagesHemato 1toot aliNo ratings yet
- APP2 E1 NoteDocument28 pagesAPP2 E1 NotelifecostNo ratings yet
- Circulatory System Part I - BloodDocument123 pagesCirculatory System Part I - BloodAngelyn DomingoNo ratings yet
- Erythrocytes Red Blood CellsDocument54 pagesErythrocytes Red Blood Cellsclarence fernandezNo ratings yet
- BloodDocument13 pagesBloodمحمد احمدNo ratings yet
- RBC Production and DestructionDocument44 pagesRBC Production and DestructionNehemiah FranciscoNo ratings yet
- Blood Chapter 11Document5 pagesBlood Chapter 11Michoe BanugNo ratings yet
- Hematopoiesis and ErytherokiniticsDocument20 pagesHematopoiesis and ErytherokiniticsShahid F.S.D.No ratings yet
- HEMATOLOGY (Week 2) LABDocument8 pagesHEMATOLOGY (Week 2) LABJessica PontanaresNo ratings yet
- Red Blood Cells, Anemia, and PolycythemiaDocument7 pagesRed Blood Cells, Anemia, and PolycythemiaShi no Me100% (1)
- Blood PhysiologyDocument223 pagesBlood PhysiologyBindiya MangarNo ratings yet
- Blood - Mcon 01 (Lec) A4Document5 pagesBlood - Mcon 01 (Lec) A4Lemon AdeNo ratings yet
- Hemolytic Anemia Basic Concepts NotesDocument9 pagesHemolytic Anemia Basic Concepts NotesA-sHakour AadenNo ratings yet
- Anatomy and Physiology With PhatophysiologyDocument6 pagesAnatomy and Physiology With PhatophysiologyJustine Mae OyongNo ratings yet
- AnaemiasDocument60 pagesAnaemiasbvkjtzrvnyNo ratings yet
- 1 Blood22Document48 pages1 Blood22Wizz Háķìm ĻêşòwNo ratings yet
- Blood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19Document62 pagesBlood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19AntarleenaNo ratings yet
- Topics of This Lecture: RBC: - Structural Characteristics - Hemoglobin - Erythropoiesis - Erythrocytes DestructionDocument23 pagesTopics of This Lecture: RBC: - Structural Characteristics - Hemoglobin - Erythropoiesis - Erythrocytes DestructionHashim GhazoNo ratings yet
- 1 Intro RBCsDocument59 pages1 Intro RBCsDanz ShNo ratings yet
- Hemolytic Anemia IntrinsicDocument14 pagesHemolytic Anemia IntrinsicSophia Gail ChingNo ratings yet
- Zoology Full PDF EMDocument108 pagesZoology Full PDF EMSmiruthi RavichandranNo ratings yet
- CARDIOVASCULARDocument20 pagesCARDIOVASCULARpriya garciaNo ratings yet
- Chapter Blood: RBC Platelet HemostasisDocument89 pagesChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- 2020 Red Blood Cells (Erythrocytes)Document33 pages2020 Red Blood Cells (Erythrocytes)Raymon Villagonzalo TocoyoNo ratings yet
- Blood Physiology: Biconcave Discs 120 DaysDocument6 pagesBlood Physiology: Biconcave Discs 120 DaysHanamiNo ratings yet
- Dr. Sailendra Nayak Assistant Professor MedicineDocument49 pagesDr. Sailendra Nayak Assistant Professor MedicineAishwarya JeeNo ratings yet
- Transes Anaphy BloodDocument5 pagesTranses Anaphy BloodPia LouiseNo ratings yet
- Heamatology Dr. Osama PDFDocument94 pagesHeamatology Dr. Osama PDFAnmar ZawahraNo ratings yet
- Blood: Erythropoeisis by U.SivakumarDocument41 pagesBlood: Erythropoeisis by U.SivakumarAkash JaatNo ratings yet
- RBC DisordersDocument70 pagesRBC DisordersNdor Baribolo100% (1)
- Anaemias: P. Manyau School of Pharmacy University of ZimbabweDocument41 pagesAnaemias: P. Manyau School of Pharmacy University of Zimbabwebrian mgabiNo ratings yet
- Lecture 2 - Clinical Pathology - AnemiaDocument56 pagesLecture 2 - Clinical Pathology - AnemiaSamuel GitongaNo ratings yet
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoFrom EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoNo ratings yet
- Module 3 Do Not Edit Template Only - XLSX - Sheet1Document3 pagesModule 3 Do Not Edit Template Only - XLSX - Sheet1DIANA CAMILLE CARITATIVONo ratings yet
- PHCP - Unit 2 Putline - ReviewerDocument4 pagesPHCP - Unit 2 Putline - ReviewerDIANA CAMILLE CARITATIVONo ratings yet
- Quiz La Liga FilipinaDocument2 pagesQuiz La Liga FilipinaDIANA CAMILLE CARITATIVONo ratings yet
- Phos 313 - Activity No 7 PhosDocument6 pagesPhos 313 - Activity No 7 PhosDIANA CAMILLE CARITATIVONo ratings yet
- Pmoc ReviewerDocument10 pagesPmoc ReviewerDIANA CAMILLE CARITATIVONo ratings yet
- Continuation HEMOPHILIADocument3 pagesContinuation HEMOPHILIADIANA CAMILLE CARITATIVONo ratings yet
- Arta ReviewerDocument11 pagesArta ReviewerDIANA CAMILLE CARITATIVONo ratings yet
- Greek and Egyptian CivilizationDocument3 pagesGreek and Egyptian CivilizationDIANA CAMILLE CARITATIVONo ratings yet
- Introduction To GeneticsDocument3 pagesIntroduction To Geneticsjerni2012No ratings yet
- PlasmidsDocument25 pagesPlasmidsbijay karki100% (3)
- Biotechnology Regulatory Requirements On Continuous Manufacturing For Monoclonal AntibodiesDocument75 pagesBiotechnology Regulatory Requirements On Continuous Manufacturing For Monoclonal AntibodiesrayyitsaiNo ratings yet
- 1757 1626 1 333Document5 pages1757 1626 1 333Ade CandraNo ratings yet
- Nutrition in ProtozoaDocument6 pagesNutrition in Protozoaapi-481318101100% (3)
- Part3 Clinical ChemistryDocument4 pagesPart3 Clinical ChemistryGodofredo Hermosura100% (1)
- Cell Injury and Death: By: Taleya HidayatullahDocument49 pagesCell Injury and Death: By: Taleya HidayatullahtaleyaNo ratings yet
- Evaluating Antimicrobial Activity of Aloe Vera Plant Extract in Human LifeDocument3 pagesEvaluating Antimicrobial Activity of Aloe Vera Plant Extract in Human LifeMuhammad NaseerNo ratings yet
- Intro Bio Chapter 12 Fall 2012Document72 pagesIntro Bio Chapter 12 Fall 2012Aadil KhanNo ratings yet
- 400-001!06!13-A - API NH System BioMerieux Product InsertDocument13 pages400-001!06!13-A - API NH System BioMerieux Product InsertRickyNo ratings yet
- Seymour Schools Nov 6 COVID LetterDocument2 pagesSeymour Schools Nov 6 COVID LetterThe Valley IndyNo ratings yet
- 2009-08-25 Nowak Thyroid PDFDocument47 pages2009-08-25 Nowak Thyroid PDFEndalew Alemu NathanNo ratings yet
- Pathology Revision E6.5Document130 pagesPathology Revision E6.5vikashchahal1987No ratings yet
- Medical Immunology (7th Ed - 2020)Document474 pagesMedical Immunology (7th Ed - 2020)Sevim AkçağlarNo ratings yet
- Final Paper 1Document140 pagesFinal Paper 1Ramil LucasNo ratings yet
- 2021-03 - Newsletter Microbiology Standards N22EN 280131 - CompressedDocument7 pages2021-03 - Newsletter Microbiology Standards N22EN 280131 - Compressedkhoi moleNo ratings yet
- Y8 Biology Worksheet Task 1,2 and 3 SerenaDocument3 pagesY8 Biology Worksheet Task 1,2 and 3 SerenaSERENA TAYNo ratings yet
- Cell Asad NotesDocument23 pagesCell Asad NotesHess AhmedNo ratings yet
- Sindorme de Hutchinson-GilfordDocument8 pagesSindorme de Hutchinson-GilfordMaria Garcia FernandezNo ratings yet
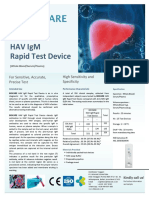
- Brosur BIOCARE HAV IgM Rapid Test Device OKDocument1 pageBrosur BIOCARE HAV IgM Rapid Test Device OKAlfarizi Julistyo S.No ratings yet
- ISLab P5 - Bacterial Agglutination TestDocument8 pagesISLab P5 - Bacterial Agglutination TestDanielle Anne LambanNo ratings yet
- Dgge (Denaturing Gradient Gel Electrophoresis)Document4 pagesDgge (Denaturing Gradient Gel Electrophoresis)twangpanNo ratings yet
- ARCHITECT - IA-CC - ASSAY MenuDocument4 pagesARCHITECT - IA-CC - ASSAY MenuKostya OnyshchukNo ratings yet
- Biotechnology and Its Application Class 12 Notes Biology Chapter 12 (PDF)Document8 pagesBiotechnology and Its Application Class 12 Notes Biology Chapter 12 (PDF)Saishreeta JoshiNo ratings yet
- SUBHADIPA MAJUMDER2022-07-22Cell PotencyDocument2 pagesSUBHADIPA MAJUMDER2022-07-22Cell PotencySuvNo ratings yet
- Cambridge International AS & A Level: Biology 9700/11Document20 pagesCambridge International AS & A Level: Biology 9700/11Shawn YosaNo ratings yet
- Gardasil HPV VaccineDocument4 pagesGardasil HPV VaccineThorsteinn ThorsteinssonNo ratings yet
- Test Bank For Molecular Biology Principles and Practice 1st Edition Michael M CoxDocument6 pagesTest Bank For Molecular Biology Principles and Practice 1st Edition Michael M CoxglendavictoriabbkNo ratings yet
- Bcr-Abl: Cancer Protein Structure and Function: About This WorksheetDocument2 pagesBcr-Abl: Cancer Protein Structure and Function: About This WorksheetRed FoxNo ratings yet
- Biological Sciences Research3Document21 pagesBiological Sciences Research3Neeta M UdariNo ratings yet