You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rule On Commitment of ChildrenDocument6 pagesRule On Commitment of ChildrenDawiNo ratings yet
- Superfreakonomics Summarize ChaptersDocument22 pagesSuperfreakonomics Summarize ChaptersLoik-mael NysNo ratings yet
- Capitalism Vs Socialism 1Document7 pagesCapitalism Vs Socialism 1Rohin AroraNo ratings yet
- Enclosed/ Confined Space Entry Permit: As Per ISGOTT - Chapter 10Document4 pagesEnclosed/ Confined Space Entry Permit: As Per ISGOTT - Chapter 10irakli100% (2)
- Topic 5: Handling Stress: ObjectivesDocument5 pagesTopic 5: Handling Stress: ObjectivesfarhanjahariNo ratings yet
- Bsbcmm401 Task 1 & 2 (Tal)Document16 pagesBsbcmm401 Task 1 & 2 (Tal)Shar KhanNo ratings yet
- Cinimatic Unisystem CompiledDocument189 pagesCinimatic Unisystem CompiledAnonymous jSTkQVC27bNo ratings yet
- Fluid and Electrolyte Therapy During Vomiting and DiarrheaDocument22 pagesFluid and Electrolyte Therapy During Vomiting and Diarrheafernin96No ratings yet
- Central Pontine Myelinolysis in A Patient With Methamphetamine AbuseDocument10 pagesCentral Pontine Myelinolysis in A Patient With Methamphetamine Abusefernin96No ratings yet
- Lethal Diquat Poisoning Manifesting As Central Pontine Myelinolysis and Acute Kidney Injury - A Case Report and Literature ReviewDocument3 pagesLethal Diquat Poisoning Manifesting As Central Pontine Myelinolysis and Acute Kidney Injury - A Case Report and Literature Reviewfernin96No ratings yet
- Central Pontine Myelinolysis in Pregnancy - A Case of Rare OccurrenceDocument5 pagesCentral Pontine Myelinolysis in Pregnancy - A Case of Rare Occurrencefernin96No ratings yet
- Noninvasive Ventilation in Preterm Infants: Factors Influencing Weaning Decisions and The Role of The Silverman-Andersen ScoreDocument18 pagesNoninvasive Ventilation in Preterm Infants: Factors Influencing Weaning Decisions and The Role of The Silverman-Andersen Scorefernin96No ratings yet
- ScoreDocument7 pagesScorefernin96No ratings yet
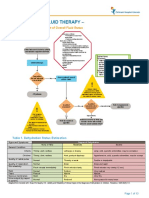
- Intravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid StatusDocument13 pagesIntravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid Statusfernin96No ratings yet
- SA PerformanceDocument8 pagesSA Performancefernin96No ratings yet
- Mekala Lakshman - Google Scholar Citations PDFDocument3 pagesMekala Lakshman - Google Scholar Citations PDFMekala LakshmanNo ratings yet
- Definition of TermsDocument4 pagesDefinition of TermsKenneth SastadoNo ratings yet
- Customer Price List - Outer NutritionDocument2 pagesCustomer Price List - Outer NutritionsandeepNo ratings yet
- Pediatric Pharyngotonsillitis Sore ThroatDocument5 pagesPediatric Pharyngotonsillitis Sore Throatdef_10No ratings yet
- The Lessons of Quantec Recommendations For Reporting and Gathering Data On Dose-Volume Dependencies of Treatment OutcomeDocument6 pagesThe Lessons of Quantec Recommendations For Reporting and Gathering Data On Dose-Volume Dependencies of Treatment OutcomeCarina Isabel Bento Marques CoelhoNo ratings yet
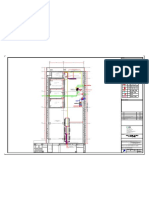
- REVISED HVAC Layout For DC3 Annex - 4F Roof - 08.10.2022.dwg-Roof HVACDocument1 pageREVISED HVAC Layout For DC3 Annex - 4F Roof - 08.10.2022.dwg-Roof HVACaamnagroup officeNo ratings yet
- Information Systems and Community DiagnosisDocument26 pagesInformation Systems and Community DiagnosisLena TresnawatiNo ratings yet
- Introduction To Autism PDFDocument50 pagesIntroduction To Autism PDFiindahlubisNo ratings yet
- Adjustment DisordersDocument2 pagesAdjustment DisordersIsabel CastilloNo ratings yet
- Cover Letter For EportfolioDocument2 pagesCover Letter For Eportfolioapi-231487081No ratings yet
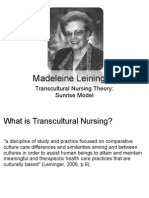
- Transcultural Nursing Nur324Document18 pagesTranscultural Nursing Nur324lidyaNo ratings yet
- Delhi Victims Compensation Scheme 2018Document52 pagesDelhi Victims Compensation Scheme 2018Kiryuu KanameNo ratings yet
- Risk AssesmentDocument2 pagesRisk AssesmentChristopher Stewart0% (1)
- Mqa203t Mpharm Summer 2021Document1 pageMqa203t Mpharm Summer 2021Koushal DhamijaNo ratings yet
- Pediatric PneumoniaDocument12 pagesPediatric PneumoniaKrystal Migo Denolo ContrerasNo ratings yet
- Aquaculture: Junior Farmer Field and Life School - Facilitator's GuideDocument50 pagesAquaculture: Junior Farmer Field and Life School - Facilitator's GuideJuhainah C. GuroNo ratings yet
- The Scientific Facts About WaterDocument7 pagesThe Scientific Facts About WaterNizam HasniNo ratings yet
- Analysis of Various Effects of Web Serie PDFDocument15 pagesAnalysis of Various Effects of Web Serie PDFAayush Sinha100% (1)
- Ketamine Can Be Produced by Pochonia Chlamydosporia - An Old Molecule and A New AnthelminticDocument9 pagesKetamine Can Be Produced by Pochonia Chlamydosporia - An Old Molecule and A New AnthelminticHamilton MorrisNo ratings yet
- 131-msds 2014Document11 pages131-msds 2014ivan_kenzo1290No ratings yet
- Intermittent FastingDocument7 pagesIntermittent FastingJohnny KeeverNo ratings yet
- Kelat AsennusalustatDocument138 pagesKelat AsennusalustatJose MolinaNo ratings yet
- Abstrak Asmiha 2Document1 pageAbstrak Asmiha 2Indrawan MataramNo ratings yet