You might also like
- Philips Brilliance IctDocument38 pagesPhilips Brilliance IctJimmy CamonesNo ratings yet
- IVF ART Laboratory Equipment - IVF Lab Design SetupDocument30 pagesIVF ART Laboratory Equipment - IVF Lab Design Setup24x7emarketing100% (3)
- Infinix 8000Document7 pagesInfinix 8000Khan Kaka100% (1)
- Gen Ed Answer Key (A)Document7 pagesGen Ed Answer Key (A)Antonette Escarpe TorcinoNo ratings yet
- Physics Formulas and Symbols: Physics I Symbol FormulaDocument5 pagesPhysics Formulas and Symbols: Physics I Symbol Formulakaparthy100% (9)
- Construction Site PremisesDocument78 pagesConstruction Site PremisesDrew B Mrtnz67% (6)
- 11 - FORAGERS by Sam BoyerDocument106 pages11 - FORAGERS by Sam BoyerMurtaza HussainNo ratings yet
- Bionics: By:K.Saipradeep 160040422Document21 pagesBionics: By:K.Saipradeep 160040422pradeep 5959No ratings yet
- BionicsDocument24 pagesBionicsTANVI VERMA0% (1)
- Cochlear ImplantsDocument17 pagesCochlear Implantsyeabsira getachewNo ratings yet
- Vibrant Soundbridge ® Implantable Hearing System: Kristin M. Avitabile, MS, CCC-ADocument35 pagesVibrant Soundbridge ® Implantable Hearing System: Kristin M. Avitabile, MS, CCC-AsemiragaNo ratings yet
- Kunal KarnikDocument3 pagesKunal KarnikWatchwitz Technologies Pvt LtdNo ratings yet
- oticonDocument5 pagesoticonHamna AhmadNo ratings yet
- Introduction To Meril InnovationDocument49 pagesIntroduction To Meril InnovationLulu MizbahNo ratings yet
- Bicon HistoryDocument5 pagesBicon HistoryBicon Implant InaNo ratings yet
- Introduction to Biomaterials: Materials, Applications and DevelopmentDocument74 pagesIntroduction to Biomaterials: Materials, Applications and Developmentpayaliya91No ratings yet
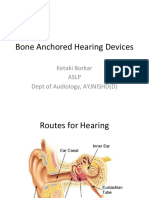
- Bone Anchored Hearing Devices: Ketaki Borkar Aslp Dept of Audiology, AYJNISHD (D)Document26 pagesBone Anchored Hearing Devices: Ketaki Borkar Aslp Dept of Audiology, AYJNISHD (D)shivaniNo ratings yet
- Medical Surgical NursingDocument38 pagesMedical Surgical NursingTripti PunNo ratings yet
- Hearing Aids PPT FinalDocument26 pagesHearing Aids PPT Finalchristina0% (1)
- Cochlear Implant Presentation: Jennifer CallawayDocument14 pagesCochlear Implant Presentation: Jennifer CallawayDev ROYNo ratings yet
- E64 HCD2017 AcousticsDocument41 pagesE64 HCD2017 AcousticsJoel GomezNo ratings yet
- Resource AspxDocument52 pagesResource AspxJustin QuintalNo ratings yet
- Hearing Aid Parts and Types of Hearing LossDocument8 pagesHearing Aid Parts and Types of Hearing LossHugh JacobsNo ratings yet
- Partnerships For Success: Corneal Transplant in The 21st CenturyDocument55 pagesPartnerships For Success: Corneal Transplant in The 21st CenturynellieauthorNo ratings yet
- Root Canal TreatmentDocument21 pagesRoot Canal TreatmentMary Noelyn Degoma100% (3)
- Camino ICP MonitorDocument2 pagesCamino ICP MonitorJuan Miguel AlemánNo ratings yet
- Clear 25Document25 pagesClear 25PZNo ratings yet
- Product PortfolioDocument8 pagesProduct PortfolioPrerna SharmaNo ratings yet
- Your Guide To Hearing AidsDocument20 pagesYour Guide To Hearing AidsMarhama FitrianiNo ratings yet
- BPS - The Biofunctional Prosthetic System PDFDocument20 pagesBPS - The Biofunctional Prosthetic System PDFVinay PandeyNo ratings yet
- Hearing Aids WidexDocument10 pagesHearing Aids WidexWidex Emirates Hearing CareNo ratings yet
- Pre Thesis Seminar - HospitalDocument7 pagesPre Thesis Seminar - HospitalAshis PattanaikNo ratings yet
- Emerging Technologies: Curs Actualitati in Ortopedie 3Document17 pagesEmerging Technologies: Curs Actualitati in Ortopedie 3Mariaa MariutssaNo ratings yet
- SPINE EU ENG ITA REV 07 31 05 2022 - Compressed 1Document32 pagesSPINE EU ENG ITA REV 07 31 05 2022 - Compressed 1Guo KangNo ratings yet
- Cochlear Implant Surgery - Cochlear Implants Surgery Hospitals IndiaDocument9 pagesCochlear Implant Surgery - Cochlear Implants Surgery Hospitals IndiaindiacarezNo ratings yet
- Bio MaterialsDocument13 pagesBio MaterialsPower RiderNo ratings yet
- Catheter InnovationsDocument2 pagesCatheter Innovationswww.elsdNo ratings yet
- Immediate Dentures - S2Document41 pagesImmediate Dentures - S2Nikita AggarwalNo ratings yet
- BPS+ +the+Biofunctional+Prosthetic+SystemDocument20 pagesBPS+ +the+Biofunctional+Prosthetic+SystemPravin Prathip JNo ratings yet
- Ab 3 01473 B Conveyer Belt BookletDocument6 pagesAb 3 01473 B Conveyer Belt BookletOmer ErgeanNo ratings yet
- Come With Us: It's The Way ForwardDocument8 pagesCome With Us: It's The Way ForwardJimmy AlexanderNo ratings yet
- Cochlear Implants Improve Speech Perception in a 66-Year-Old PatientDocument21 pagesCochlear Implants Improve Speech Perception in a 66-Year-Old PatientsurgpissNo ratings yet
- Engbusiness ProjectDocument19 pagesEngbusiness Projectapi-548943629No ratings yet
- AIS Learning Hearing AidsDocument2 pagesAIS Learning Hearing AidsElias Oktovianus HaulussyNo ratings yet
- Welcome To Your Digital Edition Of: Bio IT World Magazine!Document54 pagesWelcome To Your Digital Edition Of: Bio IT World Magazine!TamNo ratings yet
- PDF SlideshareDocument40 pagesPDF SlideshareMehri AishaNo ratings yet
- Detartraj ManualDocument4 pagesDetartraj ManualMiruna CojocaruNo ratings yet
- CHCF Seminar Whitepapers FINALDocument37 pagesCHCF Seminar Whitepapers FINALJoanna AngelopoulouNo ratings yet
- Bio ChipsDocument20 pagesBio ChipsArcher CasioNo ratings yet
- Basic Surgical Techniques For Endosseous Implant PlacementDocument101 pagesBasic Surgical Techniques For Endosseous Implant PlacementAnshuman Dwivedi100% (2)
- MaheshDocument15 pagesMaheshbabblubabblu295No ratings yet
- Literature Reading on Cochlear ImplantsDocument35 pagesLiterature Reading on Cochlear ImplantsOke KadarullahNo ratings yet
- Voluson S10: Extraordinary VisionDocument8 pagesVoluson S10: Extraordinary VisionNam LeNo ratings yet
- Creation of Competence Center, How To Bring Biotechnology Into The BusinessDocument18 pagesCreation of Competence Center, How To Bring Biotechnology Into The BusinessinfooncoNo ratings yet
- Wilcoxon Short Form Catalog-2018Document36 pagesWilcoxon Short Form Catalog-2018Dhananjay B KNo ratings yet
- Philadelphia Cervical Collar PDFDocument2 pagesPhiladelphia Cervical Collar PDFvivekNo ratings yet
- Al-Assaf dental implant notesDocument7 pagesAl-Assaf dental implant notesmohammed alsaadNo ratings yet
- VISIONS17Document52 pagesVISIONS17mohamed boufasNo ratings yet
- Project Spotlight: Philips Applied Technologies 22 Ways To Apply TechnologyDocument32 pagesProject Spotlight: Philips Applied Technologies 22 Ways To Apply Technologyapi-26400825No ratings yet
- Ge PresentationDocument42 pagesGe PresentationAbdoulaye LoNo ratings yet
- Kaplan PDFDocument51 pagesKaplan PDFNic KnightNo ratings yet
- Gita Product Catlog - 2018Document31 pagesGita Product Catlog - 2018Rohira YashNo ratings yet
- HA & BrainDocument100 pagesHA & BrainGhada WageihNo ratings yet
- Assessing and Monitoring The Progress of Deaf Children and Young PeopleDocument174 pagesAssessing and Monitoring The Progress of Deaf Children and Young PeopleGhada WageihNo ratings yet
- Brain Blood SupplyDocument11 pagesBrain Blood SupplyGhada WageihNo ratings yet
- BC HaDocument140 pagesBC HaGhada WageihNo ratings yet
- Assessing Verbal Working Memory in ChildrenDocument10 pagesAssessing Verbal Working Memory in ChildrenGhada WageihNo ratings yet
- Vestibular Consequences in CIDocument46 pagesVestibular Consequences in CIGhada WageihNo ratings yet
- BPPVDocument26 pagesBPPVGhada WageihNo ratings yet
- BHI Guide To Tinnitus PDFDocument14 pagesBHI Guide To Tinnitus PDFGhada WageihNo ratings yet
- THI QuestionnaireDocument1 pageTHI QuestionnaireGhada WageihNo ratings yet
- VRBQ Scoring GuideDocument1 pageVRBQ Scoring GuideGhada WageihNo ratings yet
- Assessing Dizziness and its Impact with the DHI QuestionnaireDocument2 pagesAssessing Dizziness and its Impact with the DHI QuestionnaireGhada WageihNo ratings yet
- Tinnitus ASHADocument3 pagesTinnitus ASHAGhada WageihNo ratings yet
- Motion (Travel) SicknessDocument3 pagesMotion (Travel) SicknessGhada WageihNo ratings yet
- 6-Digital Circuit & ADCDocument8 pages6-Digital Circuit & ADCGhada WageihNo ratings yet
- Anatomy & Physiology Vestibular SystemDocument44 pagesAnatomy & Physiology Vestibular SystemGhada WageihNo ratings yet
- Inner Ear AnatomyDocument103 pagesInner Ear AnatomyGhada WageihNo ratings yet
- Balance and Dizziness QuestionaireDocument5 pagesBalance and Dizziness QuestionaireGhada WageihNo ratings yet
- Ear EmbryologyDocument34 pagesEar EmbryologyGhada WageihNo ratings yet
- A Headache Is Defined As A Pain in The Head or Upper Neck.: Migraine HeadachesDocument5 pagesA Headache Is Defined As A Pain in The Head or Upper Neck.: Migraine HeadachesGhada WageihNo ratings yet
- ABR Instruction SheetDocument1 pageABR Instruction SheetGhada WageihNo ratings yet
- Enlarged Vestibular AqueductDocument86 pagesEnlarged Vestibular AqueductGhada WageihNo ratings yet
- Comparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010Document6 pagesComparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010mtanaydinNo ratings yet
- Cell Structure ActivityDocument4 pagesCell Structure ActivitysharksiedNo ratings yet
- Demonstration POSTNATAL EXAMINATION Easy WayDocument9 pagesDemonstration POSTNATAL EXAMINATION Easy Wayjyoti singhNo ratings yet
- Errata Introduction To Quantum Mechanics, David Griffiths, 2nd Ed.Document3 pagesErrata Introduction To Quantum Mechanics, David Griffiths, 2nd Ed.Marcel BezerraNo ratings yet
- Memorial Garden Policies and Guidelines St. Mark's Episcopal Church, Raleigh, North CarolinaDocument7 pagesMemorial Garden Policies and Guidelines St. Mark's Episcopal Church, Raleigh, North Carolinaestela maria dulaganNo ratings yet
- Let Us Be HappyDocument2 pagesLet Us Be HappyMarjule DechavezNo ratings yet
- Wily Walnut BRAIN SQUEEZERS Vol.1Document116 pagesWily Walnut BRAIN SQUEEZERS Vol.1tarzaman88% (8)
- Petford & Atherton., 1996Document31 pagesPetford & Atherton., 1996Ivan Hagler Becerra VasquezNo ratings yet
- Differences in Left Ventricular and Left Atrial FuDocument10 pagesDifferences in Left Ventricular and Left Atrial FueugeniaNo ratings yet
- Beyond Schein DentalDocument9 pagesBeyond Schein DentaltomdietzlerNo ratings yet
- Metal Enameling: Arts & CommunicationDocument15 pagesMetal Enameling: Arts & CommunicationAnjali DavidNo ratings yet
- Acute Severe Asthma Hospital ManagementDocument1 pageAcute Severe Asthma Hospital ManagementItharshan IndreswaranNo ratings yet
- Sample Article Used by MeDocument14 pagesSample Article Used by MeMagnum OpusNo ratings yet
- Pantheon-Katalog Eng WebDocument16 pagesPantheon-Katalog Eng WebJoe DoeNo ratings yet
- Well Rounded.: 360 CassetteDocument12 pagesWell Rounded.: 360 CassetteMonty Va Al MarNo ratings yet
- 5988-4082EN Designers GuidDocument82 pages5988-4082EN Designers GuidAndreaNo ratings yet
- Chapter 14 Chemical EquilibriumDocument29 pagesChapter 14 Chemical EquilibriumlynloeNo ratings yet
- PSUTIL Documentation for Monitoring System ResourcesDocument77 pagesPSUTIL Documentation for Monitoring System ResourcesImam RiadiNo ratings yet
- Tabcalcs.com general equations sheetDocument2 pagesTabcalcs.com general equations sheetRamadan RashadNo ratings yet
- The Image of The CityDocument17 pagesThe Image of The CityMay Rose ParagasNo ratings yet
- NTPC Training ReportDocument83 pagesNTPC Training ReportAbhishek Mittal100% (2)
- AABB Accredited DNA Testing FacilitiesDocument2 pagesAABB Accredited DNA Testing Facilitiesjosueduran75No ratings yet
- Textile Internship Report AlokDocument39 pagesTextile Internship Report AlokRahul TelangNo ratings yet
- Mohair FiberDocument33 pagesMohair FiberMuhammad Ahsan AftabNo ratings yet
- Chapter-1: Introduction of The StudyDocument21 pagesChapter-1: Introduction of The StudyViswanathanNo ratings yet
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet