You might also like
- Ethics in HealthcareDocument5 pagesEthics in HealthcareEphraimNo ratings yet
- Order 4161202 - Medical EthicsDocument5 pagesOrder 4161202 - Medical EthicsJohn NdambukiNo ratings yet
- Week 7 Discussion Board Decision-MakingDocument3 pagesWeek 7 Discussion Board Decision-Makingmutoro fredNo ratings yet
- HCM 523 WK I PostDocument4 pagesHCM 523 WK I PostDanis R. AbieroNo ratings yet
- Legal and Ethical Issues in Nursing DiscussionDocument3 pagesLegal and Ethical Issues in Nursing Discussionapi-639782898No ratings yet
- Ethics of Breaking Sad News To Patient by Health C PDFDocument3 pagesEthics of Breaking Sad News To Patient by Health C PDFvidiyahNo ratings yet
- Frontiers Frvir-04-1195196 07252023Document12 pagesFrontiers Frvir-04-1195196 07252023Robert CarrilloNo ratings yet
- NSG 436 Benchmark 2 Ethical Dilemma-2Document5 pagesNSG 436 Benchmark 2 Ethical Dilemma-2api-520026903No ratings yet
- MainDocument2 pagesMainandri bachtiarNo ratings yet
- Calkins 2021Document2 pagesCalkins 2021diyanarelNo ratings yet
- Using Qualitative Research REVISEDDocument5 pagesUsing Qualitative Research REVISEDJapheth MitauNo ratings yet
- Order #350041417Document4 pagesOrder #350041417s.macharia1643No ratings yet
- Order 3161461Document4 pagesOrder 3161461sean davidNo ratings yet
- End of Life Issues in The Intensive Care Units: Review ArticleDocument6 pagesEnd of Life Issues in The Intensive Care Units: Review ArticlecindyNo ratings yet
- The Healing Touch: Keeping the Doctor-Patient Relationship Alive Under Managed CareFrom EverandThe Healing Touch: Keeping the Doctor-Patient Relationship Alive Under Managed CareRating: 5 out of 5 stars5/5 (1)
- NCM 108 Cultural RelativityDocument1 pageNCM 108 Cultural RelativityKRISTOFER DAN ACUT TRUGILLONo ratings yet
- Ethical Dilemmas in SurgeryDocument2 pagesEthical Dilemmas in Surgeryياسر مطلب عبد اللهNo ratings yet
- CDC Wonder - EditedDocument4 pagesCDC Wonder - EditedPaul WahomeNo ratings yet
- DNR and Medical FutilityDocument13 pagesDNR and Medical Futilityapi-216057141No ratings yet
- Going For Gold Sports and Exercise Groups For People With Dementia and Carers Contribute To Their Well-BeingDocument15 pagesGoing For Gold Sports and Exercise Groups For People With Dementia and Carers Contribute To Their Well-BeingDrHellenNo ratings yet
- Doctors Striking 2Document1 pageDoctors Striking 2Vijaya RajNo ratings yet
- IJSR PublishedDocument9 pagesIJSR Publishedprasetyo ediNo ratings yet
- AMA Code of Medical Ethics' Opinions Related To A Physician's Power To NameDocument4 pagesAMA Code of Medical Ethics' Opinions Related To A Physician's Power To NameJave GajellomaNo ratings yet
- Caring, Curing, Coping: Nurse, Physician, and Patient RelationshipsFrom EverandCaring, Curing, Coping: Nurse, Physician, and Patient RelationshipsNo ratings yet
- The Ethical Right To Healthcare in The Affordable Care Act PDFDocument471 pagesThe Ethical Right To Healthcare in The Affordable Care Act PDFFabricio LafebreNo ratings yet
- The Limited Right To Die: Submitted byDocument27 pagesThe Limited Right To Die: Submitted byJohn SanchezNo ratings yet
- Ethical Concerns in Nursing or HealthDocument4 pagesEthical Concerns in Nursing or HealthHILLARY SISULENo ratings yet
- JCM 10 04900Document14 pagesJCM 10 04900Chistian LassoNo ratings yet
- Frozen Shoulder JurnalDocument10 pagesFrozen Shoulder JurnalShiba MiyukiNo ratings yet
- Cost Benefit of Sustaining Life - EditedDocument6 pagesCost Benefit of Sustaining Life - EditedJohn Muthama MbathiNo ratings yet
- Ethical DilemmaDocument5 pagesEthical Dilemmaapi-520985654No ratings yet
- BuryStokes PTJ April2013Document14 pagesBuryStokes PTJ April2013Vinay KumarNo ratings yet
- ASSIGNMENT 1 6th JuneDocument5 pagesASSIGNMENT 1 6th JuneAsra Tufail DahrajNo ratings yet
- Dealing With The Ethical DilemmaDocument4 pagesDealing With The Ethical Dilemmazulfiqarali nagriNo ratings yet
- Page - 1Document23 pagesPage - 1Basco Martin JrNo ratings yet
- Etika Hub DR - PasienDocument27 pagesEtika Hub DR - PasienJamali GagahNo ratings yet
- American Sociological AssociationDocument13 pagesAmerican Sociological AssociationSuryo WibowoNo ratings yet
- 1 PDFDocument19 pages1 PDFDoni DarcoNo ratings yet
- End-Of-Life Issues For A Modern India - Lessons Learnt in The WestDocument5 pagesEnd-Of-Life Issues For A Modern India - Lessons Learnt in The WestArmando TapiasNo ratings yet
- A National Survey of Hospice Aid in Dying Policy Availability and The Impact of Legal MandatesDocument5 pagesA National Survey of Hospice Aid in Dying Policy Availability and The Impact of Legal MandatesHerald Scholarly Open AccessNo ratings yet
- Universal Bioethical Priniciple (Calustre)Document4 pagesUniversal Bioethical Priniciple (Calustre)Jerimee derf CalustreNo ratings yet
- Life Sustaining Measures 2Document4 pagesLife Sustaining Measures 2tabithaNo ratings yet
- Physical Therapist Professional EthicsDocument4 pagesPhysical Therapist Professional EthicsJohn Gabriel BaduriaNo ratings yet
- Basic Principles of Nursing Care Volina ContinueDocument2 pagesBasic Principles of Nursing Care Volina Continuealena volinaNo ratings yet
- Article 10Document8 pagesArticle 10Hamza DibNo ratings yet
- Medical Futility: 23 (Suppl. 11), 11-6-11-16 (2000)Document11 pagesMedical Futility: 23 (Suppl. 11), 11-6-11-16 (2000)cindyNo ratings yet
- Patient Rights: January 2016Document10 pagesPatient Rights: January 2016CharanNo ratings yet
- Ugcs3 v3 Project Attachments E7D4F49C 638B 4CEA A9D2 149A4A1140F5 L and L Essay 3Document6 pagesUgcs3 v3 Project Attachments E7D4F49C 638B 4CEA A9D2 149A4A1140F5 L and L Essay 3David KaufmanNo ratings yet
- What Is Chiropractic?: Debate Open AccessDocument2 pagesWhat Is Chiropractic?: Debate Open AccessRajender BishtNo ratings yet
- Ethical Issue of Physician-Assisted Suicide and EuthanasiaDocument7 pagesEthical Issue of Physician-Assisted Suicide and EuthanasiacatsupsunNo ratings yet
- Welfare and Legal Aspects of Making Decisions On Medical Treatments of Pet AnimalsDocument10 pagesWelfare and Legal Aspects of Making Decisions On Medical Treatments of Pet AnimalsAngelisa L. RazoNo ratings yet
- Chapter 18Document6 pagesChapter 18lrdn_ghrcNo ratings yet
- BuryStokes PTJ April2013Document14 pagesBuryStokes PTJ April2013Milan AnandNo ratings yet
- Paternalism in HealthcareDocument9 pagesPaternalism in Healthcarearies usamaNo ratings yet
- Improving Health Outcomes Through Patient Education and Partnerships With PatientsDocument3 pagesImproving Health Outcomes Through Patient Education and Partnerships With Patientsmanishms1No ratings yet
- Organ Donation and TransplantationDocument6 pagesOrgan Donation and TransplantationpysarchukludmylaNo ratings yet
- Hand Out - 2 Case Study + Elements of Strong JustificationDocument4 pagesHand Out - 2 Case Study + Elements of Strong JustificationasmexNo ratings yet
- Paternalism in HealthcareDocument9 pagesPaternalism in Healthcarearies usamaNo ratings yet
- Discussion PostsDocument4 pagesDiscussion Postslagatduncan520No ratings yet
- Topic Title - Reflective EssayDocument12 pagesTopic Title - Reflective EssayBlessing N. Ikiseh (Bibieandrea)No ratings yet
- Running Head: An Analysis of The Creole Language 1Document13 pagesRunning Head: An Analysis of The Creole Language 1Stephen WainainaNo ratings yet
- Business Continuity Management: Project Task On Alliance Foods Company LLCDocument7 pagesBusiness Continuity Management: Project Task On Alliance Foods Company LLCStephen WainainaNo ratings yet
- 462174034Document2 pages462174034Stephen WainainaNo ratings yet
- 450571666Document2 pages450571666Stephen WainainaNo ratings yet
- Work Attitudes in The United StatesDocument3 pagesWork Attitudes in The United StatesStephen WainainaNo ratings yet
- 450762614Document2 pages450762614Stephen WainainaNo ratings yet
- Community Service by The Coca-Cola CompanyDocument3 pagesCommunity Service by The Coca-Cola CompanyStephen WainainaNo ratings yet
- Occupational Safety and Health AdministrationDocument10 pagesOccupational Safety and Health AdministrationStephen WainainaNo ratings yet
- Women Empowement Student'S Name Institutional AffiliationDocument5 pagesWomen Empowement Student'S Name Institutional AffiliationStephen WainainaNo ratings yet
- Running Head: Environmental Forces and Trends in Healthcare 1Document7 pagesRunning Head: Environmental Forces and Trends in Healthcare 1Stephen WainainaNo ratings yet
- MKT332 Final ExamDocument7 pagesMKT332 Final ExamStephen WainainaNo ratings yet
- Water BillDocument1 pageWater BillAdnan AliNo ratings yet
- List of BFP Pensioners and Survivors For 3Rd Quarter of 2018Document6 pagesList of BFP Pensioners and Survivors For 3Rd Quarter of 2018Bfp Gma FS CaviteNo ratings yet
- Benefits of Effective Lifting ProgramDocument30 pagesBenefits of Effective Lifting ProgramMoradeke OnasanyaNo ratings yet
- KAP Customer Satisfaction Survey Questionnaire FinalDocument7 pagesKAP Customer Satisfaction Survey Questionnaire FinalBongga Ka DayNo ratings yet
- QRD Appendix V Adverse Drug Reaction Reporting Details enDocument5 pagesQRD Appendix V Adverse Drug Reaction Reporting Details enharomilanovNo ratings yet
- Cover Letter - NursingDocument1 pageCover Letter - Nursingapi-621785757No ratings yet
- History of NursingDocument33 pagesHistory of NursingMubashirNo ratings yet
- The Safe & Effective Care EnvironmentDocument140 pagesThe Safe & Effective Care EnvironmentMoreiyamNo ratings yet
- Fairford Leys Bus PDFDocument2 pagesFairford Leys Bus PDFTheresaNo ratings yet
- Documentation ActivityDocument5 pagesDocumentation ActivityAh AlshaibaniNo ratings yet
- Complaint Register 1Document79 pagesComplaint Register 1simon maaaklaNo ratings yet
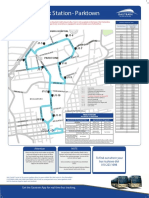
- Gautrain Park Station Parktown Map J1 BusesDocument1 pageGautrain Park Station Parktown Map J1 BusesIvory PlatypusNo ratings yet
- Access Guidebook 2022Document133 pagesAccess Guidebook 2022Paul Vincent NonatNo ratings yet
- Curriculum Vitae: Mohd MunawwarDocument3 pagesCurriculum Vitae: Mohd MunawwarMunwarNo ratings yet
- Wait Times To Medical Care and Treatment in Canada: LAWS-6046 - (34) - 22S - Emily PassanhaDocument10 pagesWait Times To Medical Care and Treatment in Canada: LAWS-6046 - (34) - 22S - Emily Passanhaemily passanhaNo ratings yet
- Presentation On Health InsuranceDocument12 pagesPresentation On Health InsuranceAditi SinghNo ratings yet
- Home Health Registered NurseDocument2 pagesHome Health Registered NurseLiwliwa LiwliwNo ratings yet
- Leave of Absence Form: Withpay W Ithout P Ay Yes NoDocument1 pageLeave of Absence Form: Withpay W Ithout P Ay Yes NoLocus Jhun MichaelNo ratings yet
- Should The UDocument4 pagesShould The Uapi-599084001No ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: 4th 'T' Block Jayanagar, Bengaluru-560041Document8 pagesRajiv Gandhi University of Health Sciences, Karnataka: 4th 'T' Block Jayanagar, Bengaluru-560041nidacon bidarNo ratings yet
- HealthDocument8 pagesHealthLily Jane MontefalcoNo ratings yet
- Community Pharmacy Symptoms Diagnosis AnDocument2 pagesCommunity Pharmacy Symptoms Diagnosis AnmnbNo ratings yet
- Adon Job DescriptionDocument5 pagesAdon Job DescriptionDickson DanielrajNo ratings yet
- Sample Survey - HMO Study - 20HMO - 20studyDocument19 pagesSample Survey - HMO Study - 20HMO - 20studyHebatallah FahmyNo ratings yet
- Books ListsDocument7 pagesBooks ListsMiguel Cadagan100% (1)
- Merp Sepco IiiDocument8 pagesMerp Sepco IiiErwadi ErwadiNo ratings yet
- 5.3 - Structured Communication Using The SBAR ToolDocument15 pages5.3 - Structured Communication Using The SBAR ToolJehad AlturkNo ratings yet
- Madison Health - Health Care Providers List 2023Document2 pagesMadison Health - Health Care Providers List 2023Sharik EssaNo ratings yet
- NURS FPX 6016 Assessment 3 Data Analysis and Quality Improvement Initative ProposalDocument6 pagesNURS FPX 6016 Assessment 3 Data Analysis and Quality Improvement Initative Proposalzadem5266No ratings yet
- MD, TranscriptDocument2 pagesMD, TranscriptRohullah SultaniNo ratings yet