You might also like
- The Tale of Sweet-Friend and Ali-NurDocument2 pagesThe Tale of Sweet-Friend and Ali-NurJomarie Siason Sumagpao100% (1)
- Immune Disorders, Vaccines, Covid-19 and Drug Reactions DiscussedDocument73 pagesImmune Disorders, Vaccines, Covid-19 and Drug Reactions DiscussedErum JanNo ratings yet
- Low-Level AutoimmunityDocument13 pagesLow-Level AutoimmunityBeeBee SethNo ratings yet
- Connective Tissue Disease LectureDocument99 pagesConnective Tissue Disease Lectureconfuzzledfreak100% (1)
- Diseases of Immune System Part 2Document47 pagesDiseases of Immune System Part 2KundaNo ratings yet
- Rev Med Clin Condes Endocrine Autoimmune SyndromesDocument6 pagesRev Med Clin Condes Endocrine Autoimmune SyndromesFabiola Javiera Reales NúñezNo ratings yet
- Chapter 20 Tolerance and Auto Immune DiseaseDocument32 pagesChapter 20 Tolerance and Auto Immune Diseasehusseinabdullahahmad99No ratings yet
- Immunopathology Lec 4Document11 pagesImmunopathology Lec 4zaharNo ratings yet
- Копия Autoimmunity-and-Autoimmune-disordersDocument38 pagesКопия Autoimmunity-and-Autoimmune-disordersManav VyasNo ratings yet
- Autoimunitas: Ika NurzijahDocument43 pagesAutoimunitas: Ika NurzijahDimas SuryapratamaNo ratings yet
- Autoimmune-Disorders PDF Divya Mam PracticalDocument44 pagesAutoimmune-Disorders PDF Divya Mam Practicaltariqahmeda34No ratings yet
- Thyroid Autoimmune DiseasesDocument21 pagesThyroid Autoimmune Diseasesmicheal1960No ratings yet
- Kuby5 20 AutoImmunity PDFDocument19 pagesKuby5 20 AutoImmunity PDFASDASDDD2No ratings yet
- Immunity, Autoimmunity - QsDocument5 pagesImmunity, Autoimmunity - QsMaedehNo ratings yet
- Presentation Auto 2Document33 pagesPresentation Auto 2mlllNo ratings yet
- Auto ImmunityDocument44 pagesAuto ImmunityA. PathakNo ratings yet
- AutoimmunDocument17 pagesAutoimmunIka Superti DaruningrumNo ratings yet
- Auto ImmunityDocument38 pagesAuto ImmunityMau studioNo ratings yet
- Understanding Autoimmune Disease Cells and ImmunityDocument38 pagesUnderstanding Autoimmune Disease Cells and ImmunityGustiandari FidhyaNo ratings yet
- Autoimmunity: 1 Semester DMLTDocument11 pagesAutoimmunity: 1 Semester DMLTTepfi TepsNo ratings yet
- Sle DevDocument10 pagesSle DevDev VithlaniNo ratings yet
- Autoimmune Disorders - AgungDocument40 pagesAutoimmune Disorders - AgungalgutNo ratings yet
- Hypersensitivity Diseases: Autoimmune Disease-1Document27 pagesHypersensitivity Diseases: Autoimmune Disease-1fakhirNo ratings yet
- Autoimun MekanismeDocument22 pagesAutoimun MekanismeMeity ElvinaNo ratings yet
- Clinical Immunology Lecture on Autoimmunity and Rheumatoid ArthritisDocument33 pagesClinical Immunology Lecture on Autoimmunity and Rheumatoid ArthritisAli AlhamdaniNo ratings yet
- Document-22Document3 pagesDocument-22nicolasdanica018No ratings yet
- Autoimmune DisordersDocument49 pagesAutoimmune DisordersAyesha RasheedNo ratings yet
- Week 16 - Autoimmune DiseasesDocument25 pagesWeek 16 - Autoimmune DiseasesKyle CollladoNo ratings yet
- Autoimmunity and Autoimmune DisordersDocument46 pagesAutoimmunity and Autoimmune DisordersJennifer EvansNo ratings yet
- Autoimmune DiseasesDocument4 pagesAutoimmune Diseasesnizam syedNo ratings yet
- Amity Institute of BiotechnologyDocument44 pagesAmity Institute of BiotechnologyMilind SagarNo ratings yet
- AutoimmunityDocument40 pagesAutoimmunityKarl RobleNo ratings yet
- AutoimmunityDocument29 pagesAutoimmunitywissam salimNo ratings yet
- Principle and Classification of Auto-Immune DiseasesDocument42 pagesPrinciple and Classification of Auto-Immune Diseasesmanuel.mayin33No ratings yet
- Autoimmune DiseasesDocument70 pagesAutoimmune DiseasesAdebisi OluwatomiwaNo ratings yet
- Immunology Unit 1Document6 pagesImmunology Unit 1Morrison GeorgeNo ratings yet
- Autoimmunity Mechanisms and DiseasesDocument22 pagesAutoimmunity Mechanisms and Diseasesrido rahmad saputraNo ratings yet
- DR WikipediaDocument15 pagesDR Wikipediamutu pkmkromenganNo ratings yet
- 10 AutoimmunityDocument11 pages10 AutoimmunityangelNo ratings yet
- Autoimmune Disorders - MicrobiologyDocument6 pagesAutoimmune Disorders - MicrobiologyAll in oneNo ratings yet
- Autoimmune Disorders: DR Muhammad ZUBAIR Consultant Chemical PathologistDocument52 pagesAutoimmune Disorders: DR Muhammad ZUBAIR Consultant Chemical PathologistZubair YousafNo ratings yet
- 2-Autoimmune DiseasesDocument29 pages2-Autoimmune DiseasessoniaNo ratings yet
- Systemic Lupus Erythematosus, Rheumatoid ArthritisDocument28 pagesSystemic Lupus Erythematosus, Rheumatoid ArthritisSalomeSibashviliNo ratings yet
- Auto Immune DiseasesDocument18 pagesAuto Immune DiseasesNareshNo ratings yet
- Autoimmunity: Jamie SturgillDocument43 pagesAutoimmunity: Jamie SturgillSeptiyani Monalisa AndriNo ratings yet
- Autoimmunity: Dr.C.Meenakshisundaram.,MDDocument66 pagesAutoimmunity: Dr.C.Meenakshisundaram.,MDChockalingam Meenakshisundaram100% (1)
- Understanding Autoimmune DiseasesDocument28 pagesUnderstanding Autoimmune Diseasesrona angelin purbaNo ratings yet
- Chapter 6 - Diseases of The Immune SystemDocument3 pagesChapter 6 - Diseases of The Immune SystemTurinawe Bin ByensiNo ratings yet
- Rheumatic Fever (RF) :: Volgograd State Medical University Faculty of DentistryDocument15 pagesRheumatic Fever (RF) :: Volgograd State Medical University Faculty of DentistryAya RagabNo ratings yet
- Diseases of ImmunityDocument11 pagesDiseases of ImmunityRAFAELLA SALVE MARIE GAETOSNo ratings yet
- Autoimmune Disorders: CausesDocument11 pagesAutoimmune Disorders: CausesJenalyn Pilapil SumaelNo ratings yet
- IMS - Immunomodulation & ImmunodeficienciesDocument3 pagesIMS - Immunomodulation & ImmunodeficienciesJeanne RodiñoNo ratings yet
- Immunlogical DisorderDocument36 pagesImmunlogical DisorderSameen NasirNo ratings yet
- Auto Immune Disorder 2016Document38 pagesAuto Immune Disorder 2016vistaNo ratings yet
- Graves' Disease and The Manifestations of Thyrotoxicosis: Leslie J de Groot, MDDocument75 pagesGraves' Disease and The Manifestations of Thyrotoxicosis: Leslie J de Groot, MDSalim JufriNo ratings yet
- Disorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedDocument25 pagesDisorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedFrances FranciscoNo ratings yet
- Autoimmune Diseases of the Immune SystemDocument73 pagesAutoimmune Diseases of the Immune SystemVisca ZerlindaNo ratings yet
- Human Autoimmune Diseases: Disease Autoantigen Symptoms ExtentDocument6 pagesHuman Autoimmune Diseases: Disease Autoantigen Symptoms ExtentsauravsarkarNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 14: ImmunologyFrom EverandComplementary and Alternative Medical Lab Testing Part 14: ImmunologyNo ratings yet
- Immunointervention in Autoimmune Diseases: Papers Based on an International Meeting in Paris, France, in June 1988From EverandImmunointervention in Autoimmune Diseases: Papers Based on an International Meeting in Paris, France, in June 1988J. F. BachNo ratings yet
- L2The Chemical Basis of Life PDFDocument43 pagesL2The Chemical Basis of Life PDFVince Martin ManaigNo ratings yet
- Tissues Part 2 of 4Document13 pagesTissues Part 2 of 4Vince Martin ManaigNo ratings yet
- Cell Structure and FunctionsDocument45 pagesCell Structure and FunctionsVince Martin ManaigNo ratings yet
- L1The Human OrganismDocument44 pagesL1The Human OrganismVince Martin ManaigNo ratings yet
- CELL STRUCTURES AND FUNCTIONSDocument27 pagesCELL STRUCTURES AND FUNCTIONSVince Martin ManaigNo ratings yet
- Anaphy Chapter 1 The Human OrganismDocument29 pagesAnaphy Chapter 1 The Human OrganismVince Martin ManaigNo ratings yet
- Topic 7 - Anemia 2Document33 pagesTopic 7 - Anemia 2Vince Martin ManaigNo ratings yet
- Anemias of Abnormal Globin Development: ThalassemiasDocument25 pagesAnemias of Abnormal Globin Development: ThalassemiasVince Martin ManaigNo ratings yet
- Topic 9 - Anemia 4Document27 pagesTopic 9 - Anemia 4Vince Martin ManaigNo ratings yet
- Iron Deficiency Anemia DiagnosisDocument62 pagesIron Deficiency Anemia DiagnosisVince Martin ManaigNo ratings yet
- Complement (Yt)Document7 pagesComplement (Yt)Vince Martin ManaigNo ratings yet
- Topic 6 - Anemia 1Document24 pagesTopic 6 - Anemia 1Vince Martin ManaigNo ratings yet
- National Geographic USA - 01 2019Document145 pagesNational Geographic USA - 01 2019Minh ThuNo ratings yet
- 2013 SmartBUS Home Automation Product Catalogue English v.1.0Document108 pages2013 SmartBUS Home Automation Product Catalogue English v.1.0Smart-G4100% (3)
- Dell in India Targeting SMB Markets - The Differentiation Strategy PDFDocument16 pagesDell in India Targeting SMB Markets - The Differentiation Strategy PDFJatinNo ratings yet
- Baltimore County IG ReportDocument35 pagesBaltimore County IG ReportChris BerinatoNo ratings yet
- Unit 2 - LISDocument24 pagesUnit 2 - LISThục Anh NguyễnNo ratings yet
- 1967 Painting Israeli VallejoDocument1 page1967 Painting Israeli VallejoMiloš CiniburkNo ratings yet
- 41 Programmer Isp RT809F PDFDocument3 pages41 Programmer Isp RT809F PDFArunasalam ShanmugamNo ratings yet
- Dictation TechniquesDocument12 pagesDictation TechniquesMuhamad IbrohimNo ratings yet
- You Write, It Types!: Quick Start GuideDocument21 pagesYou Write, It Types!: Quick Start Guidejean michelNo ratings yet
- Review of Esu Yoruba God Power and The IDocument7 pagesReview of Esu Yoruba God Power and The IBoris MilovicNo ratings yet
- Use VCDS with PC lacking InternetDocument1 pageUse VCDS with PC lacking Internetvali_nedeleaNo ratings yet
- Scan Sep 2, 2020Document1 pageScan Sep 2, 2020Taresh MittalNo ratings yet
- 09 Egyptian Architecture PDFDocument107 pages09 Egyptian Architecture PDFIra PecsonNo ratings yet
- 2010 Christian Religious Education Past Paper - 1Document1 page2010 Christian Religious Education Past Paper - 1lixus mwangiNo ratings yet
- Our Lady of Consolation Orchestra InstrumentsDocument2 pagesOur Lady of Consolation Orchestra InstrumentsCelestian Valensario PaderangaNo ratings yet
- Types of Companies Classified by Incorporation, Membership, Liability and ControlDocument11 pagesTypes of Companies Classified by Incorporation, Membership, Liability and ControlPrasad BulbuleNo ratings yet
- Effect of Acids and Bases on Fibre Tensile StrengthDocument15 pagesEffect of Acids and Bases on Fibre Tensile StrengthVIKASH SHARMA100% (1)
- IN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Document4 pagesIN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Mary Claire ComalaNo ratings yet
- Buckley V UkDocument12 pagesBuckley V UkShriya ChandankarNo ratings yet
- Lesson Plan-MethodsDocument6 pagesLesson Plan-Methodsapi-272643370No ratings yet
- Surveying 2 Practical 3Document15 pagesSurveying 2 Practical 3Huzefa AliNo ratings yet
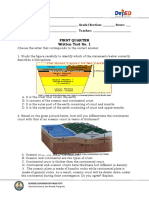
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- Sivas Doon LecturesDocument284 pagesSivas Doon LectureskartikscribdNo ratings yet
- Sealed with a Kiss Hit Song from 1962Document1 pageSealed with a Kiss Hit Song from 1962mrmarcoguimaNo ratings yet
- Mora Solvendi (Delay of The Debtor)Document11 pagesMora Solvendi (Delay of The Debtor)John Paul100% (1)
- Sec 4 RA 6713 & Sec 3 RA 3019 OutlineDocument4 pagesSec 4 RA 6713 & Sec 3 RA 3019 OutlineAivan Charles TorresNo ratings yet
- Flex Id Driver Install InstructionsDocument24 pagesFlex Id Driver Install InstructionskingdiamondNo ratings yet
- Module IV StaffingDocument3 pagesModule IV Staffingyang_19250% (1)
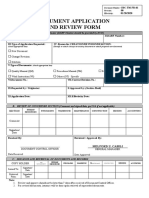
- Document Application and Review FormDocument1 pageDocument Application and Review FormJonnel CatadmanNo ratings yet