You might also like
- Diagnostic AlgorithmDocument7 pagesDiagnostic AlgorithmindahNo ratings yet
- Jurnal THTDocument3 pagesJurnal THTValentina AdindaNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- Ulnar Acces 2006Document10 pagesUlnar Acces 2006Rodrigo MartinNo ratings yet
- 2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceDocument7 pages2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceAryfKurniawanNo ratings yet
- Ecocardiografia Monitoreo Hemodinamico en Critico..Document12 pagesEcocardiografia Monitoreo Hemodinamico en Critico..cositaamorNo ratings yet
- J Jacc 2021 08 061Document11 pagesJ Jacc 2021 08 061Dhessy SusantoNo ratings yet
- Articulo 1Document8 pagesArticulo 1Julio Cosme CastorenaNo ratings yet
- Zheng 2016Document6 pagesZheng 2016Arindya RezekiNo ratings yet
- Before and After PTCADocument8 pagesBefore and After PTCAAstrid Karina PutriNo ratings yet
- Cardiac ValveDocument9 pagesCardiac Valveikbal rambalinoNo ratings yet
- Complications of Arteriovenous Fistula For Haemodialysis AccessDocument6 pagesComplications of Arteriovenous Fistula For Haemodialysis AccessAkiko Syawalidhany TahirNo ratings yet
- Comparison of Open and Laproscopic Live Donor NephrectomyDocument7 pagesComparison of Open and Laproscopic Live Donor NephrectomyEhab Omar El HalawanyNo ratings yet
- J Jacc 2012 10 036Document6 pagesJ Jacc 2012 10 036Ertan ALNo ratings yet
- 62 2020 Article 898Document7 pages62 2020 Article 898sinamirjaniNo ratings yet
- Early Follow-Up and Treatment Recommendations For Isolated Calf Deep Venous ThrombosisDocument5 pagesEarly Follow-Up and Treatment Recommendations For Isolated Calf Deep Venous ThrombosisDr. Aditya ShindeNo ratings yet
- ' Premio Publicación Indexada 2Document7 pages' Premio Publicación Indexada 2Francisco Álvarez MarcosNo ratings yet
- Radial Versus Femoral Approach For Percutaneous Coronary Diagnostic and Interventional ProceduresDocument8 pagesRadial Versus Femoral Approach For Percutaneous Coronary Diagnostic and Interventional ProceduresYashinta MaharaniNo ratings yet
- 2020 - Early Screening For Aortic Dissection With Point-Of-Care Ultrasound by Emergency PhysiciansDocument7 pages2020 - Early Screening For Aortic Dissection With Point-Of-Care Ultrasound by Emergency PhysiciansMartha Isabel BurgosNo ratings yet
- Risk Model DialysiddssssDocument7 pagesRisk Model DialysiddssssDumitru GrozaNo ratings yet
- Perioperative Hemodynamic MonitoringDocument9 pagesPerioperative Hemodynamic MonitoringjayezmenonNo ratings yet
- A-Line Complication PDFDocument8 pagesA-Line Complication PDFaeagesNo ratings yet
- 10 1159@000510402Document8 pages10 1159@000510402Guillermo Chacon AcevedoNo ratings yet
- ESC Hot Line: European Heart Journal (2015) 36, 3359-3367 Doi:10.1093/eurheartj/ehv444Document9 pagesESC Hot Line: European Heart Journal (2015) 36, 3359-3367 Doi:10.1093/eurheartj/ehv444maranzazuuNo ratings yet
- Guia CIRSEDocument14 pagesGuia CIRSEjfayalaNo ratings yet
- Complicaiones de La Ventriculostomia Agosto 2011Document6 pagesComplicaiones de La Ventriculostomia Agosto 2011Felipe Anduquia GarayNo ratings yet
- Journal of Cardiothoracic and Vascular Anesthesia: Original ArticleDocument11 pagesJournal of Cardiothoracic and Vascular Anesthesia: Original ArticleRicardoNo ratings yet
- Abdominal Ultrasound Is An Unreliable Modality For The Detection of Hemoperitoneum in Patients With Pelvic FractureDocument6 pagesAbdominal Ultrasound Is An Unreliable Modality For The Detection of Hemoperitoneum in Patients With Pelvic FractureEvelyn GrandaNo ratings yet
- The Barrow Ruptured Aneurysm Trial - 6-Year ResultsDocument9 pagesThe Barrow Ruptured Aneurysm Trial - 6-Year ResultsJulieta PereyraNo ratings yet
- Annsurg00185 0122Document6 pagesAnnsurg00185 0122Fajr MuzammilNo ratings yet
- Diseccion Aortica Acguda CronicaDocument10 pagesDiseccion Aortica Acguda Cronicaarturo garciaNo ratings yet
- Thrombectomy 6 To 24 Hours After Stroke With Mismatch Between Deficit and InfarctDocument11 pagesThrombectomy 6 To 24 Hours After Stroke With Mismatch Between Deficit and InfarctMELVIN BURTONNo ratings yet
- Preoperative Electrocardiogram and Perioperative M - 2020 - Journal of CardiothoDocument7 pagesPreoperative Electrocardiogram and Perioperative M - 2020 - Journal of CardiothoStefan LaurentiuNo ratings yet
- Anesthetic Technique and Acute Kidney Injury in Endovascular Abdominal Aortic Aneurism RepairDocument7 pagesAnesthetic Technique and Acute Kidney Injury in Endovascular Abdominal Aortic Aneurism RepairDiego RodriguezNo ratings yet
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsDocument9 pagesReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobNo ratings yet
- Is Endocan a Marker for Pneumonia After SurgeryDocument6 pagesIs Endocan a Marker for Pneumonia After SurgeryThomas HussonNo ratings yet
- Eco in Cardiac Sugrery Anesthesic 1-s2.0-S1053077020305875-MainDocument11 pagesEco in Cardiac Sugrery Anesthesic 1-s2.0-S1053077020305875-MainCésar Marriaga ZárateNo ratings yet
- Article 8Document4 pagesArticle 8Kamal SaleemNo ratings yet
- Preoperative Scoring Systems Used in Retroperitoneoscopic Partial Nephrectomy For T1-T2Document15 pagesPreoperative Scoring Systems Used in Retroperitoneoscopic Partial Nephrectomy For T1-T2Fana Ștefania DucaNo ratings yet
- nihms951502Document24 pagesnihms951502Svt Mscofficial2No ratings yet
- Low Diagnostic AngiographyDocument10 pagesLow Diagnostic AngiographyMei Lisa PutriNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- Jorgensen 2019Document8 pagesJorgensen 2019Emeray EssenceNo ratings yet
- 10.1007@s00134 019 05651 9Document9 pages10.1007@s00134 019 05651 9Moisés Alberto CharajaNo ratings yet
- Performance in The Shuttle Walk Test Is Associated With Cardiopulmonary Complications After Lung ResectionsDocument10 pagesPerformance in The Shuttle Walk Test Is Associated With Cardiopulmonary Complications After Lung ResectionsAnonymous Skzf3D2HNo ratings yet
- J.jhep.2009.04.01420160516 7753 11ag9zr With Cover Page v2Document9 pagesJ.jhep.2009.04.01420160516 7753 11ag9zr With Cover Page v2amazinggraceNo ratings yet
- Ischemic Heart Disease and Diagnostic Coronary Angiographyepidemiological Data and Femoral vs. Radial Approach: A Series of 100 CasesDocument6 pagesIschemic Heart Disease and Diagnostic Coronary Angiographyepidemiological Data and Femoral vs. Radial Approach: A Series of 100 CasesIJAR JOURNALNo ratings yet
- Vascular Complications Associated With Arteriotomy Closure Devices in Patients Undergoing Percutaneous Coronary ProceduresDocument10 pagesVascular Complications Associated With Arteriotomy Closure Devices in Patients Undergoing Percutaneous Coronary ProcedurescallmelikaNo ratings yet
- Fifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDocument6 pagesFifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDavid RamirezNo ratings yet
- Costantino Et Al-2012-Academic Emergency MedicineDocument6 pagesCostantino Et Al-2012-Academic Emergency MedicineCii WaaiiNo ratings yet
- Define PCIDocument11 pagesDefine PCIJose JacobNo ratings yet
- ACFrOgAB8 Tkw2cTNZ5H661ndcneV9fi1RTn1ykvnJvumEFlHYEvSpEHtoXIvYK5jjNGQbrB35rwgjvkxfQME3bphkaekY6xwI BQlK08W3zxE2v4uvQ7YrquWEUIv3SWl0RB VNAPF1WDhLtIIeDocument6 pagesACFrOgAB8 Tkw2cTNZ5H661ndcneV9fi1RTn1ykvnJvumEFlHYEvSpEHtoXIvYK5jjNGQbrB35rwgjvkxfQME3bphkaekY6xwI BQlK08W3zxE2v4uvQ7YrquWEUIv3SWl0RB VNAPF1WDhLtIIevinicius.alvarez3No ratings yet
- Open Journal of SurgeryDocument6 pagesOpen Journal of SurgerySciresNo ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- Predicting Mortality and Morbidity of Patients Operated On For Perforated Peptic UlcersDocument5 pagesPredicting Mortality and Morbidity of Patients Operated On For Perforated Peptic UlcersbintixxNo ratings yet
- ArticolsssaDocument11 pagesArticolsssaCosmin GabrielNo ratings yet
- Blunt Traumatic Aortic Injury: Initial Experience With Endovascular RepairDocument6 pagesBlunt Traumatic Aortic Injury: Initial Experience With Endovascular RepairYahya AlmalkiNo ratings yet
- 1 s2.0 S1053077022007510 MainDocument16 pages1 s2.0 S1053077022007510 MainCristhian BastidasNo ratings yet
- 1 s2.0 S0929664617300487 MainDocument8 pages1 s2.0 S0929664617300487 MainSuryati HusinNo ratings yet
- 2021 ESC Guidelines On Cardiac Pacing andDocument94 pages2021 ESC Guidelines On Cardiac Pacing andLeo Purba100% (1)
- SAMPLE Solve Exam Type Maths P3Document10 pagesSAMPLE Solve Exam Type Maths P3Binod KumarNo ratings yet
- Arrhythmia in Cardiac SarcoidosisDocument12 pagesArrhythmia in Cardiac SarcoidosisBinod KumarNo ratings yet
- ESC Guidelines CardiomyopathiesDocument124 pagesESC Guidelines CardiomyopathiesSergio Mora CanelaNo ratings yet
- 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)Document61 pages2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)AdelaNo ratings yet
- Guias ESC para Insuficiencia Cardiaca CronicaDocument128 pagesGuias ESC para Insuficiencia Cardiaca CronicaKarla HernandezNo ratings yet
- Ehab 484Document111 pagesEhab 484aslinNo ratings yet
- MATHS PARTNER Book 5 - Sample PagesDocument10 pagesMATHS PARTNER Book 5 - Sample PagesBinod KumarNo ratings yet
- 2021 ESC/EACTS Guidelines For The Management of Valvular Heart DiseaseDocument72 pages2021 ESC/EACTS Guidelines For The Management of Valvular Heart DiseaseAdriana VladutuNo ratings yet
- ESC Arterial Hypertension 2018Document98 pagesESC Arterial Hypertension 2018ddantoniusgmailNo ratings yet
- 2020 ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseDocument80 pages2020 ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseBinod KumarNo ratings yet
- 2020 ESC Guidelines For The Management of Adult Congenital Heart DiseaseDocument84 pages2020 ESC Guidelines For The Management of Adult Congenital Heart DiseaseBinod KumarNo ratings yet
- 4 5931499803149076504 PDFDocument126 pages4 5931499803149076504 PDFCristianAltunaSotomayorNo ratings yet
- Ehaa575 PDFDocument79 pagesEhaa575 PDFPatricia MarceloNo ratings yet
- Ehz 467Document66 pagesEhz 467Cosmina Alina MoscuNo ratings yet
- Ghid Dislipidemie 2019Document78 pagesGhid Dislipidemie 2019Ema PetrescuNo ratings yet
- 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)Document61 pages2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)AdelaNo ratings yet
- ESC Guidelines Hypertrophic CardiomyopathyDocument55 pagesESC Guidelines Hypertrophic CardiomyopathyFlavian ȚuțuianuNo ratings yet
- 2018 ESC-EACTS Guidelines On Myocardial RevascularizationDocument96 pages2018 ESC-EACTS Guidelines On Myocardial RevascularizationTony Miguel Saba SabaNo ratings yet
- Syncope Guideline ESC 2018Document69 pagesSyncope Guideline ESC 2018ddantoniusgmailNo ratings yet
- Guidlines Gagal Jantung Dengan Kehamilan 2018 EscDocument84 pagesGuidlines Gagal Jantung Dengan Kehamilan 2018 EscanakratukuberasNo ratings yet
- Pericardial DiseaseDocument44 pagesPericardial DiseaseAlin AmaliyahNo ratings yet
- ESC Guidelines on Diagnosis and Treatment of Aortic DiseasesDocument62 pagesESC Guidelines on Diagnosis and Treatment of Aortic DiseasesDidi SNo ratings yet
- 2018 AHA Guidelines For Management of Blood CholesterolDocument66 pages2018 AHA Guidelines For Management of Blood CholesterolsarumaxNo ratings yet
- Ehv319 PDFDocument54 pagesEhv319 PDFPrisela Zharaswati SagaNo ratings yet
- J Jacc 2020 11 0907Document39 pagesJ Jacc 2020 11 0907Mister SimpleNo ratings yet
- 2020 Acute Chest Pain in The Emergency Department 20222Document36 pages2020 Acute Chest Pain in The Emergency Department 20222Binod KumarNo ratings yet
- 2021 AC and APT Decision Pathway For AF VTE and PCI ASCVDDocument30 pages2021 AC and APT Decision Pathway For AF VTE and PCI ASCVDPeter Albeiro Falla CortesNo ratings yet
- Child Health COURSE PLAN M.SC 2 YEARDocument49 pagesChild Health COURSE PLAN M.SC 2 YEARSanthosh.S.UNo ratings yet
- The Ultimate Guide To Breathwork 2024Document8 pagesThe Ultimate Guide To Breathwork 2024lucicdNo ratings yet
- Nuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaDocument124 pagesNuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaWhite HeartNo ratings yet
- Msds Sodium HypochloriteDocument9 pagesMsds Sodium Hypochloritehinur awaNo ratings yet
- Laporan Jaga Perina Selasa Malam EditDocument15 pagesLaporan Jaga Perina Selasa Malam EditmuhammadrikiNo ratings yet
- SAS 6 - Abapo, Aquea B.Document5 pagesSAS 6 - Abapo, Aquea B.Aquea Bernardo AbapoNo ratings yet
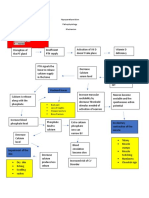
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- T10 FinDocument12 pagesT10 FinalejandraNo ratings yet
- Gen 2 - Unit Test - 25.2.2022Document8 pagesGen 2 - Unit Test - 25.2.2022Phương Thảo NguyễnNo ratings yet
- NCP For Older Adults With Sleep DisturbanceDocument17 pagesNCP For Older Adults With Sleep DisturbanceAlienda Puspita PutriNo ratings yet
- Clinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and PapacarieDocument8 pagesClinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and PapacarieVianney Guadalupe González ElizaldeNo ratings yet
- Understand the Difference Between Omega-3 EPA and DHADocument7 pagesUnderstand the Difference Between Omega-3 EPA and DHASutanto TanakaNo ratings yet
- NP1 - ToprankDocument16 pagesNP1 - ToprankAllaiza Cristille100% (1)
- PASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceDocument2 pagesPASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceJhigo Villar Franco PascualNo ratings yet
- Sina Cheffer PDFDocument7 pagesSina Cheffer PDFCaroline RobisonNo ratings yet
- B1621 - V - Lisdexamfetamine For Patients Within Adult ServicesDocument27 pagesB1621 - V - Lisdexamfetamine For Patients Within Adult Servicesdimitros kristianopoulosNo ratings yet
- Reproductive ToxicologyDocument31 pagesReproductive ToxicologyfianceeleeNo ratings yet
- Hydrotherapy Principles & TechniquesDocument75 pagesHydrotherapy Principles & TechniquesSANLAPAN SAHOONo ratings yet
- What Is Nano Silver - Nano Silver PDFDocument2 pagesWhat Is Nano Silver - Nano Silver PDFvijuNo ratings yet
- List of International Days and WeeksDocument10 pagesList of International Days and WeeksSatram RoopaniNo ratings yet
- Learning Guide 18: Animal Health Care Service NTQF Level-IVDocument105 pagesLearning Guide 18: Animal Health Care Service NTQF Level-IVRafez JoneNo ratings yet
- Research Article Smilacina Japonica A. Gray: Antifungal Activity of Crude Extract From The Rhizome and Root ofDocument10 pagesResearch Article Smilacina Japonica A. Gray: Antifungal Activity of Crude Extract From The Rhizome and Root ofJolianna Andrea Beatrice BallezaNo ratings yet
- Stree Rog 4Document11 pagesStree Rog 4Sambamurthi Punninnair NarayanNo ratings yet
- Experimental and Correlational Studies of The Fear of Death: Direct Inethdds. The Earliest TechniqueDocument10 pagesExperimental and Correlational Studies of The Fear of Death: Direct Inethdds. The Earliest TechniqueDana PascuNo ratings yet
- DVLA Null NewDocument1 pageDVLA Null NewTaniaNo ratings yet
- Comprehensive Geriatric Assessment FormDocument13 pagesComprehensive Geriatric Assessment FormJojo Binay0% (1)
- Incucyte Nuclight Lentivirus ReagentsDocument6 pagesIncucyte Nuclight Lentivirus Reagents李琇琴No ratings yet
- Treatment of Acute BronchitisDocument3 pagesTreatment of Acute BronchitisjokosudibyoNo ratings yet
- OVPR FY20Q1 Proposal List PDFDocument45 pagesOVPR FY20Q1 Proposal List PDFtsuregiNo ratings yet
- Anaesthesia For Adenotonsillectomy An UpdateDocument7 pagesAnaesthesia For Adenotonsillectomy An UpdateSrihari JanakiNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)