You might also like
- Common Sports InjuryDocument71 pagesCommon Sports InjuryGlen Dizon100% (1)
- Jim's Surgery Progress Note TemplateDocument1 pageJim's Surgery Progress Note TemplatekatNo ratings yet
- Rife Consolidated Annotated Frequency List - EMR Labs, LLCDocument19 pagesRife Consolidated Annotated Frequency List - EMR Labs, LLCMatimba SimangoNo ratings yet
- Homeopathy for Cold Hands and FeetDocument9 pagesHomeopathy for Cold Hands and FeetsherazbthNo ratings yet
- Mark Klimek Full Nclex ReviewerDocument30 pagesMark Klimek Full Nclex ReviewerAlex BellNo ratings yet
- Blood Banking and Serology QuizDocument14 pagesBlood Banking and Serology QuizLyudmyla Gillego100% (3)
- Bronchopneumonia Case PresentationDocument17 pagesBronchopneumonia Case Presentationgandhialpit100% (1)
- Z Track Injection TechniqueDocument3 pagesZ Track Injection TechniquebunsokoyNo ratings yet
- Nursing Management of PatientDocument32 pagesNursing Management of PatientNoky KiaNo ratings yet
- Eritroderma RangkumanDocument4 pagesEritroderma RangkumanNisrinaNo ratings yet
- 101 Clinical Cases in Emergency Room Book PDFDocument1 page101 Clinical Cases in Emergency Room Book PDFHhaNo ratings yet
- Ncmb312 Rle:: Bachelor of Science in NursingDocument7 pagesNcmb312 Rle:: Bachelor of Science in NursingVAL ASHLIE ACEBAR100% (1)
- Ventilatory Limitations BC Ws 21Document29 pagesVentilatory Limitations BC Ws 21Eto Tamazashvili MiguelNo ratings yet
- Modul Interna Tropical MedicineDocument25 pagesModul Interna Tropical MedicineYifada SNo ratings yet
- 17.N. HTA - Boli Art Vene - TEV - SangerariDocument16 pages17.N. HTA - Boli Art Vene - TEV - SangerariAna MîndrilăNo ratings yet
- Record foundation settlement observations Hassyan Clean Coal Power PlantDocument1 pageRecord foundation settlement observations Hassyan Clean Coal Power PlantJoseph DzingiraiNo ratings yet
- Item:: E L E EDocument7 pagesItem:: E L E Eshahbaz HazardousNo ratings yet
- Scenario 3 exerciseDocument3 pagesScenario 3 exercisePeemnapat PhamornNo ratings yet
- Guest Lecture Hypertension NotesDocument4 pagesGuest Lecture Hypertension NotesKellyNo ratings yet
- APPENDICITISDocument1 pageAPPENDICITISAmber BlodduweddNo ratings yet
- 19.R. Pancreas - Cai BiliareDocument10 pages19.R. Pancreas - Cai BiliareAna MîndrilăNo ratings yet
- Controlling Asthma: Treatment Options and Management StepsDocument25 pagesControlling Asthma: Treatment Options and Management StepsDwi Esthi PutriNo ratings yet
- CVS 2 TableDocument2 pagesCVS 2 TablembdzNo ratings yet
- BRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISDocument3 pagesBRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISmarielleaudreeyNo ratings yet
- BedahDocument1 pageBedahLovely MeNo ratings yet
- 7.7 HematologyDocument11 pages7.7 HematologyGhianx Carlox PioquintoxNo ratings yet
- Notițe Curs Fiziologie FicatDocument5 pagesNotițe Curs Fiziologie FicatDaliNo ratings yet
- Routes_Of_Administration.pdfDocument1 pageRoutes_Of_Administration.pdfnazbeen.ahmadiNo ratings yet
- Tropikal MedicineDocument23 pagesTropikal MedicineJonathan ArielNo ratings yet
- MED2 - Spirometry: Key Parameters and Patterns (Restrictive vs ObstructiveDocument3 pagesMED2 - Spirometry: Key Parameters and Patterns (Restrictive vs ObstructivessasianNo ratings yet
- O2 Supply and Demand FrameworkDocument1 pageO2 Supply and Demand FrameworkrachelweinhardtNo ratings yet
- LP1 PTSC 10uzu C C1 Itp 0001 0Document33 pagesLP1 PTSC 10uzu C C1 Itp 0001 0Nguyễn Hoàng HảiNo ratings yet
- Scientific PosterDocument1 pageScientific PosterJa'far ShodiqNo ratings yet
- Marketing Business ProcessDocument2 pagesMarketing Business ProcessVhie SimatupangNo ratings yet
- Frog PDFDocument14 pagesFrog PDFrohitsharmakls3No ratings yet
- Evaluate PDFDocument3 pagesEvaluate PDFMc SantosNo ratings yet
- Real 2 Tower Indoor DAS - Neutral Host Proposal: /nfrastructureDocument12 pagesReal 2 Tower Indoor DAS - Neutral Host Proposal: /nfrastructureJhon GrandezNo ratings yet
- ריאותDocument61 pagesריאותLiav KfirNo ratings yet
- AsthmaDocument10 pagesAsthmaAnkit JonwalNo ratings yet
- PharmacologyDocument4 pagesPharmacologys748jNo ratings yet
- Physical ExamDocument7 pagesPhysical ExamNicole GayetaNo ratings yet
- OpthalmologyDocument6 pagesOpthalmologyeilyabashir315No ratings yet
- FinalsDocument14 pagesFinalsZarina AvesNo ratings yet
- PathologyDocument64 pagesPathology2021004207.garimaNo ratings yet
- CKD PathophyDocument1 pageCKD PathophyGinoTevesNo ratings yet
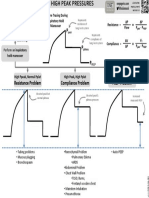
- VENT TROUBLESHOOTING: HIGH PEAK PRESSURESDocument1 pageVENT TROUBLESHOOTING: HIGH PEAK PRESSURESRonald MoralesNo ratings yet
- DIARRHEA CARE PLANDocument1 pageDIARRHEA CARE PLANRenty AgustikaNo ratings yet
- AclameDocument1 pageAclameMartin EullerNo ratings yet
- Standard Operating Procedure Matrix For Research Staff Training FilesDocument4 pagesStandard Operating Procedure Matrix For Research Staff Training FilesVanitha vashti100% (1)
- Sciencedirect SciencedirectDocument6 pagesSciencedirect SciencedirectLuis Alexander López AldanaNo ratings yet
- Interpretation of CPET PosterDocument1 pageInterpretation of CPET PosterczukmiklosNo ratings yet
- Biology 3Document1 pageBiology 3KacperCoghenNo ratings yet
- Schema VirusoDocument2 pagesSchema VirusoSabyna BurcaNo ratings yet
- PleuraDocument3 pagesPleuraAmrinder MaanNo ratings yet
- VbSeries Feature ComparisonDocument1 pageVbSeries Feature ComparisonmmmmNo ratings yet
- LiverDocument1 pageLiverstoragejoannamsvNo ratings yet
- Org Chem LabDocument3 pagesOrg Chem Labกรวรินทร์ ชำนาญกุลNo ratings yet
- Lab E Unknown Y Data AnalysisDocument5 pagesLab E Unknown Y Data Analysismirah.ej.gertzNo ratings yet
- Two-Phase Systems States of The Matter: MeeseDocument24 pagesTwo-Phase Systems States of The Matter: MeeseTung PhamNo ratings yet
- Anatomy Lower Limb by DR AzamDocument19 pagesAnatomy Lower Limb by DR AzamroulprayashNo ratings yet
- HZA-PS Leviat 20-EDocument24 pagesHZA-PS Leviat 20-Eeuric82No ratings yet
- Biology 4Document1 pageBiology 4Phimsiya ThongyooNo ratings yet
- Micro 22 RATIO by Clerky StubuDocument13 pagesMicro 22 RATIO by Clerky StubuJohn RamosNo ratings yet
- BronchiolitisDocument8 pagesBronchiolitisdrvaishnavishashiNo ratings yet
- CKD ROQ 1 120ktDocument17 pagesCKD ROQ 1 120ktarum gladysNo ratings yet
- Respiratory SystemDocument11 pagesRespiratory SystemU-MANNo ratings yet
- Wilson Tre - 1677 - ScannedDocument3 pagesWilson Tre - 1677 - ScannedZach EdwardsNo ratings yet
- ARDS UpdateDocument29 pagesARDS UpdatefathaNo ratings yet
- Image Husband-Quote-Heart-Soul - JPG Family LoveDocument1 pageImage Husband-Quote-Heart-Soul - JPG Family LoveNicole GayetaNo ratings yet
- Screenshot 2021-08-16 at 1.32.24 PMDocument1 pageScreenshot 2021-08-16 at 1.32.24 PMNicole GayetaNo ratings yet
- 79 Husband Quotes (2021)Document3 pages79 Husband Quotes (2021)Nicole GayetaNo ratings yet
- Im NotesDocument1 pageIm NotesNicole GayetaNo ratings yet
- Physical ExamDocument7 pagesPhysical ExamNicole GayetaNo ratings yet
- PEDIADocument1 pagePEDIANicole GayetaNo ratings yet
- STEMIDocument29 pagesSTEMIHemanthNo ratings yet
- Form Form M Student Health CertificateDocument4 pagesForm Form M Student Health CertificateAnindya Wisastra Inggas AriawanNo ratings yet
- OsgoodDocument8 pagesOsgooddiretoriacmbaNo ratings yet
- Livelife Homecare: Nurse's Daily Psychiatric Assessment ChecklistDocument2 pagesLivelife Homecare: Nurse's Daily Psychiatric Assessment ChecklistJames Trick Ocampo ValeraNo ratings yet
- Common Sports Injuries: August 2016Document8 pagesCommon Sports Injuries: August 2016Binte SajjadNo ratings yet
- Thesis Statement For Birth DefectsDocument6 pagesThesis Statement For Birth Defectsashleygomezalbuquerque100% (2)
- NATVNS Paediatric Glamorgan v7Document5 pagesNATVNS Paediatric Glamorgan v7Nie AfnyNo ratings yet
- Name: Chintiya Cahaya Putri NIM: P20637020008 Class: 1A Prodi: Diii RmikDocument37 pagesName: Chintiya Cahaya Putri NIM: P20637020008 Class: 1A Prodi: Diii RmikChintiya PutriNo ratings yet
- Solid and Cystic Lesion of PancreasDocument27 pagesSolid and Cystic Lesion of PancreasRabina PantaNo ratings yet
- Clopixol Patient Information Leaflet 2mg 10mg 20mg From Mind OrgDocument9 pagesClopixol Patient Information Leaflet 2mg 10mg 20mg From Mind OrgRevaz SurguladzeNo ratings yet
- Tinea VersicolorDocument2 pagesTinea VersicolorAchep WahyuNo ratings yet
- GP Kaunseling 2019 Isbn FinalDocument90 pagesGP Kaunseling 2019 Isbn FinalAtiqah RamzanNo ratings yet
- Congestive Heart Failure Case StudyDocument20 pagesCongestive Heart Failure Case StudyMegan100% (1)
- Iligan City Hospital 1Document3 pagesIligan City Hospital 1danny17phNo ratings yet
- Vol 27 No 1 April 2014 Medicinus 1Document68 pagesVol 27 No 1 April 2014 Medicinus 1Natasya DelarespitaNo ratings yet
- Advanced Assessment Chest Assessment and Auscultation: Base Hospital GroupDocument41 pagesAdvanced Assessment Chest Assessment and Auscultation: Base Hospital GroupdeebertoNo ratings yet
- Mitral Stenosis Etiology and TreatmentDocument19 pagesMitral Stenosis Etiology and TreatmentAdi TrisnoNo ratings yet
- Eating Disorders Reading AssignmentDocument2 pagesEating Disorders Reading AssignmentNasratullah sahebzadaNo ratings yet
- Aim Global Approved Product Prescription-8Document9 pagesAim Global Approved Product Prescription-8ZION SIONNo ratings yet
- Clarithromycin - Drug Information - UpToDate PDFDocument56 pagesClarithromycin - Drug Information - UpToDate PDFNaztasia 'ola' Flowerin BNo ratings yet
- Childhood-Onset SchizophreniaDocument20 pagesChildhood-Onset SchizophreniaAndrea SalazarNo ratings yet