You might also like
- Ramain Medical CertificateDocument1 pageRamain Medical CertificateAlibasher MacalnasNo ratings yet
- Medical Certificate II 1Document1 pageMedical Certificate II 1Ky Namseok LaparanNo ratings yet
- Ts Govt Telangana Physical Fitness FormDocument1 pageTs Govt Telangana Physical Fitness FormSantosh Santosh100% (2)
- Icu Progress Note #1Document2 pagesIcu Progress Note #1Shane Allen100% (7)
- Non Conformity Report and Corrective, Preventive Action RequestDocument1 pageNon Conformity Report and Corrective, Preventive Action RequestvinothNo ratings yet
- TS GOVT TELANGANA Physical Fitness FormDocument1 pageTS GOVT TELANGANA Physical Fitness Formanil kumar80% (25)
- Cannabis Class Action Lawsuit - UHDocument2 pagesCannabis Class Action Lawsuit - UHTony Lange100% (1)
- ID Application FormsDocument5 pagesID Application Formskez leigh AmberNo ratings yet
- Digital Transformation in The HealthcareDocument19 pagesDigital Transformation in The Healthcaresheila kimberlyNo ratings yet
- Med CertDocument1 pageMed CertAngelieV.Remedios100% (1)
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 Palarogtunida100% (1)
- FMLA Blank FormDocument4 pagesFMLA Blank FormAndy WilsonNo ratings yet
- TB Skin Test FormDocument1 pageTB Skin Test Formapi-381635811No ratings yet
- Psychomotor Skills Outcome FormDocument1 pagePsychomotor Skills Outcome FormFray BotodNo ratings yet
- ACE MIPS Attestation 22FEB2018Document1 pageACE MIPS Attestation 22FEB2018jmauldinNo ratings yet
- Medical Screening FormDocument2 pagesMedical Screening FormibrahimNo ratings yet
- Medical Fitness CertificateDocument1 pageMedical Fitness Certificateshahid94lhrNo ratings yet
- Tags and Record of InspectionDocument1 pageTags and Record of Inspectionjim tauNo ratings yet
- REINSTATEMENT-FORM-1Document1 pageREINSTATEMENT-FORM-1Joana Ruthche T ButialNo ratings yet
- Operating Room Case Slip SummaryDocument2 pagesOperating Room Case Slip SummaryLoungayvan BatuyogNo ratings yet
- Philippine College of Occupational Medicine, Inc. (PCOM)Document3 pagesPhilippine College of Occupational Medicine, Inc. (PCOM)Kat S. Paule, MDNo ratings yet
- Financial Aid Program: Innovative Institute of Training and Services®Document1 pageFinancial Aid Program: Innovative Institute of Training and Services®Malik Sohail AwanNo ratings yet
- Aics Ce For BeneficiaryDocument1 pageAics Ce For BeneficiaryJaz AchNo ratings yet
- Attending Physicians Statement-Disability Claim Ver2.1 - English - tcm47-27477Document2 pagesAttending Physicians Statement-Disability Claim Ver2.1 - English - tcm47-27477saika tabbasumNo ratings yet
- Signature/thumb Impression of Person Whose Examination Has Been Conducted or Guardian (In Case Victim Is Minor, Relation, Student, Insane)Document8 pagesSignature/thumb Impression of Person Whose Examination Has Been Conducted or Guardian (In Case Victim Is Minor, Relation, Student, Insane)Joy SinghNo ratings yet
- 10 Case Slips Scrub Circulating Delivery New Born REVISED Doc RevisedDocument2 pages10 Case Slips Scrub Circulating Delivery New Born REVISED Doc RevisedIrish Paping TucyapaoNo ratings yet
- CPS Dependent Information FormDocument2 pagesCPS Dependent Information Formtristero312No ratings yet
- 3 VSR Updated Form (6-3-2021) 2Document5 pages3 VSR Updated Form (6-3-2021) 2Zeeshan KhanNo ratings yet
- Final Hra-Hrdta-Form-01Document13 pagesFinal Hra-Hrdta-Form-01Charisse Jean PelominoNo ratings yet
- RRT Evaluation FormDocument1 pageRRT Evaluation FormNurul IkmaliyahNo ratings yet
- Form Must Be Returned Within 15 Days. Parts 1-3 Must Be Completed For The Application To Be ApprovedDocument1 pageForm Must Be Returned Within 15 Days. Parts 1-3 Must Be Completed For The Application To Be ApprovedKenneth SandersNo ratings yet
- Checklist of Requirements For Hospital Accreditation (Secondary)Document4 pagesChecklist of Requirements For Hospital Accreditation (Secondary)pamgelNo ratings yet
- CFPA-Medical ExpensesDocument2 pagesCFPA-Medical ExpensesDivya VoletiNo ratings yet
- Certificate of Appearance Philippines Bureau Animal Industry Official BusinessDocument2 pagesCertificate of Appearance Philippines Bureau Animal Industry Official BusinessyoyongNo ratings yet
- Preschool Injury Occurance Incident ReportDocument4 pagesPreschool Injury Occurance Incident ReportIrene IvyNo ratings yet
- Purchase Request: Cagayan Valley Medical Center Cagayan Valley Medical CenterDocument26 pagesPurchase Request: Cagayan Valley Medical Center Cagayan Valley Medical CenterAlex SibalNo ratings yet
- Medical Certificate: Khyber Pakhtunkhwa Medical Form No. 4Document1 pageMedical Certificate: Khyber Pakhtunkhwa Medical Form No. 4Taimur Abdullah100% (1)
- Medical Examination Result SheetDocument1 pageMedical Examination Result SheetJuan Wil CenturyNo ratings yet
- Medical Examination Result SheetDocument1 pageMedical Examination Result SheetDebands LimatocNo ratings yet
- Medical Examination Result SheetDocument1 pageMedical Examination Result SheetDuran Kdj JonardNo ratings yet
- PNP Medical Examination Result Sheet TitleDocument1 pagePNP Medical Examination Result Sheet TitleGlorious El DomineNo ratings yet
- Travel and Overtime FormsDocument2 pagesTravel and Overtime FormsJUVIE DUTERTENo ratings yet
- Solar Rebate FormDocument2 pagesSolar Rebate FormsandyolkowskiNo ratings yet
- Microsoft Word - Form Electronic Funds Transfer (EFT) Settlement 20th AnnivDocument2 pagesMicrosoft Word - Form Electronic Funds Transfer (EFT) Settlement 20th Annivannekay dacresNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroAllen EndayaNo ratings yet
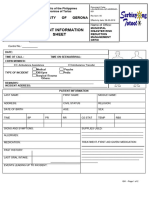
- Quality-Form-Incident Information SheetDocument2 pagesQuality-Form-Incident Information Sheetnjbxhycn4bNo ratings yet
- CI: No Erasures Complete and Correct Data Sign in Blue Pen UC-VPAA-CON-FORM-10a June 2012 Rev. 00Document2 pagesCI: No Erasures Complete and Correct Data Sign in Blue Pen UC-VPAA-CON-FORM-10a June 2012 Rev. 00Illya AnnesyNo ratings yet
- Purchase Request EpsonDocument2 pagesPurchase Request EpsonDeng SeseNo ratings yet
- Regional Paramedical Services, Inc.Document1 pageRegional Paramedical Services, Inc.Richard SheddNo ratings yet
- Claim FormDocument1 pageClaim FormAziz Ahmad0% (1)
- CT REFERRAL PACKAGE FOR AXXESS IMAGING April 2020Document4 pagesCT REFERRAL PACKAGE FOR AXXESS IMAGING April 2020JovanyGrezNo ratings yet
- Request for CT Scan Non-OHIP CoverageDocument4 pagesRequest for CT Scan Non-OHIP CoverageJovanyGrezNo ratings yet
- COVID-19-Revised-Monitoring-Form-2021Document3 pagesCOVID-19-Revised-Monitoring-Form-2021Aaron Paul BernasNo ratings yet
- Application For Reinstatement of Membeship Mas 65 MRBS Plus 3Document1 pageApplication For Reinstatement of Membeship Mas 65 MRBS Plus 3alnazherkaray55No ratings yet
- Philippine Health Insurance FormDocument1 pagePhilippine Health Insurance FormMarilou G. EsparagozaNo ratings yet
- Enrolment Form 2014Document8 pagesEnrolment Form 2014api-289121841No ratings yet
- ZONE - Adult Release Form 2011Document2 pagesZONE - Adult Release Form 2011Stephen RagsdaleNo ratings yet
- Medical Certificate: The National University Hospital University of The Philippine ManilaDocument2 pagesMedical Certificate: The National University Hospital University of The Philippine ManilaEira OrateNo ratings yet
- Referral FormDocument1 pageReferral FormVirginia Dare Behavioral Health ServicesNo ratings yet
- Internal controls for accounts receivableDocument3 pagesInternal controls for accounts receivableanon_266036241No ratings yet
- Annexure II - Medical Fitness Form - 2020 22 - 20 MayDocument1 pageAnnexure II - Medical Fitness Form - 2020 22 - 20 MayAgrim RawatNo ratings yet
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipFrom EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo ratings yet
- CTASDocument1 pageCTASJm uniteNo ratings yet
- Triage Assessment SlipDocument1 pageTriage Assessment SlipJm unite100% (1)
- List of Emergency DrugsDocument1 pageList of Emergency DrugsJm uniteNo ratings yet
- Who Standardized Emergency Unit Form TraumaDocument2 pagesWho Standardized Emergency Unit Form TraumaJm uniteNo ratings yet
- ED/Trauma Center Organogram StructureDocument1 pageED/Trauma Center Organogram StructureJm uniteNo ratings yet
- Fireworks-Related Injury Surveillance ReportDocument3 pagesFireworks-Related Injury Surveillance ReportJm uniteNo ratings yet
- FWRI Surveillance Orientation 2021Document20 pagesFWRI Surveillance Orientation 2021Jm uniteNo ratings yet
- South Dakota EMS Patient Care Report FormDocument2 pagesSouth Dakota EMS Patient Care Report FormJm uniteNo ratings yet
- Performance Evaluation Supervisor FormDocument13 pagesPerformance Evaluation Supervisor FormJm uniteNo ratings yet
- CS Form No. 212 Attachment - Work Experience Sheet...Document3 pagesCS Form No. 212 Attachment - Work Experience Sheet...Jm uniteNo ratings yet
- UCO - GROUP CARE 360 APPLICATION FORM (Scheme For Customers of UCO Bank) (JULY-5th) - CompressedDocument2 pagesUCO - GROUP CARE 360 APPLICATION FORM (Scheme For Customers of UCO Bank) (JULY-5th) - CompressedRahulSinghNo ratings yet
- Mental Health Services Billing GuideDocument136 pagesMental Health Services Billing Guidemiranda criggerNo ratings yet
- Frameworks-International-Health ModelsDocument4 pagesFrameworks-International-Health ModelsVictor Hugo Loaiza SeguraNo ratings yet
- Knowledge, Awareness and Perception of Health Insurance Among Insured in A Tertiary Care HospitalDocument9 pagesKnowledge, Awareness and Perception of Health Insurance Among Insured in A Tertiary Care HospitalIAEME PublicationNo ratings yet
- 83-Article Text-122-1-10-20171114Document6 pages83-Article Text-122-1-10-20171114Zainut TholibinNo ratings yet
- Deloitte StudyDocument2 pagesDeloitte StudyRob PortNo ratings yet
- HSSQ Theory and VivaDocument134 pagesHSSQ Theory and VivaPooja FuloriaNo ratings yet
- Elements of Insurance ContractDocument10 pagesElements of Insurance ContractRohit SoniNo ratings yet
- Health Insurance Presentation. (Fn-26)Document19 pagesHealth Insurance Presentation. (Fn-26)m_dattaiasNo ratings yet
- 2022 Everise Executives Benefits GuideDocument56 pages2022 Everise Executives Benefits GuideEricaNo ratings yet
- Pre Test MentoringDocument2 pagesPre Test MentoringLevy Garcia SanchezNo ratings yet
- Medication Errors - Where Do They Happen - The Pharmaceutical JournalDocument7 pagesMedication Errors - Where Do They Happen - The Pharmaceutical JournalAre Pee EtcNo ratings yet
- Complete Healthcare Insurance Premium Chart for Universal Sompo General InsuranceDocument10 pagesComplete Healthcare Insurance Premium Chart for Universal Sompo General InsuranceNaveenraj SNo ratings yet
- PhilHealth Certificate Verifies Member ContributionsDocument1 pagePhilHealth Certificate Verifies Member ContributionsLanissa FerminNo ratings yet
- Hospital Service Quality AsDocument20 pagesHospital Service Quality AsNurulfitrahhafidNo ratings yet
- Passionate Doctor Seeks Scholarship to Improve Pakistani HealthcareDocument1 pagePassionate Doctor Seeks Scholarship to Improve Pakistani HealthcarebloomNo ratings yet
- Week 5 Healthcare Service PurchasingDocument21 pagesWeek 5 Healthcare Service Purchasingpwala5151No ratings yet
- Blandes Final DraftDocument53 pagesBlandes Final Draftjupiter stationeryNo ratings yet
- Star Health and Allied Insurance Company LimitedDocument2 pagesStar Health and Allied Insurance Company LimitedMr. RAJASEKHARNo ratings yet
- SUD Life Century RoyaleDocument4 pagesSUD Life Century RoyaleDivili PadmavathiNo ratings yet
- Insurance Importance For Senior CitizensDocument2 pagesInsurance Importance For Senior CitizensbfhfxNo ratings yet
- BioethicsDocument6 pagesBioethicsClarissa Anne TabaosaresNo ratings yet
- PHR Primer For Policymakers - Pnach345Document12 pagesPHR Primer For Policymakers - Pnach345andry budiarjoNo ratings yet
- Selection of Personal Injury Protection (PIP) Medical Coverage - Individual(s)Document6 pagesSelection of Personal Injury Protection (PIP) Medical Coverage - Individual(s)Doug RoyseNo ratings yet
- Organization Assessment and Readiness of EHR ImplementationDocument40 pagesOrganization Assessment and Readiness of EHR ImplementationDoni mustofa al MakiNo ratings yet
- 2023 Medical Sterilizer Promo DetailsDocument2 pages2023 Medical Sterilizer Promo DetailsVulcano JerezNo ratings yet
- Passenger Insurance: Your Ride With Rapido On 29 Apr 2022 at 07:23AM Is Now Insured!Document6 pagesPassenger Insurance: Your Ride With Rapido On 29 Apr 2022 at 07:23AM Is Now Insured!rahuljssstuNo ratings yet
- Endorsement Schedule: LC0000000619 Intermediary Code Name M/S.Policybazaar Insurance Brokers Private LimitedDocument1 pageEndorsement Schedule: LC0000000619 Intermediary Code Name M/S.Policybazaar Insurance Brokers Private LimitedPrakhar ShuklaNo ratings yet