You might also like
- Week 2Document26 pagesWeek 2Shilpi SinghalNo ratings yet
- Effectiveness of Planned Teaching Programme On Knowledge Regarding Identification of Danger Signs in Neonates Among Post-Natal MothersDocument4 pagesEffectiveness of Planned Teaching Programme On Knowledge Regarding Identification of Danger Signs in Neonates Among Post-Natal MothersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 KMCDocument4 pages1 KMCahid3safitraNo ratings yet
- Preterm Complications..Document89 pagesPreterm Complications..UdayBhaskar ChinthaNo ratings yet
- Macro Teaching - Care of Baby in VentilatorDocument13 pagesMacro Teaching - Care of Baby in VentilatorSheena SharmaNo ratings yet
- A Quasi Experimental Study To Evaluate The Effect of Prefeeding Oral Stimulation Program On Oral Feeding Skills Among Preterm Infants in Selected Hospitals, PunjabDocument29 pagesA Quasi Experimental Study To Evaluate The Effect of Prefeeding Oral Stimulation Program On Oral Feeding Skills Among Preterm Infants in Selected Hospitals, PunjabEditor IJTSRD100% (1)
- New Born Case StudyDocument4 pagesNew Born Case StudyErick SanangaNo ratings yet
- Fix Care of NewbornDocument39 pagesFix Care of Newborngratzia fionaNo ratings yet
- LESSON PLAN of Sandhya SisDocument5 pagesLESSON PLAN of Sandhya SisAshish GuptaNo ratings yet
- CCSBS) : CSBS DP Infant-Toddler ChecklistDocument3 pagesCCSBS) : CSBS DP Infant-Toddler Checklistİpek OMURNo ratings yet
- An Essay AboutDocument3 pagesAn Essay Aboutamoghlingamalla100% (1)
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Weaning Among Mothers of InfantsDocument5 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding Weaning Among Mothers of InfantsEditor IJTSRD100% (1)
- FamilyDocument19 pagesFamilyVaishnavee Singh100% (1)
- Pediatric NotesDocument4 pagesPediatric NotesJincy PrinceNo ratings yet
- Health Edu. On Breast Feedind WASEEM-1Document7 pagesHealth Edu. On Breast Feedind WASEEM-1MysaraNo ratings yet
- Assessment of Beonate - FN - IIIDocument79 pagesAssessment of Beonate - FN - IIIashamartinaNo ratings yet
- A Study To Assess The Effectiveness of Information Booklet On Knowledge Regarding Breastfeeding Techniques Among Primipara Mothers in Selected Hospitals at Bhopal M.P.Document8 pagesA Study To Assess The Effectiveness of Information Booklet On Knowledge Regarding Breastfeeding Techniques Among Primipara Mothers in Selected Hospitals at Bhopal M.P.Editor IJTSRDNo ratings yet
- كتاب عملى تمريض الاطفالDocument56 pagesكتاب عملى تمريض الاطفالziad aymanNo ratings yet
- Congenital Malformations and Fetal DevelopmentDocument14 pagesCongenital Malformations and Fetal DevelopmentMartha LubasiNo ratings yet
- Iycf Who PDFDocument157 pagesIycf Who PDFMarilyn RealistaNo ratings yet
- Student Assess Knowledge and Awareness Among Post Natal Mother'S Regarding Kangaroo Mother CareDocument112 pagesStudent Assess Knowledge and Awareness Among Post Natal Mother'S Regarding Kangaroo Mother CareSunny ProNo ratings yet
- Hand Out PDFDocument6 pagesHand Out PDFJoanna Lyn PonceNo ratings yet
- A Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Dangerous Signs of New Born Among The Postnatal Mothers at Selected Hospitals, LucknowDocument9 pagesA Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Dangerous Signs of New Born Among The Postnatal Mothers at Selected Hospitals, LucknowEditor IJTSRDNo ratings yet
- BF12 Formula FeedingDocument5 pagesBF12 Formula FeedingFikri Ulil AlbabNo ratings yet
- Management of Fever in ChildrenDocument1 pageManagement of Fever in ChildrensabirNo ratings yet
- Spina Bifida Guide: Types, Causes & Nursing CareDocument5 pagesSpina Bifida Guide: Types, Causes & Nursing CareJulliza Joy PandiNo ratings yet
- Minordisordersofbnewborn 161129154708Document33 pagesMinordisordersofbnewborn 161129154708Kevin Daniel GoveasNo ratings yet
- 5 Hospitalized Child Nursing Care PlansDocument13 pages5 Hospitalized Child Nursing Care PlansAyesha ImtiazNo ratings yet
- Newborn CareDocument49 pagesNewborn CareJohn Mark PocsidioNo ratings yet
- SurveyDocument7 pagesSurveyalphons josephNo ratings yet
- Birth InjuriesDocument13 pagesBirth Injuriesrittika dasNo ratings yet
- Essential Infant Nutrition: Benefits of Exclusive BreastfeedingDocument11 pagesEssential Infant Nutrition: Benefits of Exclusive BreastfeedingRosa PalconitNo ratings yet
- Nursing Care of Newborn AssessmentDocument15 pagesNursing Care of Newborn AssessmentMary RoseNo ratings yet
- ImmunityDocument19 pagesImmunityKailash Nagar100% (1)
- Newborn Bath ChecklistDocument6 pagesNewborn Bath ChecklistAL HAMIER DAUD DAGANIONo ratings yet
- National Nutrition ProgramDocument3 pagesNational Nutrition ProgramAbdul Ghaffar BughioNo ratings yet
- Trends in Midwifry and ObstetricsDocument8 pagesTrends in Midwifry and ObstetricsVarna MohanNo ratings yet
- Therapeutic PlayDocument9 pagesTherapeutic PlayVivek PrabhakarNo ratings yet
- National Policy For ChildrenDocument5 pagesNational Policy For Childrenthilaga88No ratings yet
- Care of The Hospitalized ChildDocument60 pagesCare of The Hospitalized ChildJSeasharkNo ratings yet
- A Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Exclusive Breastfeeding Among Nursing Mothers in Postnatal Ward of Selected Maternity Settings at LucknowDocument13 pagesA Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Exclusive Breastfeeding Among Nursing Mothers in Postnatal Ward of Selected Maternity Settings at LucknowEditor IJTSRDNo ratings yet
- Hospital Management System Project ReportDocument28 pagesHospital Management System Project ReportYash SrivastavaNo ratings yet
- Ethical Issues in NeonateDocument11 pagesEthical Issues in Neonatethilaga880% (1)
- Cleft Lip and Cleft PalateDocument27 pagesCleft Lip and Cleft Palatenamah odatNo ratings yet
- Paediatric Booklet by Win Nursing CoachingDocument116 pagesPaediatric Booklet by Win Nursing CoachingAkshya YadavNo ratings yet
- Code of Ethics in NursingDocument8 pagesCode of Ethics in NursingSallieNo ratings yet
- Comparison Theories PDFDocument3 pagesComparison Theories PDFエド パジャロンNo ratings yet
- Principles of Growth & DevelopmentDocument43 pagesPrinciples of Growth & DevelopmentDIZZA MAE BATURIANONo ratings yet
- HYPERBILIRUBINEMIADocument30 pagesHYPERBILIRUBINEMIAAlexisRoyE100% (1)
- A Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Management of Low Birth Weight LBW Babies Among Postnatal Mothers in Selected Community at GwaliorDocument7 pagesA Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Management of Low Birth Weight LBW Babies Among Postnatal Mothers in Selected Community at GwaliorEditor IJTSRDNo ratings yet
- Bladder Extrophy: Medical ManagementDocument8 pagesBladder Extrophy: Medical ManagementChristian James CamaongayNo ratings yet
- Handbook For ASHA On Home Based Care For Young Child-EnglishDocument116 pagesHandbook For ASHA On Home Based Care For Young Child-EnglishDr. Vanitha BNo ratings yet
- DDST Patient Co PDFDocument3 pagesDDST Patient Co PDFkamelisshaNo ratings yet
- Spina Bifida: Causes, Types and SymptomsDocument95 pagesSpina Bifida: Causes, Types and SymptomsEric ChristianNo ratings yet
- INTRODUCTIONDocument26 pagesINTRODUCTIONTina Manoj100% (1)
- Growth & Development of A PreschoolerDocument6 pagesGrowth & Development of A Preschoolerta CNo ratings yet
- Child Development: Prof. Rachelle Gay R. Pacial, MSN, RN Saint Louis University School of NursingDocument26 pagesChild Development: Prof. Rachelle Gay R. Pacial, MSN, RN Saint Louis University School of NursingRachelle Gay PacialNo ratings yet
- CHILD HEALTH NURSING: Growth and DevelopmentDocument67 pagesCHILD HEALTH NURSING: Growth and DevelopmentEllen Angel100% (3)
- Affidavit of Accident Dominador Rosario BagamaspadDocument2 pagesAffidavit of Accident Dominador Rosario BagamaspadJaime GonzalesNo ratings yet
- Atkinson R L - Weight CyclingDocument7 pagesAtkinson R L - Weight CyclingmaddafackerNo ratings yet
- Cricket Academy Head Coach RoleDocument4 pagesCricket Academy Head Coach Roletauseef1716No ratings yet
- Water Treatment PDFDocument87 pagesWater Treatment PDFJubin KumarNo ratings yet
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- Breaking The Silence - Art TherapyDocument43 pagesBreaking The Silence - Art TherapyAdriana100% (1)
- 11.0 - Safety in The Heat v3.0 EnglishDocument14 pages11.0 - Safety in The Heat v3.0 EnglishAnonymous hBBam1nNo ratings yet
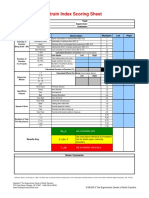
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- Fat-Burning FoodsDocument11 pagesFat-Burning FoodsRamzi FaddoulNo ratings yet
- Errata 1Document9 pagesErrata 1Doc AhsanNo ratings yet
- Nursing assessment diagnosis interventions rationale evaluationDocument3 pagesNursing assessment diagnosis interventions rationale evaluationanimesh pandaNo ratings yet
- HRM Case StudyDocument21 pagesHRM Case StudyNabil Eyg Iakini100% (1)
- Unit 1-Omd553-Telehealth TechnologyDocument53 pagesUnit 1-Omd553-Telehealth TechnologyjgjeslinNo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet
- Hum. Reprod.-1999-Tesarik-1318-23Document6 pagesHum. Reprod.-1999-Tesarik-1318-23Meilana Sapta DNo ratings yet
- Training Needs Analysis FormDocument4 pagesTraining Needs Analysis FormLizjasmine DimayaNo ratings yet
- Introduction To The Alpaca andDocument9 pagesIntroduction To The Alpaca andMai Chi PhạmNo ratings yet
- Rock Solid Immunity, Naturally - by Rajeev Agarwal R3Document5 pagesRock Solid Immunity, Naturally - by Rajeev Agarwal R3Rajeev B AgarwalNo ratings yet
- Calculator NotesDocument4 pagesCalculator NotessdiamanNo ratings yet
- Booklet - e 1 - 2013Document101 pagesBooklet - e 1 - 2013Dani AedoNo ratings yet
- Preface: Color Profile: Disabled Composite Default ScreenDocument2 pagesPreface: Color Profile: Disabled Composite Default ScreenCláudio CastroNo ratings yet
- EBM TerbaruDocument5 pagesEBM TerbaruTetty PrasetyaNo ratings yet
- Metabolic Surge - Rapid Fat Loss ProgramDocument5 pagesMetabolic Surge - Rapid Fat Loss ProgramTamer Luka100% (2)
- Neonatal Care Pocket Guide For Hospital Physicians PDFDocument319 pagesNeonatal Care Pocket Guide For Hospital Physicians PDFelmaadawy2002100% (7)
- Pothole Claim Form in PhiladelphiaDocument3 pagesPothole Claim Form in Philadelphiaphilly victorNo ratings yet
- Top 10 Graphic Design Interview Questions and AnswersDocument16 pagesTop 10 Graphic Design Interview Questions and Answersbetsjonh100% (1)
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- Umftgm 2017 MarissiensisDocument148 pagesUmftgm 2017 MarissiensisAdriana VillarrealNo ratings yet
- Asq 3 42 MDocument8 pagesAsq 3 42 MMohammed AlsuwaidiNo ratings yet