You might also like
- Medicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenDocument13 pagesMedicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenAsniar RNo ratings yet
- Jurnal ReadingDocument5 pagesJurnal ReadingUjang HasanNo ratings yet
- Hearing Status of Children Under Five Years Old in Jatinangor DistrictDocument5 pagesHearing Status of Children Under Five Years Old in Jatinangor DistricterickNo ratings yet
- Swanepoel Telehealth (2010) PDFDocument24 pagesSwanepoel Telehealth (2010) PDFRoberta VianaNo ratings yet
- 2020 - LSHSS 20 00089Document13 pages2020 - LSHSS 20 00089Meva'a RogerNo ratings yet
- A Survey of Deaf Mutes: Original ArticleDocument4 pagesA Survey of Deaf Mutes: Original Articleomelbat-1No ratings yet
- Jurnal Newborn Hearing ScreningDocument13 pagesJurnal Newborn Hearing ScreningCitra LyadhaNo ratings yet
- 166929-Article Text-498394-1-10-20200724Document9 pages166929-Article Text-498394-1-10-20200724Swab IndonesiaNo ratings yet
- OutDocument13 pagesOutJoshua LuNo ratings yet
- Features of Unilateral Hearing Loss Detected by Newborn Hearing ScreeningDocument9 pagesFeatures of Unilateral Hearing Loss Detected by Newborn Hearing Screening21 TMHNo ratings yet
- Evaluation of Noise-Induced Hearing Loss in Young People Using A Web-Based Survey TechniqueDocument9 pagesEvaluation of Noise-Induced Hearing Loss in Young People Using A Web-Based Survey TechniqueJesusita Ortiz CollazosNo ratings yet
- 2 PB PDFDocument5 pages2 PB PDFmelivha otaraniNo ratings yet
- Hearing AidDocument9 pagesHearing AidClever ImaniaNo ratings yet
- Keywords: Congenital Deafness, Family Support, Early DetectionDocument8 pagesKeywords: Congenital Deafness, Family Support, Early DetectionAlifia Nurdani DarmawanNo ratings yet
- Fulltext02 PDFDocument28 pagesFulltext02 PDFGabriel CarterNo ratings yet
- Some Guiding Models of Voice Therapy For ChildrenDocument15 pagesSome Guiding Models of Voice Therapy For ChildrenCarlos ValenciaNo ratings yet
- Jamaotolaryngology Le Clercq 2018 Oi 180029Document8 pagesJamaotolaryngology Le Clercq 2018 Oi 180029Agustina TambingNo ratings yet
- Clinical Study: Newborn Hearing Screening and Early Diagnostic in The NICUDocument11 pagesClinical Study: Newborn Hearing Screening and Early Diagnostic in The NICUannisanangNo ratings yet
- Knowledge, Attitude of Sikkim Primary School Teachers About Paediatric Hearing LossDocument6 pagesKnowledge, Attitude of Sikkim Primary School Teachers About Paediatric Hearing LossMaria P12No ratings yet
- Deaf Mute PaperDocument11 pagesDeaf Mute PaperneviNo ratings yet
- Ch7 Herman and MorganDocument11 pagesCh7 Herman and MorganIbrahim Al AdhamNo ratings yet
- 1 s2.0 S0165587620306959 MainDocument5 pages1 s2.0 S0165587620306959 MainMiguel GómezNo ratings yet
- Minimal Hearing Loss From A Failure Based Approach To Evidence Based Practice 2016Document14 pagesMinimal Hearing Loss From A Failure Based Approach To Evidence Based Practice 2016Gloria Thomas100% (1)
- Training Adults and Children With An Autism Spectrum Disorder To Be Compliant With A Clinical Dental Assessment Using A TEACCH-Based ApproachDocument10 pagesTraining Adults and Children With An Autism Spectrum Disorder To Be Compliant With A Clinical Dental Assessment Using A TEACCH-Based ApproachSpecial CareNo ratings yet
- Self Reported Knowledgeand Behaviors Relatedto Oraland Dental Healthin Turkish ChildrenDocument15 pagesSelf Reported Knowledgeand Behaviors Relatedto Oraland Dental Healthin Turkish ChildrenArsalan Ahmed chakibNo ratings yet
- Johnd 04 0022Document7 pagesJohnd 04 0022Fahheemm AahmedNo ratings yet
- Original Article: Consanguinity and Hearing Impairment in A Deaf SchoolDocument6 pagesOriginal Article: Consanguinity and Hearing Impairment in A Deaf SchoolrennodhanyNo ratings yet
- Artigo 2 OKDocument14 pagesArtigo 2 OKdruvao136No ratings yet
- 02 Review PDFDocument10 pages02 Review PDFDanan LaksetyaNo ratings yet
- 10 1016@j Ijporl 2019 06 019Document7 pages10 1016@j Ijporl 2019 06 019Eva PerdanaNo ratings yet
- MAO 0b013e3182814d2cDocument8 pagesMAO 0b013e3182814d2cCoAsst MuhammadNuhAlhudawyNo ratings yet
- Childhood Hearing Health: Educating For Prevention of Hearing LossDocument6 pagesChildhood Hearing Health: Educating For Prevention of Hearing LossrennodhanyNo ratings yet
- HIPOACUSIA6Document5 pagesHIPOACUSIA6cristianNo ratings yet
- Newborn Hearing ScreeningDocument3 pagesNewborn Hearing ScreeningHamam KusumaganiNo ratings yet
- 1 SM PDFDocument5 pages1 SM PDFJaya Wira RajaNo ratings yet
- Early Identification of Hearing Loss in HighDocument4 pagesEarly Identification of Hearing Loss in HighKakaNo ratings yet
- Assignment Topic:: NameDocument9 pagesAssignment Topic:: Namehuraira bhattiNo ratings yet
- DTSCH Arztebl Int-117 0690Document12 pagesDTSCH Arztebl Int-117 0690CoAsst MuhammadNuhAlhudawyNo ratings yet
- Advocacy HIDocument2 pagesAdvocacy HIJamesAnthonyNo ratings yet
- whd2016 Brochure en 2Document16 pageswhd2016 Brochure en 2api-311125682No ratings yet
- Passive Smoking A Possible Risk Factor For Development of Minimal Hearing Loss in ChildrenDocument1 pagePassive Smoking A Possible Risk Factor For Development of Minimal Hearing Loss in ChildrenRamona StefanNo ratings yet
- 2022 2097133Document12 pages2022 2097133Pablo SepulvedaNo ratings yet
- J Paediatrics Child Health - 2012 - Onslow - Management of Childhood StutteringDocument4 pagesJ Paediatrics Child Health - 2012 - Onslow - Management of Childhood Stutteringfereshteh.mzNo ratings yet
- Effects of Maternal Singing During Kangaroo Care On Maternal Anxiety Wellbeing and Mother-Infant Relationship After Preterm Birth A Mixed Methods SDocument21 pagesEffects of Maternal Singing During Kangaroo Care On Maternal Anxiety Wellbeing and Mother-Infant Relationship After Preterm Birth A Mixed Methods SZikri AhmadNo ratings yet
- Hearing Impaired Children in Turkey and Their Education: DavidDocument6 pagesHearing Impaired Children in Turkey and Their Education: DavidBetül Özsoy TanrıkuluNo ratings yet
- Randomized Trial of Four Noise-Induced Hearing Loss and Tinnitus Prevention Interventions For ChildrenDocument9 pagesRandomized Trial of Four Noise-Induced Hearing Loss and Tinnitus Prevention Interventions For ChildrenMaríaAlejandraRiveraNo ratings yet
- University of Botswana: Department of Educational FoundationsDocument58 pagesUniversity of Botswana: Department of Educational FoundationsChangu Matildah JacobNo ratings yet
- Oral Health 1-3&5Document38 pagesOral Health 1-3&5Umar FarouqNo ratings yet
- HSC 430 Childhood Disease PaperDocument10 pagesHSC 430 Childhood Disease Paperapi-502687231No ratings yet
- Accepted Manuscript: Accepted Article Preview: Published Ahead of Advance Online PublicationDocument31 pagesAccepted Manuscript: Accepted Article Preview: Published Ahead of Advance Online PublicationireneaureliaNo ratings yet
- N BhvygvDocument7 pagesN BhvygvKirana SmartyaNo ratings yet
- Challenges of Participation For Deaf Children in Early Childhood ProgramsDocument61 pagesChallenges of Participation For Deaf Children in Early Childhood ProgramsJonry CuyagNo ratings yet
- Late Diagnosis of Congenital Hearing Impairment in Children - The Parents' Experiences and OpinionsDocument10 pagesLate Diagnosis of Congenital Hearing Impairment in Children - The Parents' Experiences and OpinionsDwi KhoirriyaniNo ratings yet
- The Impact of Voice Disorders Among Teachers: Vocal Complaints, Treatment-Seeking Behavior, Knowledge of Vocal Care, and Voice-Related AbsenteeismDocument6 pagesThe Impact of Voice Disorders Among Teachers: Vocal Complaints, Treatment-Seeking Behavior, Knowledge of Vocal Care, and Voice-Related AbsenteeismDomenica AvilaNo ratings yet
- Diteksi Dini Cegah Disabilitas Pendengaran Dheajeng Putri Alintang HDocument10 pagesDiteksi Dini Cegah Disabilitas Pendengaran Dheajeng Putri Alintang HAlifio DeaNo ratings yet
- Key Facts: Congenital CausesDocument3 pagesKey Facts: Congenital CausesStar DustNo ratings yet
- Risk Factors of Hearing Loss in Children Under 10 Years of Age - A Clinical Study in A Tertiary Care CentreDocument6 pagesRisk Factors of Hearing Loss in Children Under 10 Years of Age - A Clinical Study in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Speech Recognition Abilities in Noise For Children With Severe To Profound Unilateral Hearing ImpairmentDocument9 pagesSpeech Recognition Abilities in Noise For Children With Severe To Profound Unilateral Hearing ImpairmentKhaled Al-GhamdiNo ratings yet
- Hearing ImpairmentDocument3 pagesHearing ImpairmentTABLAC, Abegail AgpaloNo ratings yet
- Opoku Et Al. - Understanding The Parental Experiences of Raising Deaf Children in GhanaDocument21 pagesOpoku Et Al. - Understanding The Parental Experiences of Raising Deaf Children in GhanaPablo VasquezNo ratings yet
- Leigh - Inclusive Education and Personal DevelopmentDocument10 pagesLeigh - Inclusive Education and Personal DevelopmentPablo VasquezNo ratings yet
- Cejas Et Al. - Quality of Life-CI: Development of An Early Childhood Parent-Proxy & Adolescent VersionDocument28 pagesCejas Et Al. - Quality of Life-CI: Development of An Early Childhood Parent-Proxy & Adolescent VersionPablo VasquezNo ratings yet
- Razafimahefa-Raoelina Et Al. - Self-And Parental Assessment of Quality of Life in Child Cochlear Implant BearersDocument5 pagesRazafimahefa-Raoelina Et Al. - Self-And Parental Assessment of Quality of Life in Child Cochlear Implant BearersPablo VasquezNo ratings yet
- Walsh - Family TherapyDocument26 pagesWalsh - Family TherapyPablo Vasquez100% (1)
- Scherer Et Al. - Mental Health Support For Children and Adolescents With Hearing LossDocument11 pagesScherer Et Al. - Mental Health Support For Children and Adolescents With Hearing LossPablo VasquezNo ratings yet
- Glover - The Deaf Child-Challenges in Management - A Parent's PerspectiveDocument4 pagesGlover - The Deaf Child-Challenges in Management - A Parent's PerspectivePablo VasquezNo ratings yet
- Wong Et Al. - Psychosocial Development of 5-Year-Old Children With Hearing LossDocument13 pagesWong Et Al. - Psychosocial Development of 5-Year-Old Children With Hearing LossPablo VasquezNo ratings yet
- Luterman - Early Childhood Deafness: A 50-Year PerspectiveDocument5 pagesLuterman - Early Childhood Deafness: A 50-Year PerspectivePablo VasquezNo ratings yet
- Whicker Et Al. - Parent Challenges, Perspectives and Experiences Caring For Children Who Are Deaf or Hard-Of-Hearing With Other DisabilitiesDocument8 pagesWhicker Et Al. - Parent Challenges, Perspectives and Experiences Caring For Children Who Are Deaf or Hard-Of-Hearing With Other DisabilitiesPablo VasquezNo ratings yet
- Depression in Hearing-Impaired ChildrenDocument5 pagesDepression in Hearing-Impaired ChildrenPablo VasquezNo ratings yet
- Henderson Et Al. - Parent-to-Parent Support For Parents With Children Who Are Deaf or Hard of HearingDocument12 pagesHenderson Et Al. - Parent-to-Parent Support For Parents With Children Who Are Deaf or Hard of HearingPablo VasquezNo ratings yet
- Family Empowerment: Supporting Language Development in Young Children Who Are Deaf or Hard of HearingDocument25 pagesFamily Empowerment: Supporting Language Development in Young Children Who Are Deaf or Hard of HearingPablo VasquezNo ratings yet
- Stress and Child DevelopmentDocument20 pagesStress and Child DevelopmentPablo VasquezNo ratings yet
- Hearing Impairment, Work, and Vocational EnablementDocument7 pagesHearing Impairment, Work, and Vocational EnablementPablo VasquezNo ratings yet
- ESL Questions About EverythingDocument17 pagesESL Questions About EverythingBrenda AldoNo ratings yet
- Writing Inquiry Lesson PlanDocument15 pagesWriting Inquiry Lesson PlankokilavanniNo ratings yet
- NSTP HandoutsDocument38 pagesNSTP HandoutsAira Aquino0% (1)
- Lesson 21Document2 pagesLesson 21Beberly Kim AmaroNo ratings yet
- Business Immersion ProjectDocument74 pagesBusiness Immersion ProjectArchana SagarNo ratings yet
- 2nd Cot KoDocument9 pages2nd Cot KoMackie YlananNo ratings yet
- Cbpo ChecklistDocument17 pagesCbpo ChecklistAnna-KatrinaNo ratings yet
- Flexsim in AcademiaDocument143 pagesFlexsim in Academiaresearcher-690955No ratings yet
- School Ict - Action PlanDocument4 pagesSchool Ict - Action PlanEmilia MalabananNo ratings yet
- Draft Mini Project Question - 20212022Document4 pagesDraft Mini Project Question - 20212022Thulasi 2036No ratings yet
- Students' Self PerceivedDocument14 pagesStudents' Self PerceivedainasuhaNo ratings yet
- JCCMA Accreditation Application FormDocument2 pagesJCCMA Accreditation Application FormSergio MartinsNo ratings yet
- CogAT Form 7 Overview Lincoln PS 050615Document55 pagesCogAT Form 7 Overview Lincoln PS 050615Ashida SarodeNo ratings yet
- Razrabotka Uroka 2 Klass Kazakh Traditions and Customs 2021Document10 pagesRazrabotka Uroka 2 Klass Kazakh Traditions and Customs 20211 2100% (2)
- The Ultimate Chemistry NotesDocument33 pagesThe Ultimate Chemistry NotesChelsea Chee Ching IianNo ratings yet
- Reiser and BalderasDocument3 pagesReiser and BalderasRham BlaimNo ratings yet
- POSTER: Human Services CareerDocument1 pagePOSTER: Human Services CareerBeatriz AlvaradoNo ratings yet
- Corporate Reporting I Course Outline FINALDocument6 pagesCorporate Reporting I Course Outline FINALemeraldNo ratings yet
- Delhi Public School Mahendra Hills (Feeder School of DPS Nacharam)Document2 pagesDelhi Public School Mahendra Hills (Feeder School of DPS Nacharam)naveen theerthala100% (1)
- Failure Is Instructive. The Person Who Really Thinks Learns Quite As Much From His Failures As From His Successes.Document6 pagesFailure Is Instructive. The Person Who Really Thinks Learns Quite As Much From His Failures As From His Successes.Sirak ArekiNo ratings yet
- Strama - Finals and Grading RubricsDocument2 pagesStrama - Finals and Grading RubricsKyleNo ratings yet
- Summative MathDocument9 pagesSummative MathKangNo ratings yet
- Facilitating LearningDocument4 pagesFacilitating LearningCamille MendozaNo ratings yet
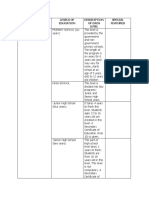
- Name of Country Levels of Education Description of Each Level Special Features 1. AustraliaDocument5 pagesName of Country Levels of Education Description of Each Level Special Features 1. AustraliaJohn David R. ValenciaNo ratings yet
- Impt Methods and ApproachesDocument68 pagesImpt Methods and ApproachesAnonymous KW9qyWkNo ratings yet
- Complete Research 12Document50 pagesComplete Research 12nicole friasNo ratings yet
- Learning Theories and PrinciplesDocument12 pagesLearning Theories and PrinciplesJenne Parido86% (7)
- Satyawati-Guest Faculty Notification LatestDocument1 pageSatyawati-Guest Faculty Notification LatestGupta JiNo ratings yet
- 15 B 1 AerospaceEngineering 0Document52 pages15 B 1 AerospaceEngineering 0Sam IraniNo ratings yet
- AB-ECM FlowchartDocument2 pagesAB-ECM FlowchartCarlosJohn02100% (1)