You might also like
- Informative Speech OutlineDocument4 pagesInformative Speech Outlineapi-242586808100% (2)
- Raising Siblings Without RivalryDocument32 pagesRaising Siblings Without RivalryMoveshade74100% (1)
- CH 2Document4 pagesCH 2api-479483832No ratings yet
- Nutri SiDocument153 pagesNutri SiEveLyn PRadanaNo ratings yet
- Teen Pregnancy PresentationDocument12 pagesTeen Pregnancy Presentationapi-501254101100% (1)
- In-Hospital Kangaroo Adaptation and Discharge PoliciesDocument51 pagesIn-Hospital Kangaroo Adaptation and Discharge PoliciesMelina Defita SariNo ratings yet
- Review of Literature Kangaroo Mother CareDocument5 pagesReview of Literature Kangaroo Mother Caregw1m2qtf100% (1)
- 12th MDCON Madam MiniDocument20 pages12th MDCON Madam MiniMinnie PamutanNo ratings yet
- Module6 Eng PDFDocument29 pagesModule6 Eng PDFyasodha maharajNo ratings yet
- Clinical Learning Model in Professional Midwifery Education ProgramDocument59 pagesClinical Learning Model in Professional Midwifery Education ProgramHana NazeefaNo ratings yet
- Mannel2006 FteDocument9 pagesMannel2006 FteShasa Aulia MadjidNo ratings yet
- SR MC EducationDocument8 pagesSR MC Educationimas KurniawatyNo ratings yet
- Handbook of Specialist Training in Paediatric Nephrology in MalaysiaDocument57 pagesHandbook of Specialist Training in Paediatric Nephrology in MalaysiaPICU HTJSNo ratings yet
- Review of Literature Related To Kangaroo Mother CareDocument8 pagesReview of Literature Related To Kangaroo Mother Carec5swkkcnNo ratings yet
- KMC Module: Learn Kangaroo Mother Care SkillsDocument11 pagesKMC Module: Learn Kangaroo Mother Care SkillsKristina BurburanNo ratings yet
- Literature Review Kangaroo Mother CareDocument7 pagesLiterature Review Kangaroo Mother CareafdtuwxrbNo ratings yet
- Framework For Maternal and Child Health NursingDocument7 pagesFramework For Maternal and Child Health NursingBeBs jai SelasorNo ratings yet
- Integrating Breastfeeding in University CurriculaDocument124 pagesIntegrating Breastfeeding in University CurriculaMuhammad Farooq SaeedNo ratings yet
- Helping Mothers Survive Bleeding After Birth 0Document2 pagesHelping Mothers Survive Bleeding After Birth 0Daniel RamalhoNo ratings yet
- Kangaroo Mother CareDocument9 pagesKangaroo Mother CareVikas NehraNo ratings yet
- The Midwifery-Body of Knowledge: Materi Pertemuan Ke-2 Dr. Yanti SST., M.KebDocument36 pagesThe Midwifery-Body of Knowledge: Materi Pertemuan Ke-2 Dr. Yanti SST., M.KebAndwi AsriNo ratings yet
- RCN TrainingDocument64 pagesRCN TrainingkaidNo ratings yet
- NBNS3224 Learning KitDocument54 pagesNBNS3224 Learning KitShaa ShaamalaahNo ratings yet
- Cmo MidwiferyDocument14 pagesCmo MidwiferyArleneDelosSantos100% (1)
- Bab I Pendahuluan: A. Latar BelakangDocument7 pagesBab I Pendahuluan: A. Latar BelakanglinaNo ratings yet
- Diploma in Midwifery CurriculumDocument57 pagesDiploma in Midwifery CurriculumShyamal MajumderNo ratings yet
- Assess The Knowledge Among Staff NursesDocument9 pagesAssess The Knowledge Among Staff Nursesمالك مناصرةNo ratings yet
- Tagoloan Community College Midwifery Program OutcomesDocument8 pagesTagoloan Community College Midwifery Program OutcomesRam AugustNo ratings yet
- Kangaroo Mother Care Kenya GuidelinesDocument48 pagesKangaroo Mother Care Kenya Guidelinesokwadha simionNo ratings yet
- Midwifery Cmo PDFDocument74 pagesMidwifery Cmo PDFgilissa50% (2)
- Resource Unit On Nutritional Needs of A NewbornDocument16 pagesResource Unit On Nutritional Needs of A NewbornKrishna Faith P. DelaraNo ratings yet
- 1705406887-158Document13 pages1705406887-158melpayangsNo ratings yet
- Cmo 33 Series 2007-MidwiferyDocument74 pagesCmo 33 Series 2007-MidwiferyJohnard B. RebatoNo ratings yet
- Improving Kangaroo Mother CareDocument6 pagesImproving Kangaroo Mother CareSuryadi LimardiNo ratings yet
- 1 s2.0 S0884217521001738 MainDocument2 pages1 s2.0 S0884217521001738 Mainmia.dubon17213No ratings yet
- Educational Perspectives: Educational Strategies To Improve Outcomes From Neonatal ResuscitationDocument13 pagesEducational Perspectives: Educational Strategies To Improve Outcomes From Neonatal ResuscitationDian RahmawatiNo ratings yet
- 479 Professional DevelopmentDocument13 pages479 Professional Developmentapi-708880014No ratings yet
- Kangaroo Mother Care Brief FinalDocument2 pagesKangaroo Mother Care Brief FinalSirju RanaNo ratings yet
- Kangaroo Mother Care: Benefits of KMC: What Is The Evidence?Document12 pagesKangaroo Mother Care: Benefits of KMC: What Is The Evidence?sandeepv08No ratings yet
- Appendix 4M - Paediatric Emergency MedicineDocument21 pagesAppendix 4M - Paediatric Emergency MedicineEssam HassanNo ratings yet
- Cmo 33-2007Document74 pagesCmo 33-2007Dino Pring50% (2)
- 1 SMDocument4 pages1 SMHasanNo ratings yet
- Review of Literature On Knowledge of Kangaroo Mother CareDocument4 pagesReview of Literature On Knowledge of Kangaroo Mother CarexbvtmpwgfNo ratings yet
- RCH Lesson Plan on Reproductive and Child Health ServicesDocument5 pagesRCH Lesson Plan on Reproductive and Child Health ServicesSanthu Su83% (6)
- CMO No.33 s2007Document92 pagesCMO No.33 s2007queenfaustineeNo ratings yet
- OBGYN Skills Lab GuideDocument91 pagesOBGYN Skills Lab GuideSeydel DucosquelNo ratings yet
- The Kangaroo NutritionDocument55 pagesThe Kangaroo NutritionMelina Defita SariNo ratings yet
- 1 KMC History, Concept and DevelopmentDocument52 pages1 KMC History, Concept and DevelopmentteabagmanNo ratings yet
- Curriculum of Diploma in MidwiferyDocument45 pagesCurriculum of Diploma in MidwiferycaperobeeNo ratings yet
- DC10637 APP Paediatric Emergency Medicine Syllabus 75637504Document22 pagesDC10637 APP Paediatric Emergency Medicine Syllabus 75637504Essam HassanNo ratings yet
- Framework for competency-based obstetrics and gynecology educationDocument10 pagesFramework for competency-based obstetrics and gynecology educationateebNo ratings yet
- Government College of Nursing Kalburgi, Gims, KalaburgiDocument8 pagesGovernment College of Nursing Kalburgi, Gims, KalaburgiAshok TawadeNo ratings yet
- Icm Competencies English Document Final Oct 2018Document21 pagesIcm Competencies English Document Final Oct 2018ISHITA VYASNo ratings yet
- BSC in Neonatal NursingDocument14 pagesBSC in Neonatal NursingsmsmdsdsffNo ratings yet
- Appendix 4O Paediatric Neurology PDF 86370742Document21 pagesAppendix 4O Paediatric Neurology PDF 86370742Aditya GhoshNo ratings yet
- Bfci Hcws HandoutDocument68 pagesBfci Hcws HandoutBrianBeauttahNo ratings yet
- Chapter 15 - RESOURCE UNITDocument109 pagesChapter 15 - RESOURCE UNITKrishna Faith P. DelaraNo ratings yet
- 2011 10 10 MWF Background To Education Pack V 4Document38 pages2011 10 10 MWF Background To Education Pack V 4Jonas Marvin AnaqueNo ratings yet
- Rolling Out of Kangaroo Mother Care in Secondary.11Document7 pagesRolling Out of Kangaroo Mother Care in Secondary.11sunny kumarNo ratings yet
- Next Generation NCLEX-PN Prep 2023-2024: Practice Test + Proven StrategiesFrom EverandNext Generation NCLEX-PN Prep 2023-2024: Practice Test + Proven StrategiesNo ratings yet
- A Handbook for Student Nurses, 2015–16 edition: Introducing Key Issues Relevant to PracticeFrom EverandA Handbook for Student Nurses, 2015–16 edition: Introducing Key Issues Relevant to PracticeRating: 5 out of 5 stars5/5 (2)
- NCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsFrom EverandNCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsNo ratings yet
- Penyuluhan Prematur DayDocument50 pagesPenyuluhan Prematur DayMelina Defita SariNo ratings yet
- Test Infanib PhotosDocument26 pagesTest Infanib PhotosMelina Defita SariNo ratings yet
- Neurological assessment at 40 weeksDocument11 pagesNeurological assessment at 40 weeksMelina Defita SariNo ratings yet
- Exit of The Neonatal Unit and Ambulatory Follow Up of High RiskDocument176 pagesExit of The Neonatal Unit and Ambulatory Follow Up of High RiskMelina Defita SariNo ratings yet
- The Kangaroo NutritionDocument55 pagesThe Kangaroo NutritionMelina Defita SariNo ratings yet
- Flow Chart-30 Nov 2020pakistan-1Document4 pagesFlow Chart-30 Nov 2020pakistan-1Melina Defita SariNo ratings yet
- Kangaroo Mother Care Protocol - 19092020Document2 pagesKangaroo Mother Care Protocol - 19092020Melina Defita SariNo ratings yet
- Numbers of NursesDocument4 pagesNumbers of NursesMelina Defita SariNo ratings yet
- Kangaroo Mother Care Protocol-V4 - 19092020Document5 pagesKangaroo Mother Care Protocol-V4 - 19092020Melina Defita SariNo ratings yet
- Kangaroo Mother Care Program DiagramDocument1 pageKangaroo Mother Care Program DiagramMelina Defita SariNo ratings yet
- The Kangaroo PositionDocument45 pagesThe Kangaroo PositionMelina Defita SariNo ratings yet
- Question Words (Part 1)Document1 pageQuestion Words (Part 1)Melina Defita SariNo ratings yet
- In-Hospital KMC DiagramDocument2 pagesIn-Hospital KMC DiagramMelina Defita SariNo ratings yet
- Asking About Someone's Condition (Part 1)Document1 pageAsking About Someone's Condition (Part 1)Melina Defita SariNo ratings yet
- Talking About The Future (Part 1)Document1 pageTalking About The Future (Part 1)Melina Defita SariNo ratings yet
- How To Make A Personal Statement (Part 2)Document1 pageHow To Make A Personal Statement (Part 2)Melina Defita SariNo ratings yet
- Baju Kaos Cowok Pria Polos Surfing Distro Ripcurl RIP Curl 137 Fashion Pria Atasan PriaDocument120 pagesBaju Kaos Cowok Pria Polos Surfing Distro Ripcurl RIP Curl 137 Fashion Pria Atasan PriaMelina Defita SariNo ratings yet
- Language Tools in Public Speaking (Part 2)Document1 pageLanguage Tools in Public Speaking (Part 2)Melina Defita SariNo ratings yet
- Talk, Mention, Chat, Say, Tell, Speak, Discuss (Part 1)Document1 pageTalk, Mention, Chat, Say, Tell, Speak, Discuss (Part 1)Melina Defita SariNo ratings yet
- Question Words (Part 2)Document1 pageQuestion Words (Part 2)Melina Defita SariNo ratings yet
- Talking About The Future (Part 1)Document1 pageTalking About The Future (Part 1)Melina Defita SariNo ratings yet
- Effect of Time of Starting Assembly Post-Birth: PreliminaryDocument8 pagesEffect of Time of Starting Assembly Post-Birth: PreliminaryMelina Defita SariNo ratings yet
- Talking About The Future (Part 1)Document1 pageTalking About The Future (Part 1)Melina Defita SariNo ratings yet
- Philippine Team: Fay de Ocampo Francine Bofill Daisy PanagsaganDocument17 pagesPhilippine Team: Fay de Ocampo Francine Bofill Daisy PanagsaganMelina Defita SariNo ratings yet
- Language Tools in Public Speaking (Part 2)Document1 pageLanguage Tools in Public Speaking (Part 2)Melina Defita SariNo ratings yet
- Talk, Mention, Chat, Say, Tell, Speak, Discuss (Part 2)Document1 pageTalk, Mention, Chat, Say, Tell, Speak, Discuss (Part 2)Melina Defita SariNo ratings yet
- Why Do You Want A Job (Part 1)Document1 pageWhy Do You Want A Job (Part 1)Melina Defita SariNo ratings yet
- Asuhan Keperawatan Bayi Berat Badan Lahir Rendah di NICUDocument9 pagesAsuhan Keperawatan Bayi Berat Badan Lahir Rendah di NICUMelina Defita SariNo ratings yet
- Perception On The Role of Parenting Style On Juvenile Delinquency Among Adolescents in The Government Remand Homes Lagos State NigeriaDocument18 pagesPerception On The Role of Parenting Style On Juvenile Delinquency Among Adolescents in The Government Remand Homes Lagos State NigeriaAstin AstinNo ratings yet
- Early Childhood EducationDocument3 pagesEarly Childhood EducationLipatOla123No ratings yet
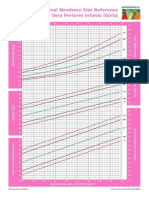
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Yogesh TripathiDocument4 pagesYogesh TripathiBilal MohammadNo ratings yet
- Part 1Document33 pagesPart 1Joseph Barnes100% (1)
- Domains of Developmental PsychologyDocument10 pagesDomains of Developmental Psychologypramod harlalkaNo ratings yet
- Identifying Child Abuse LoopholesDocument3 pagesIdentifying Child Abuse LoopholesashleighNo ratings yet
- Child Care Providers in Loudoun CountyDocument5 pagesChild Care Providers in Loudoun Countygsmeka100% (2)
- Health Care Providers List ENGLISHDocument28 pagesHealth Care Providers List ENGLISHcasey.teleskNo ratings yet
- Grandparents HandbookDocument82 pagesGrandparents HandbookPamela Nancy ElamNo ratings yet
- Daycare Decisions - Rayne LiddyDocument2 pagesDaycare Decisions - Rayne Liddyapi-534204337No ratings yet
- Ans Sf4 For The Months of June, July, August 2017Document12 pagesAns Sf4 For The Months of June, July, August 2017allanjulesNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Objectives Nursing Interventions Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Scientific Rationale Objectives Nursing Interventions Rationale EvaluationArdel LabadaNo ratings yet
- Administration of The Behavioral Pediatrics Feeding Assessment SCDocument50 pagesAdministration of The Behavioral Pediatrics Feeding Assessment SCPaula Caceres RiveraNo ratings yet
- Email:: Heriyusuf@upi - EduDocument14 pagesEmail:: Heriyusuf@upi - EduDwi SuyatmiNo ratings yet
- PR2 Group1Document2 pagesPR2 Group1Dwcb HS RegistrarNo ratings yet
- Collaborative Tasks Group 2 - Kamela NGDocument3 pagesCollaborative Tasks Group 2 - Kamela NGtherese angelieNo ratings yet
- Baby SensesDocument2 pagesBaby SensesCamille LiqueNo ratings yet
- Assessment Prelim CPE100Document4 pagesAssessment Prelim CPE100Jouf JourdynNo ratings yet
- 2018 Child Abuse Prevention Resource GuideDocument105 pages2018 Child Abuse Prevention Resource GuideJamie Wilkinson100% (1)
- Breastfeeding Assessment Tool-BAT (Mothers Version)Document1 pageBreastfeeding Assessment Tool-BAT (Mothers Version)paanar100% (1)
- Unit 4 Principles of DevelopmentDocument10 pagesUnit 4 Principles of DevelopmentRajni KesharwaniNo ratings yet
- SourcesDocument2 pagesSourcesJustin RadamNo ratings yet
- Module 3 Lesson 2Document10 pagesModule 3 Lesson 2Mark Calpon LechidoNo ratings yet
- FREE Article CTR DrChuckGeddesDocument3 pagesFREE Article CTR DrChuckGeddesAnalia FerracesNo ratings yet
- Contact Info f2f - Grade 12Document12 pagesContact Info f2f - Grade 12MAE ANN TOLENTINONo ratings yet