You might also like
- Neonatal VentilatorAnalyzerDocument6 pagesNeonatal VentilatorAnalyzeradnanNo ratings yet
- Respiradores - Valvulas PasivasDocument7 pagesRespiradores - Valvulas Pasivasluc1902No ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- The Anesthesia Gas MachineDocument28 pagesThe Anesthesia Gas MachineBianca RotaruNo ratings yet
- Ventilator Waveforms and The Physiology of Pressure Support PDFDocument21 pagesVentilator Waveforms and The Physiology of Pressure Support PDFRoberto RamirezNo ratings yet
- GEHC Technical Report Pressure Control Ventilation Volume GuaranteedDocument4 pagesGEHC Technical Report Pressure Control Ventilation Volume GuaranteedHani Al-NassNo ratings yet
- The Basics of Respiratory Mechanics: Ventilator-Derived ParametersDocument11 pagesThe Basics of Respiratory Mechanics: Ventilator-Derived ParametersAntonioLonigroNo ratings yet
- Volume-Targeted Modes of Modern Neonatal Ventilators: How Stable Is The Delivered Tidal Volume?Document10 pagesVolume-Targeted Modes of Modern Neonatal Ventilators: How Stable Is The Delivered Tidal Volume?DawoodNo ratings yet
- Working Principles of ICU Ventilators: Dr. AnanyaDocument98 pagesWorking Principles of ICU Ventilators: Dr. AnanyaHarsono PrihadiNo ratings yet
- Early Initiation MV 2017 - DR - TrisnaDocument34 pagesEarly Initiation MV 2017 - DR - TrisnaHappy ShalalaNo ratings yet
- Ventilator Waveform AnalysisDocument76 pagesVentilator Waveform Analysischtbht100% (1)
- Mechanical Ventilation SeminarDocument82 pagesMechanical Ventilation Seminarrajan kumar90% (21)
- Advances in Mechanical Ventilation 4AH PDFDocument11 pagesAdvances in Mechanical Ventilation 4AH PDFsérgio_nakano_2No ratings yet
- New Ventilators For The ICU-usefulness of Lung Performance ReportingDocument7 pagesNew Ventilators For The ICU-usefulness of Lung Performance ReportingAnonymous gXiDxwuJsNo ratings yet
- Mechanical VentilationDocument21 pagesMechanical VentilationWang EvanNo ratings yet
- Basic Modes of Mechanical VentilationDocument16 pagesBasic Modes of Mechanical VentilationDoreli RuizNo ratings yet
- Wa0007.Document16 pagesWa0007.Ulises CasarrubiasNo ratings yet
- Breathing SystemDocument6 pagesBreathing SystemJulian LiemNo ratings yet
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical VentilationDuy ThanhNo ratings yet
- Design Principles:: Mechanical VentilatorsDocument41 pagesDesign Principles:: Mechanical VentilatorsSailu KatragaddaNo ratings yet
- Modos Basicos de VentilacionDocument16 pagesModos Basicos de Ventilacionbenitez1228No ratings yet
- A Noninvasive High Frequency Oscillation Ventilator: Achieved by Utilizing A Blower and A ValveDocument7 pagesA Noninvasive High Frequency Oscillation Ventilator: Achieved by Utilizing A Blower and A ValveSalNo ratings yet
- Principles of Icu VentilatorsDocument98 pagesPrinciples of Icu VentilatorsshivamNo ratings yet
- Ajrccm/136 4 872Document8 pagesAjrccm/136 4 872Yesica Villalba CerqueraNo ratings yet
- Mechanical Ventilation ReviewDocument5 pagesMechanical Ventilation Reviewbluecrush1No ratings yet
- Mechanical VentilatorsDocument11 pagesMechanical VentilatorsIra Katrina Bernales MendozaNo ratings yet
- Mechanical Ventilation of Adults in The Emergency Department - UpToDateDocument28 pagesMechanical Ventilation of Adults in The Emergency Department - UpToDateCarlos E. Morales AyoraNo ratings yet
- Mechanical Power and Development of VentilatorDocument9 pagesMechanical Power and Development of VentilatorJesus FrancoNo ratings yet
- Overview of Mechanical Ventilation - Critical Care Medicine - Merck Manuals Professional EditionDocument8 pagesOverview of Mechanical Ventilation - Critical Care Medicine - Merck Manuals Professional EditionParas KanwarNo ratings yet
- Alveolar Mechanics 2022Document12 pagesAlveolar Mechanics 2022Rasmia Mohamed ZakiNo ratings yet
- ASVDocument4 pagesASVKapten JancokNo ratings yet
- 43 Adaptive Support Ventilation As VDocument5 pages43 Adaptive Support Ventilation As Vnanang criztaNo ratings yet
- Mechanical Power Differs Between.8Document8 pagesMechanical Power Differs Between.8Carolina Aguilar OtáloraNo ratings yet
- Ajrccm 156 1 9609059Document5 pagesAjrccm 156 1 9609059Rezza HaryNo ratings yet
- Positive Pressure Breathing During Rest and Exercise: E.A. Den Hartog, R. HeusDocument10 pagesPositive Pressure Breathing During Rest and Exercise: E.A. Den Hartog, R. HeusAlex CastilloNo ratings yet
- Acapella Vs FlutterDocument7 pagesAcapella Vs FlutterDiana VillarroelNo ratings yet
- PRESION Positiva HistoriaDocument18 pagesPRESION Positiva HistoriaWALTER HUGO GOMEZNo ratings yet
- Mechanical VentilationDocument52 pagesMechanical VentilationSalma Omrr100% (1)
- VentilatorDocument9 pagesVentilatorSheeba StephenNo ratings yet
- Respiratory Mechanics Derived From Signals in The Ventilator CircuitDocument13 pagesRespiratory Mechanics Derived From Signals in The Ventilator CircuitJoaquin LopezNo ratings yet
- Mecánica Respiratoria: Signos en El Circuito VentilatorioDocument13 pagesMecánica Respiratoria: Signos en El Circuito VentilatoriojuliasimonassiNo ratings yet
- CHEST. Comentario MC Intyre de ExtuvaciónDocument4 pagesCHEST. Comentario MC Intyre de ExtuvaciónMarcelaNo ratings yet
- Nava VS PSVDocument9 pagesNava VS PSVangiolikkiaNo ratings yet
- Q 1Document3 pagesQ 1navdeep sokhalNo ratings yet
- Troubleshooting Mechanical VentDocument15 pagesTroubleshooting Mechanical VentIvy Jorene Roman RodriguezNo ratings yet
- Basics of Mechanical VentilationDocument63 pagesBasics of Mechanical VentilationDiem KhueNo ratings yet
- 13 COM TRADU+ç+âODocument9 pages13 COM TRADU+ç+âOEduardo SoaresNo ratings yet
- Test Bank For Pilbeams Mechanical Ventilation 5th Edition CairoDocument13 pagesTest Bank For Pilbeams Mechanical Ventilation 5th Edition Cairochowryurduq0krhNo ratings yet
- Wa0001.Document9 pagesWa0001.Shano Alfredo Cuizano MendocillaNo ratings yet
- Artigo Avaliação Do FLOW INDEX em PSVDocument9 pagesArtigo Avaliação Do FLOW INDEX em PSVVictoria MedeirosNo ratings yet
- Respiratorymechanics: Ralph GertlerDocument26 pagesRespiratorymechanics: Ralph GertlerblanquishemNo ratings yet
- Basic Principles of Mechanical Ventilation Andventilator GraphicsDocument70 pagesBasic Principles of Mechanical Ventilation Andventilator GraphicsLauraAlvarezMulettNo ratings yet
- Atm 06 19 389Document9 pagesAtm 06 19 389Carlos QuirogaNo ratings yet
- Anaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandDocument40 pagesAnaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandCrystieNo ratings yet
- Al Saady1985Document8 pagesAl Saady1985AlbertoMarteNo ratings yet
- Aerosols and the Lung: Clinical and Experimental AspectsFrom EverandAerosols and the Lung: Clinical and Experimental AspectsStewart W. ClarkeNo ratings yet
- Pulmonary Function Measurement in Noninvasive Ventilatory SupportFrom EverandPulmonary Function Measurement in Noninvasive Ventilatory SupportNo ratings yet
- A2Document8 pagesA2alvinNo ratings yet
- Antibiotik Dan Antiseptik Sal KemihDocument23 pagesAntibiotik Dan Antiseptik Sal KemihruuweelscribdNo ratings yet
- A Case Study On Chronic Renal DiseaseDocument17 pagesA Case Study On Chronic Renal Diseasematucojulio100% (1)
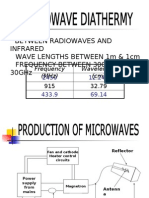
- Microwave DiathermyDocument14 pagesMicrowave Diathermybpt2No ratings yet
- PRADEEP'S - Brain TumorDocument32 pagesPRADEEP'S - Brain TumorPRADEEPNo ratings yet
- RECONSTRUCTION MAndibula 2Document62 pagesRECONSTRUCTION MAndibula 2RadianNasution100% (1)
- Nature's Pathways Dec 2014 Issue - Northeast WI EditionDocument96 pagesNature's Pathways Dec 2014 Issue - Northeast WI EditionNature's PathwaysNo ratings yet
- Ischial Bursa InjectionDocument2 pagesIschial Bursa InjectionPirthi MannNo ratings yet
- Tubing Misconnections Self Assessment For Healthcare FacilitiesDocument38 pagesTubing Misconnections Self Assessment For Healthcare FacilitiesAle Gastelum100% (1)
- Making A Reaction StatementDocument6 pagesMaking A Reaction StatementKharisma AnastasisNo ratings yet
- Case StudyDocument9 pagesCase StudyHenriettaNo ratings yet
- TheraplayDocument2 pagesTheraplayppNo ratings yet
- Use of Sedation in Palliative CareDocument13 pagesUse of Sedation in Palliative Careuriel_rojas_41No ratings yet
- NCP SepsisDocument6 pagesNCP SepsisgopscharanNo ratings yet
- Tackling DepressionDocument3 pagesTackling DepressionAndrew KennedyNo ratings yet
- Admistration of Controlled Narcotic and Controlled Non-Narcotic MedicationsDocument37 pagesAdmistration of Controlled Narcotic and Controlled Non-Narcotic MedicationsKrezielDulosEscobarNo ratings yet
- Hyper Bilirubin Emi ADocument36 pagesHyper Bilirubin Emi ASai Krishna MaddiralaNo ratings yet
- Health History QuestionnaireDocument3 pagesHealth History QuestionnairejlaferriereNo ratings yet
- Cardiovascular Medications NCLEX Practice QuizDocument8 pagesCardiovascular Medications NCLEX Practice QuizAngie MandeoyaNo ratings yet
- Chapter 60 - Insulin, Oral Hypoglycaemic Agents, and The Pharmacology of The Endocrine PancreasDocument17 pagesChapter 60 - Insulin, Oral Hypoglycaemic Agents, and The Pharmacology of The Endocrine PancreasGiliana P. García AcevedoNo ratings yet
- Improving Outcomes For Breast Cancer SurvivorsDocument280 pagesImproving Outcomes For Breast Cancer SurvivorsHồ Q. ThuậnNo ratings yet
- Oxygen TransportDocument8 pagesOxygen Transportmekar retnoningsihNo ratings yet
- CabgDocument12 pagesCabgShreeja Sajit100% (1)
- Interpretation of Stress TestsDocument26 pagesInterpretation of Stress TestsHashini VjkmrNo ratings yet
- Electroson & Electro StimulationDocument4 pagesElectroson & Electro StimulationKumar Aditya100% (2)
- The Effect of Cervical Preflaring Using Different Rotary Nickel-Titanium Systems On The Accuracy of Apical File Size DeterminationDocument4 pagesThe Effect of Cervical Preflaring Using Different Rotary Nickel-Titanium Systems On The Accuracy of Apical File Size DeterminationDrJagdish MakadiaNo ratings yet
- Arterial Puncture and CannulationDocument19 pagesArterial Puncture and CannulationAzizah Rahawarin100% (1)
- Rituximab Protocol PDFDocument13 pagesRituximab Protocol PDFSenarathKuleeshaKodisinghe100% (1)
- Psyche A AkDocument21 pagesPsyche A AkSamuel John SaludezNo ratings yet
- Lyophilized Injectables Report ProspectusDocument6 pagesLyophilized Injectables Report ProspectusgregstoneNo ratings yet