You might also like
- Opthalmoloy PDFDocument10 pagesOpthalmoloy PDFdrshekarforyouNo ratings yet
- Glaucoma: Consultant OphthalmologistDocument45 pagesGlaucoma: Consultant OphthalmologistGladys MainaNo ratings yet
- Objective - Subjective Eye Examination-Referral System and When To ReferDocument56 pagesObjective - Subjective Eye Examination-Referral System and When To ReferClara Sainuka100% (1)
- 432 OSCE Revision File PDFDocument20 pages432 OSCE Revision File PDFReza Affandi MohamadNo ratings yet
- Anisman Acute Vision LossDocument68 pagesAnisman Acute Vision Lossarnol3090No ratings yet
- Fundoscopy N PDFDocument6 pagesFundoscopy N PDFshahid12333No ratings yet
- Flashes and Floaters: Ahmed Shahab M08082Document15 pagesFlashes and Floaters: Ahmed Shahab M08082Ahmed ShahabNo ratings yet
- Geraitric Examination of EyeDocument37 pagesGeraitric Examination of Eyetanishqa eye careNo ratings yet
- Approach To A Case of CataractDocument18 pagesApproach To A Case of CataractVineet GuptaNo ratings yet
- Pemeriksaan Dasar MataDocument103 pagesPemeriksaan Dasar Mataandhie_soyNo ratings yet
- Double Vision / Diplopia: Dr. R. Handoko Pratomo, SPMDocument94 pagesDouble Vision / Diplopia: Dr. R. Handoko Pratomo, SPMNefri TiawarmanNo ratings yet
- Introduction To Neuro-Ophthalmology: Raed Behbehani, MD FRCSCDocument50 pagesIntroduction To Neuro-Ophthalmology: Raed Behbehani, MD FRCSCMarvinson Hermogino AquinoNo ratings yet
- HYPERMETROPIA and Myopia PDFDocument55 pagesHYPERMETROPIA and Myopia PDFDrashti ChudasamaNo ratings yet
- Dr. Md. Yeamli Khan: Mbbs (Dhaka) Do (Du) Fcps (Ophth)Document50 pagesDr. Md. Yeamli Khan: Mbbs (Dhaka) Do (Du) Fcps (Ophth)Kawshik SahaNo ratings yet
- Uveitis & Ocular Immunology: Introductory Lecture SeriesDocument44 pagesUveitis & Ocular Immunology: Introductory Lecture SeriesAlinaBrinzaNo ratings yet
- Ocular Emergencies TraumaDocument35 pagesOcular Emergencies TraumaMochaLover100% (2)
- Eye Examination: Dr. Seng Serey / Prof .Kenn Freedman Prof - Kong PisethDocument78 pagesEye Examination: Dr. Seng Serey / Prof .Kenn Freedman Prof - Kong PisethSela KHNo ratings yet
- Ophthalmology - RetinaDocument15 pagesOphthalmology - RetinajbtcmdtjjvNo ratings yet
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
- Chapter 11 Eye & Vision DisordersDocument72 pagesChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSANo ratings yet
- Trauma To The GlobeDocument19 pagesTrauma To The Globejollyday90No ratings yet
- Neuro-Ophta EditedDocument97 pagesNeuro-Ophta EditedMarshet GeteNo ratings yet
- Common Ocular EmergenciesDocument33 pagesCommon Ocular EmergenciesMaimoona AimanNo ratings yet
- Common Ocular DisordersDocument108 pagesCommon Ocular DisordersKa SalvinNo ratings yet
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaDocument98 pagesUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- Acute Visual LossDocument10 pagesAcute Visual LossJim Jose AntonyNo ratings yet
- Vision Impairment 1Document59 pagesVision Impairment 1122ritik goyalNo ratings yet
- Physical Assessment Internal EyesDocument29 pagesPhysical Assessment Internal EyesDeeeeeNo ratings yet
- Sudden Loss of Vision & Optic NeuropathyDocument30 pagesSudden Loss of Vision & Optic NeuropathyIshak IzharNo ratings yet
- LECTURE 8 Vitreous - Peripheral Retina PathologyDocument60 pagesLECTURE 8 Vitreous - Peripheral Retina PathologyOknitaLasmainiNo ratings yet
- PSSS-1: Christian Rendy C Rendy Andhika Sulaeman Andrianto Susilo Theodorus SuwendiDocument30 pagesPSSS-1: Christian Rendy C Rendy Andhika Sulaeman Andrianto Susilo Theodorus SuwendiSulaeman Andrianto SusiloNo ratings yet
- Degenerative MyopiaDocument53 pagesDegenerative MyopiaNiloy BasakNo ratings yet
- Ocular Examination: F. Francis Ma. L. Cid, MDDocument62 pagesOcular Examination: F. Francis Ma. L. Cid, MDroacruzmdNo ratings yet
- Mata Tenang Visus Turun MendadakDocument34 pagesMata Tenang Visus Turun MendadakTanani 102014007No ratings yet
- Ophthalmoscopy and DiseaseMgmtDocument21 pagesOphthalmoscopy and DiseaseMgmtSheral AidaNo ratings yet
- Pediatric Ocular EmergenciesDocument71 pagesPediatric Ocular EmergenciesenzomontresolNo ratings yet
- Secondary Angle Closure GlaucomaDocument35 pagesSecondary Angle Closure GlaucomaAndriati NadhilaNo ratings yet
- Ophthalmology - GlaucomaDocument13 pagesOphthalmology - GlaucomajbtcmdtjjvNo ratings yet
- Additional Slide: Lapsus Lensa 1Document58 pagesAdditional Slide: Lapsus Lensa 1Bram UtamaNo ratings yet
- Retinal Detachment: DR - Ajai Agrawal Additional Professor Department of Ophthalmology A.I.I.M.S, RishikeshDocument58 pagesRetinal Detachment: DR - Ajai Agrawal Additional Professor Department of Ophthalmology A.I.I.M.S, RishikeshSrishti KhullarNo ratings yet
- P.E. - Eyes 2020 PDFDocument45 pagesP.E. - Eyes 2020 PDFAira Mae PenaredondoNo ratings yet
- Ophthalmology Emergencies - 2Document32 pagesOphthalmology Emergencies - 2navenNo ratings yet
- Management of Nystagmus - The Ophthalmologist S PerspectiveDocument55 pagesManagement of Nystagmus - The Ophthalmologist S PerspectiveZaras Yudisthira SagaNo ratings yet
- Ophthalmology EmergenciesDocument60 pagesOphthalmology Emergenciesasraf amirullahNo ratings yet
- Assessment and Management of Patients With Eye andDocument86 pagesAssessment and Management of Patients With Eye andEsmareldah Henry SirueNo ratings yet
- Glaucoma: Zarieh Dawn Novela Medicine 2Document41 pagesGlaucoma: Zarieh Dawn Novela Medicine 2Zari NovelaNo ratings yet
- Carotid Cavernous FistulaDocument51 pagesCarotid Cavernous FistulaShiva KumaranNo ratings yet
- Diskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanDocument73 pagesDiskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanalimustagialgiNo ratings yet
- Orientation, History Taking and ExaminationDocument77 pagesOrientation, History Taking and ExaminationMuhammad AwaisNo ratings yet
- Glaucoma: Defitaria Permatasari I11109005Document46 pagesGlaucoma: Defitaria Permatasari I11109005yusufharkianNo ratings yet
- Gradual Loss of Vision-Nurses - 065937Document73 pagesGradual Loss of Vision-Nurses - 065937CosbyNo ratings yet
- Phacoantigenic Response To Ruptured Lens Capsule: Clinicopathologic CaseDocument20 pagesPhacoantigenic Response To Ruptured Lens Capsule: Clinicopathologic Casefm_askaNo ratings yet
- 35 Golden Eye RulesDocument7 pages35 Golden Eye RulesJethro WuNo ratings yet
- 2019 Dr. Halida 1. Retinopati DiabetikafixDocument44 pages2019 Dr. Halida 1. Retinopati DiabetikafixLuthfia WardhaniNo ratings yet
- L8 Neuro-OphthalmologyDocument27 pagesL8 Neuro-OphthalmologySofíaGriggsNo ratings yet
- Cataract SenilisDocument54 pagesCataract Senilismayo djitroNo ratings yet
- Assessing Eyes and EarsDocument156 pagesAssessing Eyes and EarsHyacinth Jane Dela PeñaNo ratings yet
- New Microsoft PowerPoint PresentationDocument15 pagesNew Microsoft PowerPoint Presentationsarjak shahNo ratings yet
- Visual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsFrom EverandVisual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsNo ratings yet
- Suicide and Psychiatric Emergencies 14 04 2022Document50 pagesSuicide and Psychiatric Emergencies 14 04 2022MUBIRU SAMUEL EDWARDNo ratings yet
- Radiology of Obstetrics and GynaecologyDocument61 pagesRadiology of Obstetrics and GynaecologyMUBIRU SAMUEL EDWARDNo ratings yet
- Bipolar WriteupDocument13 pagesBipolar WriteupMUBIRU SAMUEL EDWARDNo ratings yet
- YR 4 Lecture Urogenital ImagingDocument59 pagesYR 4 Lecture Urogenital ImagingMUBIRU SAMUEL EDWARDNo ratings yet
- Introduction To Clinical RadiologyDocument38 pagesIntroduction To Clinical RadiologyMUBIRU SAMUEL EDWARDNo ratings yet
- Old Age PsychiatryDocument36 pagesOld Age PsychiatryMUBIRU SAMUEL EDWARDNo ratings yet
- Child AbuseDocument34 pagesChild AbuseMUBIRU SAMUEL EDWARDNo ratings yet
- Facial NerveDocument53 pagesFacial NerveMUBIRU SAMUEL EDWARDNo ratings yet
- SchizophreniaDocument17 pagesSchizophreniaMUBIRU SAMUEL EDWARDNo ratings yet
- Case 2Document1 pageCase 2MUBIRU SAMUEL EDWARDNo ratings yet
- SEPSISDocument19 pagesSEPSISMUBIRU SAMUEL EDWARDNo ratings yet
- Pratical Two ReportDocument13 pagesPratical Two ReportMUBIRU SAMUEL EDWARDNo ratings yet
- Case 1Document2 pagesCase 1MUBIRU SAMUEL EDWARDNo ratings yet
- STUDY DESIGNS AND VARIABLES - TumusiimeDocument41 pagesSTUDY DESIGNS AND VARIABLES - TumusiimeMUBIRU SAMUEL EDWARDNo ratings yet
- Pratical Two ReportDocument13 pagesPratical Two ReportMUBIRU SAMUEL EDWARDNo ratings yet
- Pharmacology QNSDocument2 pagesPharmacology QNSMUBIRU SAMUEL EDWARDNo ratings yet
- 00 - Introduction To Research Methods - BEHDocument36 pages00 - Introduction To Research Methods - BEHMUBIRU SAMUEL EDWARDNo ratings yet
- Simulation in Nursing and Midwifery Education: The WHO Regional Office For EuropeDocument38 pagesSimulation in Nursing and Midwifery Education: The WHO Regional Office For EuropeNiveniveNo ratings yet
- The Use of Isotretinoin in AcneDocument8 pagesThe Use of Isotretinoin in AcneMelisa Silvia SembiringNo ratings yet
- Spinal Subdural Hematoma Responsible For A Syndrome of The Tail of A Horse About A Case in The University Hospital Center of Guadeloupe and Review of LiteratureDocument4 pagesSpinal Subdural Hematoma Responsible For A Syndrome of The Tail of A Horse About A Case in The University Hospital Center of Guadeloupe and Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 3.implementing ERM ProgramDocument48 pages3.implementing ERM ProgramBernard BavoNo ratings yet
- The Last PsychDocument381 pagesThe Last PsychBen BeasleyNo ratings yet
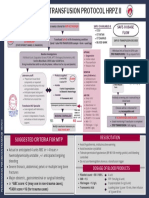
- Final Version MTP Poster 2022 2Document1 pageFinal Version MTP Poster 2022 2Hema Malini ArmugamNo ratings yet
- 4 - 24b - Media Advisory - P-SAG Parents Safety Advocacy GroupDocument4 pages4 - 24b - Media Advisory - P-SAG Parents Safety Advocacy GroupCBS News ColoradoNo ratings yet
- Incident Command System (Ics)Document3 pagesIncident Command System (Ics)Al VinNo ratings yet
- Soal Bhs. Inggris - Lat Utbk 1Document6 pagesSoal Bhs. Inggris - Lat Utbk 1Elriska TiffaniNo ratings yet
- Reproductive System of SwineDocument11 pagesReproductive System of SwineJaskhem LazoNo ratings yet
- Guidance Program Matrix For University TeachersDocument8 pagesGuidance Program Matrix For University TeachersAlexandra AlasNo ratings yet
- KLS - InST - ALL - Surgical Instrument Catalog 2nd EditionDocument722 pagesKLS - InST - ALL - Surgical Instrument Catalog 2nd EditionSuryaAtmajaya25% (4)
- Australian Beverages OHS FINALDocument41 pagesAustralian Beverages OHS FINALPauline VukiNo ratings yet
- Assessment Guide: CHCDIS007 Facilitate The Empowerment of People With DisabilityDocument31 pagesAssessment Guide: CHCDIS007 Facilitate The Empowerment of People With Disabilitydenis67% (3)
- Accounts of Practice Editorial Building Actionable Knowledge For Individuals and OrganisationsDocument3 pagesAccounts of Practice Editorial Building Actionable Knowledge For Individuals and Organisationsهادي قبيسيNo ratings yet
- 6.ento With Ans DR JADocument4 pages6.ento With Ans DR JAsubramaniam krishnamoorthiNo ratings yet
- Practical Research 2: 4Th QuarterDocument4 pagesPractical Research 2: 4Th Quartergamms upNo ratings yet
- Blueprint 4 Student Book Answer KeyDocument18 pagesBlueprint 4 Student Book Answer Keykyawzayar phyoNo ratings yet
- 2016 PJC J1 H1 EOY ExamDocument5 pages2016 PJC J1 H1 EOY ExamTimothy HandokoNo ratings yet
- Provisional Mop Up Selection List For Neet PG CPS 2021Document47 pagesProvisional Mop Up Selection List For Neet PG CPS 2021Rikesh K MhatreNo ratings yet
- LF2F Parental Consent and Waiver FormDocument6 pagesLF2F Parental Consent and Waiver FormDreSznNo ratings yet
- Po PCitesDocument62 pagesPo PCitesOusmanNo ratings yet
- Lesson 1 Nature of PsychologyDocument4 pagesLesson 1 Nature of PsychologyMariah A.No ratings yet
- Research MethodologyDocument18 pagesResearch MethodologyAhmed Saleh100% (1)
- NR 304 - Health Assessment II Head To Toe Assessment Final Script Introduction & AIDETDocument14 pagesNR 304 - Health Assessment II Head To Toe Assessment Final Script Introduction & AIDETA Sung100% (5)
- ORGANIZATIONAL BEHAVIOUR - The InternDocument4 pagesORGANIZATIONAL BEHAVIOUR - The InternVandanaNo ratings yet
- Indonesia-Korea Medical Roadshow 2023 (Seminar Program With Speaker Info)Document2 pagesIndonesia-Korea Medical Roadshow 2023 (Seminar Program With Speaker Info)Eko BudiarsoNo ratings yet
- Affirmations PDFDocument9 pagesAffirmations PDFAlex MoonNo ratings yet
- Health Benefits of Carrot JuiceDocument7 pagesHealth Benefits of Carrot JuiceSana KhanNo ratings yet
- CSR Activities of Ultratech Cement LTD.: Submitted By: Aneesh Kumar (21MBMA80) Sreyas Sathees Babu (21MBMA81)Document8 pagesCSR Activities of Ultratech Cement LTD.: Submitted By: Aneesh Kumar (21MBMA80) Sreyas Sathees Babu (21MBMA81)SreyasNo ratings yet