You might also like
- Pancreatic Islets Hormones Regulate Blood GlucoseDocument4 pagesPancreatic Islets Hormones Regulate Blood GlucoseSophia OcayNo ratings yet
- Metabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaDocument60 pagesMetabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaAmanda PutriNo ratings yet
- B Y: - Idr. Megha Gaur BDS IDocument89 pagesB Y: - Idr. Megha Gaur BDS IRishab GaurNo ratings yet
- Clinical SignificanceDocument31 pagesClinical Significancejav israelNo ratings yet
- Integration of Metabolism PathwaysDocument68 pagesIntegration of Metabolism PathwaysCahyani Tiara Safitri100% (1)
- Chapter 2 P-2 Enzyme-Inhibition 1Document39 pagesChapter 2 P-2 Enzyme-Inhibition 1Raihan I. SakibNo ratings yet
- Digestion and Absorption of Carbohydrates: by Arpitha 3 BnysDocument31 pagesDigestion and Absorption of Carbohydrates: by Arpitha 3 BnysBig ZeroNo ratings yet
- Digestive System: Carbohydrate, Protein and Fat DigestionDocument45 pagesDigestive System: Carbohydrate, Protein and Fat DigestionhiNo ratings yet
- Biochem Lec Term Paper HypoglycemiaDocument8 pagesBiochem Lec Term Paper Hypoglycemiaapi-318284296No ratings yet
- Integration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentDocument63 pagesIntegration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentGriffinNo ratings yet
- Insulin and Glucagon Regulation of Metabolic HomeostasisDocument40 pagesInsulin and Glucagon Regulation of Metabolic HomeostasisEka HabinaNo ratings yet
- HMPDocument44 pagesHMPraanja2No ratings yet
- Git Biochemistry of GitDocument9 pagesGit Biochemistry of GitSibatNo ratings yet
- 16 Pathology of Lipid MetDocument52 pages16 Pathology of Lipid MetyasingadaNo ratings yet
- Ion TransportFrom EverandIon TransportDavid KeelingNo ratings yet
- Metabolic Interrelationships Rev 07-11-2014Document82 pagesMetabolic Interrelationships Rev 07-11-2014algutNo ratings yet
- Understanding Metabolism of CarbohydratesDocument48 pagesUnderstanding Metabolism of CarbohydratesAbdullah TheNo ratings yet
- Hexose Mono Phosphate (HMP) ShuntDocument28 pagesHexose Mono Phosphate (HMP) ShuntVishesh JainNo ratings yet
- Amino SugarsDocument2 pagesAmino SugarsNarasimha MurthyNo ratings yet
- Metabolic Pathway of Carbohydrate and GlycolysisDocument22 pagesMetabolic Pathway of Carbohydrate and GlycolysisDarshansinh MahidaNo ratings yet
- Vitamins ReviewDocument105 pagesVitamins Reviewjltrek123No ratings yet
- CH 19 Integration of MetabolismDocument63 pagesCH 19 Integration of Metabolismshee140802100% (1)
- Heme Metabolism PDFDocument19 pagesHeme Metabolism PDFAnonymous jW7BU44ACNo ratings yet
- Mode of Action: InsulinDocument8 pagesMode of Action: Insulinmanus7777100% (1)
- Carbohydrates SummaryDocument9 pagesCarbohydrates SummaryHarold NagunaNo ratings yet
- Case StudyDocument1 pageCase Studyapi-311718939No ratings yet
- PDH Complex and TCA CycleDocument20 pagesPDH Complex and TCA CycleDarrion LouisNo ratings yet
- Channels, Carriers, and Pumps: An Introduction to Membrane TransportFrom EverandChannels, Carriers, and Pumps: An Introduction to Membrane TransportNo ratings yet
- Anaerobic Metabolism of Carbohydrates in RBC - Lectue XXIDocument4 pagesAnaerobic Metabolism of Carbohydrates in RBC - Lectue XXISaulNo ratings yet
- FAT Soluble VitaminsDocument53 pagesFAT Soluble VitaminsFaria LatifNo ratings yet
- Uronic Acid PathwayDocument4 pagesUronic Acid PathwayAlen Arthur100% (2)
- GluconeogenesisDocument48 pagesGluconeogenesisQshyanNo ratings yet
- Glycogen MetabolismDocument23 pagesGlycogen Metabolismessa100% (1)
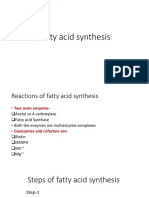
- Fatty Acid Synthesis 11.12.19Document18 pagesFatty Acid Synthesis 11.12.19Sanreet Randhawa100% (1)
- 8 Carbohydrate Metabolism PDFDocument36 pages8 Carbohydrate Metabolism PDFDayne Ocampo-SolimanNo ratings yet
- Lipoprotein MetabolismDocument23 pagesLipoprotein MetabolismDarien LiewNo ratings yet
- 2 - Lipid Metabolism Lecture For StudentsDocument68 pages2 - Lipid Metabolism Lecture For StudentshwhsgxNo ratings yet
- METABOLIC PROCESSESDocument14 pagesMETABOLIC PROCESSESNischal DhNo ratings yet
- Sphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeDocument12 pagesSphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeUzac BenuNo ratings yet
- Understanding Steroidal HormonesDocument23 pagesUnderstanding Steroidal HormonesJazab ChohanNo ratings yet
- BDS Biochemistry SyllabusDocument4 pagesBDS Biochemistry SyllabusAnandNo ratings yet
- Shelly HyperlipidemiaDocument22 pagesShelly Hyperlipidemiaale marilNo ratings yet
- S13.CHO .MetabolismDocument18 pagesS13.CHO .MetabolismGhea Jovita SinagaNo ratings yet
- Diabetes Mellitus: Overview and TreatmentsDocument36 pagesDiabetes Mellitus: Overview and TreatmentsGlenn Nadine N. Masicampo100% (1)
- Cholesterol and Lipoprotein MetabolismDocument32 pagesCholesterol and Lipoprotein MetabolismBenjamin PrabhuNo ratings yet
- Metabolism of Purine & Pyrimidine NucleotidesDocument38 pagesMetabolism of Purine & Pyrimidine NucleotidesShimmering MoonNo ratings yet
- Citric Acid Cycle Enzyme Pyruvate DehydrogenaseDocument33 pagesCitric Acid Cycle Enzyme Pyruvate Dehydrogenasesultan khabeeb100% (1)
- Lecture-5 Hormonal Regulation of Intestinal MotilityDocument4 pagesLecture-5 Hormonal Regulation of Intestinal Motilityمرتضى حسين عبدNo ratings yet
- Metabolism of Carbohydrates, Lipids, Amino Acids and its Regulation Test QuestionsDocument209 pagesMetabolism of Carbohydrates, Lipids, Amino Acids and its Regulation Test Questionsninas1112No ratings yet
- SDLS 2008 Serum Total Protein and Albumin DeterminationDocument2 pagesSDLS 2008 Serum Total Protein and Albumin DeterminationgenieqtNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDocument17 pagesM.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDr. M. Prasad Naidu100% (1)
- MCQ MembranesDocument10 pagesMCQ MembranesMarilyne RizkNo ratings yet
- Lipid Profile: by Micheal and ChristianDocument15 pagesLipid Profile: by Micheal and ChristianMichealNo ratings yet
- Carbohydrate Metabolism: Blood Haemoglobin and Respiration: - Archit SaraogiDocument6 pagesCarbohydrate Metabolism: Blood Haemoglobin and Respiration: - Archit SaraogiChictoran RukmaniNo ratings yet
- Glycogen MetabolismDocument11 pagesGlycogen MetabolismSimra ZahidNo ratings yet
- Feedback Loops: Glucose and Glucagon: Name: - Ishaan SinghDocument3 pagesFeedback Loops: Glucose and Glucagon: Name: - Ishaan SinghIshaan SinghNo ratings yet
- HW - Carbohydrate Metabolism II & Lipid MetabolismDocument2 pagesHW - Carbohydrate Metabolism II & Lipid MetabolismyanNo ratings yet
- Digestion and Absorption of Dietary LipidsDocument35 pagesDigestion and Absorption of Dietary LipidsCharmaine Luc100% (2)
- Leukocyte Structure, Function and LeukopoiesisDocument39 pagesLeukocyte Structure, Function and LeukopoiesisMarah Mazahreh100% (1)
- Benedict's TestDocument8 pagesBenedict's TestSarahNo ratings yet
- 2013 Basic Concepts of Fluid and Electrolyte TherapyDocument137 pages2013 Basic Concepts of Fluid and Electrolyte TherapySarahNo ratings yet
- Haem Introduction-Final - SDocument14 pagesHaem Introduction-Final - SSarahNo ratings yet
- Palm Kernel Oil Mill ProjectDocument8 pagesPalm Kernel Oil Mill Projectsjr141071100% (2)
- Laser LightDocument27 pagesLaser Lightdcool3784No ratings yet
- Chapter 18Document10 pagesChapter 18nehallakdawalaNo ratings yet
- Premium detergent market insights and Nirma case studyDocument32 pagesPremium detergent market insights and Nirma case studyBhavya ShahNo ratings yet
- English Form 2 Mod23042022001Document10 pagesEnglish Form 2 Mod23042022001Qiash JontezNo ratings yet
- Assay SolutionsDocument1 pageAssay SolutionsAlex RamirezNo ratings yet
- Anatomy of The PeriodontiumDocument46 pagesAnatomy of The PeriodontiumYunita Nitnot50% (2)
- Camco D Series Running ToolsDocument2 pagesCamco D Series Running Toolshosam aliNo ratings yet
- Power Con CorpDocument2 pagesPower Con Corpkhan4luvNo ratings yet
- Gulayan Project ProposalDocument2 pagesGulayan Project ProposalMarvin LagunillaNo ratings yet
- NURS 366 Exam 1 Study Guide and RubricDocument7 pagesNURS 366 Exam 1 Study Guide and RubriccmpNo ratings yet
- HANDOUT - Cell Transport Review WorksheetDocument4 pagesHANDOUT - Cell Transport Review WorksheetDenis Martinez100% (1)
- Iocl Section 1 - Process SpecficationDocument73 pagesIocl Section 1 - Process SpecficationYogi173No ratings yet
- Hedging FuturesDocument39 pagesHedging Futuresapi-3833893100% (1)
- Vegetarianism A Salvation Issue?Document7 pagesVegetarianism A Salvation Issue?ChetiweKapilaNo ratings yet
- Unit 7. The Dynamics of Ecosystems.Document12 pagesUnit 7. The Dynamics of Ecosystems.nimolesaNo ratings yet
- Choosing the Right Career and Job RequirementsDocument2 pagesChoosing the Right Career and Job RequirementsdinnahNo ratings yet
- Refrac 2Document20 pagesRefrac 2PawanNo ratings yet
- Let's Cook: Basic EnglishDocument6 pagesLet's Cook: Basic EnglishVincentNo ratings yet
- Thesis Statement 1Document4 pagesThesis Statement 1Ieka SyafiqahNo ratings yet
- Mental Health Lesson on Identity, Grief, Anxiety, OCD, Schizophrenia, and Eating DisordersDocument2 pagesMental Health Lesson on Identity, Grief, Anxiety, OCD, Schizophrenia, and Eating DisordersKaya S75% (4)
- RMO Orientation AIRMEDDocument130 pagesRMO Orientation AIRMEDqueenartemisNo ratings yet
- PN15CS1S01Document4 pagesPN15CS1S01joadNo ratings yet
- Manual de Reparacion TXV75Document16 pagesManual de Reparacion TXV75Ovh MaquinariasNo ratings yet
- NABARD Presentation On FPODocument14 pagesNABARD Presentation On FPOSomnath DasGupta71% (7)
- Onan RV GenSet Service ManualDocument136 pagesOnan RV GenSet Service ManualAlbert A Ghazaleh100% (2)
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- Letter From Springfield Mayor Sarno To License Commission Re: Late Night Hours.Document12 pagesLetter From Springfield Mayor Sarno To License Commission Re: Late Night Hours.Patrick JohnsonNo ratings yet
- Outgassing Properties of Vacuum MaterialsDocument47 pagesOutgassing Properties of Vacuum Materialsmax8086No ratings yet
- SPE/IADC-189336-MS Pioneering The First Hydraulic Fracturing in Iraq's Complex ReservoirDocument12 pagesSPE/IADC-189336-MS Pioneering The First Hydraulic Fracturing in Iraq's Complex ReservoirKarar AliNo ratings yet