You might also like
- Homeschooling PaperDocument13 pagesHomeschooling Paperapi-509508817No ratings yet
- Standard Operating Procedures On Assessment of Staff Training and CompetencyDocument4 pagesStandard Operating Procedures On Assessment of Staff Training and Competencyclairealbertini50% (6)
- Interprofessional Collaboration Three Best Practice Models of Interprofessional EducationDocument11 pagesInterprofessional Collaboration Three Best Practice Models of Interprofessional Educationgenta01100% (1)
- Tableau Developer SeniorDocument10 pagesTableau Developer SeniorSureshAtluriNo ratings yet
- The Mountain of Ignorance (Sunday Adelaja) (Z-Library)Document179 pagesThe Mountain of Ignorance (Sunday Adelaja) (Z-Library)wilfried kassiNo ratings yet
- Tle Laboratory ManualDocument7 pagesTle Laboratory ManualAileene Montenegro83% (18)
- ABB-QA-Test Strategy (9AAD134969)Document38 pagesABB-QA-Test Strategy (9AAD134969)Abhishek Gupta100% (1)
- AITCSArticle InstrumenDocument11 pagesAITCSArticle InstrumenYulianti WulandariNo ratings yet
- Impact of Simulation On Student Attitudes AboutDocument8 pagesImpact of Simulation On Student Attitudes AboutJASMIEN AISYA SASTIARINI AISYA SASTIARININo ratings yet
- Interprofessional Collaboration Three Best Practice Models of Interprofessional EducationDocument11 pagesInterprofessional Collaboration Three Best Practice Models of Interprofessional Educationanzila widyaNo ratings yet
- I Pe Artikel Individ UDocument16 pagesI Pe Artikel Individ UadelllblNo ratings yet
- KeeblerDietzLazzaraetal.2014 TeamSTEPPST TPQCFAValidationDocument11 pagesKeeblerDietzLazzaraetal.2014 TeamSTEPPST TPQCFAValidationHW HYHZNo ratings yet
- Jurnal ReferensiDocument10 pagesJurnal ReferensiBidang KeperawatanNo ratings yet
- CF Exemplar NURS-FPX4020 Assessment 4Document13 pagesCF Exemplar NURS-FPX4020 Assessment 4Sabahat BashirNo ratings yet
- Ijerph 19 03722Document14 pagesIjerph 19 03722ilhamNo ratings yet
- An Approach To Integrating Interprofessional Education in Collaborative Mental Health CareDocument6 pagesAn Approach To Integrating Interprofessional Education in Collaborative Mental Health Careanas tasyaNo ratings yet
- 1.current Trends in Interprofessional Education of Health Sciences StudentsDocument8 pages1.current Trends in Interprofessional Education of Health Sciences StudentsNguyên NguyễnNo ratings yet
- Sessionsetal High Alert Meds 919 JANDocument15 pagesSessionsetal High Alert Meds 919 JANichabojanNo ratings yet
- Omura 2017Document9 pagesOmura 2017Wijah watiNo ratings yet
- MickenRodger EffectiveTeams Aug2005Document15 pagesMickenRodger EffectiveTeams Aug200504Alya RahmaNo ratings yet
- Nembhard Edmondson - 2006 Making It Safe-The Effects of Leader Inclusiveness PDFDocument26 pagesNembhard Edmondson - 2006 Making It Safe-The Effects of Leader Inclusiveness PDFMd. Shahfayet JinnahNo ratings yet
- Developing Interprofessional Communication SkillsDocument5 pagesDeveloping Interprofessional Communication SkillsWai AbrahamNo ratings yet
- Surviving Workplace Adversity A QualitatDocument9 pagesSurviving Workplace Adversity A QualitatpecescdNo ratings yet
- Health Literacy and Children Recommendations For ADocument8 pagesHealth Literacy and Children Recommendations For ASIRIUS RTNo ratings yet
- Levett-Jones Et Al-2018-Journal of Nursing Scholarship1Document10 pagesLevett-Jones Et Al-2018-Journal of Nursing Scholarship1Nande BandeNo ratings yet
- Rapid Response QualitativeDocument14 pagesRapid Response QualitativeAprilia Putri RahmadhaniNo ratings yet
- Interprofessional Teamwork Skills As Predictors of Clinical Outcomes in A Simulated Healthcare SettingDocument6 pagesInterprofessional Teamwork Skills As Predictors of Clinical Outcomes in A Simulated Healthcare SettingNavis NaldoNo ratings yet
- Learning - The Only Way To Improve Health-Care Outcomes: J Deane Waldman and Steven A YourstoneDocument11 pagesLearning - The Only Way To Improve Health-Care Outcomes: J Deane Waldman and Steven A YourstoneAlex GuNo ratings yet
- Sorensen 2018Document36 pagesSorensen 2018munira althukairNo ratings yet
- Measuring Well-Being in A College Campus Setting White PaperDocument52 pagesMeasuring Well-Being in A College Campus Setting White PaperIra LampayanNo ratings yet
- The Critical Need For Nursing Education To Address The Diag - 2021 - Nursing OutDocument8 pagesThe Critical Need For Nursing Education To Address The Diag - 2021 - Nursing OutWakhida PuspitaNo ratings yet
- Quality and Strength of Patient Safety Climate On Medical-Surgical UnitsDocument11 pagesQuality and Strength of Patient Safety Climate On Medical-Surgical UnitsFery AdlansyahNo ratings yet
- Sacks Et Al. - 2015 - Teamwork, Communication and Safety Climate A Systematic Review of Interventions To Improve Surgical CultureDocument11 pagesSacks Et Al. - 2015 - Teamwork, Communication and Safety Climate A Systematic Review of Interventions To Improve Surgical CultureEdy Tahir MattoreangNo ratings yet
- Vogus Sutcliffe 2007 BDocument6 pagesVogus Sutcliffe 2007 BLilymayyuniNo ratings yet
- PDFDocument15 pagesPDFKarine SchmidtNo ratings yet
- Sicometrik ICP IndonesiaDocument10 pagesSicometrik ICP IndonesiaUchi SuhermanNo ratings yet
- Mentorship in An Academic Medical CenterDocument4 pagesMentorship in An Academic Medical CenternoniinnNo ratings yet
- 257.full 2Document9 pages257.full 2Christian N KarisoNo ratings yet
- Reflection Commentary Final Print VersionDocument10 pagesReflection Commentary Final Print VersionHailane BragaNo ratings yet
- Bucknall 2016Document13 pagesBucknall 2016mnazri98No ratings yet
- The Association Between Health Care Staff EngagementDocument10 pagesThe Association Between Health Care Staff Engagementtsa638251No ratings yet
- The Clinical Reasoning Mapping Exercise (CResME) )Document5 pagesThe Clinical Reasoning Mapping Exercise (CResME) )Frederico PóvoaNo ratings yet
- Validation of The Educational Stress Scale For AdoDocument25 pagesValidation of The Educational Stress Scale For AdoHai My NguyenNo ratings yet
- Declaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESDocument9 pagesDeclaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESjaldoquiNo ratings yet
- How To Be A Very Safe Maternity Unit An Ethnograp - 2019 - Social Science - MedDocument9 pagesHow To Be A Very Safe Maternity Unit An Ethnograp - 2019 - Social Science - MedAkinsola Samuel TundeNo ratings yet
- 1 - Mousa (2021) - Woman Leadership in HealthcareDocument11 pages1 - Mousa (2021) - Woman Leadership in Healthcaregundah noor cahyoNo ratings yet
- A Thesis (Proposal) Presented To The Faculty of The College of Nursing Adamson UniversityDocument22 pagesA Thesis (Proposal) Presented To The Faculty of The College of Nursing Adamson UniversityRaidis PangilinanNo ratings yet
- Health Promotion Overview: Evidence-Based Strategies For Occupational Health Nursing PracticeDocument9 pagesHealth Promotion Overview: Evidence-Based Strategies For Occupational Health Nursing PracticeAdrîîana FdEzNo ratings yet
- Assessing The Awareness On Occupational Safety andDocument10 pagesAssessing The Awareness On Occupational Safety andmariel orbetaNo ratings yet
- Academic-Clinical Service Partnerships Are Innovative Strategies To Advance Patient Safety Competence and Leadership in Prelicensure Nursing StudentsDocument5 pagesAcademic-Clinical Service Partnerships Are Innovative Strategies To Advance Patient Safety Competence and Leadership in Prelicensure Nursing StudentsYiyiz HertikaNo ratings yet
- Perceptions of Factors Associated With Inclusive Work and Learning Environments in Health Care Organizations A Qualitative Narrative AnalysisDocument14 pagesPerceptions of Factors Associated With Inclusive Work and Learning Environments in Health Care Organizations A Qualitative Narrative AnalysisAndrea Guerrero ZapataNo ratings yet
- AssessmentDocument9 pagesAssessmentdian maya puspitaNo ratings yet
- Safer Coalmines, Happier, Healthier and More Engaged CanariesDocument3 pagesSafer Coalmines, Happier, Healthier and More Engaged CanariesahmedsobhNo ratings yet
- Collegian: Michelle Barakat-Johnson, Michelle Lai, Timothy Wand, Kathryn WhiteDocument8 pagesCollegian: Michelle Barakat-Johnson, Michelle Lai, Timothy Wand, Kathryn WhiteSUCHETA DASNo ratings yet
- Ginsburg 2010Document26 pagesGinsburg 2010ReginaPutriAprizaNo ratings yet
- Asian Nursing ResearchDocument7 pagesAsian Nursing ResearchWayan Dyego SatyawanNo ratings yet
- Mindfulness in The OR A Pilot Study Investigating The Effi - 2021 - JournalDocument12 pagesMindfulness in The OR A Pilot Study Investigating The Effi - 2021 - JournalLuz GarciaNo ratings yet
- 2019 - Lee & Quinn - A Lit ReviewDocument7 pages2019 - Lee & Quinn - A Lit ReviewazeemathmariyamNo ratings yet
- Text Analysis ReportDocument5 pagesText Analysis ReportElvis Rodgers DenisNo ratings yet
- Content ServerDocument11 pagesContent ServerMona AL-FaifiNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- International Journal of Nursing Studies: Kelly J. Morrow, Allison M. Gustavson, Jacqueline JonesDocument10 pagesInternational Journal of Nursing Studies: Kelly J. Morrow, Allison M. Gustavson, Jacqueline JonesFirman Suryadi RahmanNo ratings yet
- Faculty Development CPDDocument6 pagesFaculty Development CPDAida TantriNo ratings yet
- Effect of Transformational Leadership On Job Satisfaction An - 2018 - Nursing OuDocument10 pagesEffect of Transformational Leadership On Job Satisfaction An - 2018 - Nursing OuJuan Jesús F. Valera MariscalNo ratings yet
- Health Promotion in Medical Education Lessons From A Major Undergraduate Curriculum ImplementationDocument10 pagesHealth Promotion in Medical Education Lessons From A Major Undergraduate Curriculum ImplementationKAREN VANESSA MUÑOZ CHAMORRONo ratings yet
- Comprehensive Healthcare Simulation: Mastery Learning in Health Professions EducationFrom EverandComprehensive Healthcare Simulation: Mastery Learning in Health Professions EducationNo ratings yet
- Nlit1 1609Document8 pagesNlit1 1609fransiskus mekuNo ratings yet
- Interprofessional Education (Ipe) Improves Students' Communication Skills: A Literature ReviewDocument11 pagesInterprofessional Education (Ipe) Improves Students' Communication Skills: A Literature Reviewfransiskus mekuNo ratings yet
- Kelompok 4Document11 pagesKelompok 4fransiskus mekuNo ratings yet
- Kelompok 3Document9 pagesKelompok 3fransiskus mekuNo ratings yet
- Ethical NursingDocument13 pagesEthical Nursingfransiskus mekuNo ratings yet
- Konflik Kepentingan Di PPDBDocument13 pagesKonflik Kepentingan Di PPDBMOCHAMMAD HABIB SAPUTRANo ratings yet
- Foreign Stud and Local Lit RechelDocument1 pageForeign Stud and Local Lit RechelMeane BalbontinNo ratings yet
- New Approaches To Managing StressDocument5 pagesNew Approaches To Managing Stresssmith.kevin1420344No ratings yet
- LP Educ70Document9 pagesLP Educ70Romina DaquelNo ratings yet
- Social Entrepreneur Mr. Rajendra JoshiDocument9 pagesSocial Entrepreneur Mr. Rajendra JoshiChintan DesaiNo ratings yet
- Activity No. 1Document1 pageActivity No. 1Rolando Lima Jr.No ratings yet
- Information Sheet 3.2-1 - Cultural AwarenessDocument13 pagesInformation Sheet 3.2-1 - Cultural AwarenessWyattbh AaronwyattNo ratings yet
- 2018 CPD CFlyer 3Document3 pages2018 CPD CFlyer 3zolalkkNo ratings yet
- Electrical and Computer Engineering CatalogDocument9 pagesElectrical and Computer Engineering CatalogNadisanka RupasingheNo ratings yet
- Cambryn: RubinDocument1 pageCambryn: Rubinapi-451265252No ratings yet
- Post Event Report WritingDocument6 pagesPost Event Report WritingMansi PatelNo ratings yet
- WHLP-March 5!Grade-7-Q2-W7-8Document4 pagesWHLP-March 5!Grade-7-Q2-W7-8Caryl Ann C. SernadillaNo ratings yet
- Course Syllabus For The Course Psychological TestingDocument3 pagesCourse Syllabus For The Course Psychological TestingFrehiwot AleneNo ratings yet
- Affidavit of 2 Disinterested Person Stating DiscrifancyDocument1 pageAffidavit of 2 Disinterested Person Stating DiscrifancyRich RazonNo ratings yet
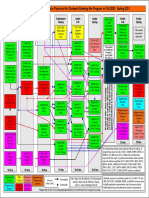
- Mechanicalengineering Sequence Chartfor Fall 2020 To Spring 2021Document1 pageMechanicalengineering Sequence Chartfor Fall 2020 To Spring 2021RonaldNo ratings yet
- PPGDocument5 pagesPPGapi-253644880No ratings yet
- Lucerne Festival AcademyDocument6 pagesLucerne Festival AcademyEduardo SantosNo ratings yet
- Articles: Self-Improvement Tips Based On Proven Scientific ResearchDocument3 pagesArticles: Self-Improvement Tips Based On Proven Scientific ResearchMike ReyesNo ratings yet
- The Role of Pragmatics in Second Language Teaching PDFDocument63 pagesThe Role of Pragmatics in Second Language Teaching PDFAndreaMaeBaltazarNo ratings yet
- Fisrt Quarter Exam For English 8Document5 pagesFisrt Quarter Exam For English 8Kathleen Legaspi MartinezNo ratings yet
- Your Personal: Masterclass WorkbookDocument10 pagesYour Personal: Masterclass WorkbookRohit RoyNo ratings yet
- Exam 2º Bachillerato.Document2 pagesExam 2º Bachillerato.Bautista Ramos SaíñasNo ratings yet
- Descriptive Essay of PlaceDocument2 pagesDescriptive Essay of PlacedinnielNo ratings yet
- Open House Checklist 18-19Document1 pageOpen House Checklist 18-19api-467926588No ratings yet