You might also like
- Test Bank For Comprehensive Perinatal and Pediatric Respiratory Care 4th Edition by WhitakerDocument6 pagesTest Bank For Comprehensive Perinatal and Pediatric Respiratory Care 4th Edition by WhitakerMargaret Mobley100% (28)
- PALS Study Guide Short FormDocument11 pagesPALS Study Guide Short FormLenTheRN88% (8)
- Wright Et Al 2022 PDFDocument9 pagesWright Et Al 2022 PDFRadu CiprianNo ratings yet
- 444 FullDocument10 pages444 FullCalvin AffendyNo ratings yet
- SA PerformanceDocument8 pagesSA Performancefernin96No ratings yet
- DANI 2012 - Surfactant Replacement in Preterm Infants With RDSDocument4 pagesDANI 2012 - Surfactant Replacement in Preterm Infants With RDSRafael JustinoNo ratings yet
- IJN - Volume 11 - Issue 4 - Pages 50-56nbnDocument7 pagesIJN - Volume 11 - Issue 4 - Pages 50-56nbnfitriNo ratings yet
- New Developments in Neonatal Respiratory MenagmentDocument7 pagesNew Developments in Neonatal Respiratory MenagmentTin TomašićNo ratings yet
- Background: Corresponding AuthorDocument8 pagesBackground: Corresponding AuthorPratiwi UmbohNo ratings yet
- Causes and Outcomes of Respiratory Distress in NeonatesDocument8 pagesCauses and Outcomes of Respiratory Distress in NeonatesMohammad AlmuhaiminNo ratings yet
- Jurnal Pubme 1 RdsDocument13 pagesJurnal Pubme 1 Rdsriri risna aNo ratings yet
- Guidelines For Surfactant Replacement Therapy in Neonates Canadian Paediatric SocietyDocument8 pagesGuidelines For Surfactant Replacement Therapy in Neonates Canadian Paediatric SocietyTiwi QiraNo ratings yet
- Evaluation of Gastric Aspirate Shake Test in Predicting Surfactant Need in Preterm Infants With Neonatal Respiratory Distress Syndrome A Cross-Sectional StudyDocument9 pagesEvaluation of Gastric Aspirate Shake Test in Predicting Surfactant Need in Preterm Infants With Neonatal Respiratory Distress Syndrome A Cross-Sectional StudyVita DesriantiNo ratings yet
- WRIGHT 2016 - Continuous Positive Airway Pressure To Prevent Neonatal Lung InjuryDocument10 pagesWRIGHT 2016 - Continuous Positive Airway Pressure To Prevent Neonatal Lung InjuryRafael JustinoNo ratings yet
- Efficacy of Non-Invasive Respiratory Support Modes For Primary Respiratory Support in Preterm Neonates With Respiratory Distress Syndrome Systematic Review and Network Meta-AnalysisDocument24 pagesEfficacy of Non-Invasive Respiratory Support Modes For Primary Respiratory Support in Preterm Neonates With Respiratory Distress Syndrome Systematic Review and Network Meta-Analysisalan tomeNo ratings yet
- Canadian Guidelines 2021Document7 pagesCanadian Guidelines 2021Radu CiprianNo ratings yet
- Guidelines For Surfactant Replacement Therapy in NeonatesDocument7 pagesGuidelines For Surfactant Replacement Therapy in NeonatesFer45No ratings yet
- Pregnancy Hypertension: SciencedirectDocument7 pagesPregnancy Hypertension: SciencedirectRolando TintayaNo ratings yet
- Journal Club: Surfactant Therapy in Premature InfantsDocument44 pagesJournal Club: Surfactant Therapy in Premature InfantsSubash PaudealNo ratings yet
- Pi Is 1875957219305510Document10 pagesPi Is 1875957219305510madimadi11No ratings yet
- Journal Homepage: - : Manuscript HistoryDocument5 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- UntitledDocument24 pagesUntitledBella FebriantiNo ratings yet
- Simorangkir (2021) - DONEDocument13 pagesSimorangkir (2021) - DONEMaya HammoudNo ratings yet
- 2174 8646 1 PBDocument5 pages2174 8646 1 PBKiran PantheeNo ratings yet
- New Modes of Surfactant Delivery - 2022 - Paediatric Respiratory ReviewsDocument6 pagesNew Modes of Surfactant Delivery - 2022 - Paediatric Respiratory ReviewsEduardo Rios DuboisNo ratings yet
- Reanimacion NeonatalDocument6 pagesReanimacion NeonatalDaniela AraujoNo ratings yet
- The Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesDocument5 pagesThe Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesJehangir AllamNo ratings yet
- Home-Made Continuous Positive Airways Pressure Device May Reduce Mortality in Neonates With Respiratory Distress in Low-Resource SettingDocument5 pagesHome-Made Continuous Positive Airways Pressure Device May Reduce Mortality in Neonates With Respiratory Distress in Low-Resource SettingNovi AryandaNo ratings yet
- Cpap Vs SurfactanteDocument10 pagesCpap Vs SurfactanteAngelicia Varela MuñozNo ratings yet
- 2010 Early CPAP Vs Surfactant in EPTI NEJMDocument10 pages2010 Early CPAP Vs Surfactant in EPTI NEJMFiorella VilcaNo ratings yet
- Jurnal Eliminating Risk IntubeDocument14 pagesJurnal Eliminating Risk IntubewilmaNo ratings yet
- The Effect of Extended Continuous Positive Airway Pressure On Changes in Lung Volumes in Stable Premature Infants A Randomized Controlled TrialDocument15 pagesThe Effect of Extended Continuous Positive Airway Pressure On Changes in Lung Volumes in Stable Premature Infants A Randomized Controlled Trialblufire78No ratings yet
- Alaiyan 2017Document5 pagesAlaiyan 2017adiNo ratings yet
- Bookshelf NBK550970Document17 pagesBookshelf NBK550970Lucas WillianNo ratings yet
- Nasal Anthropometry Among Indian NeonatesDocument5 pagesNasal Anthropometry Among Indian NeonatesPreethi KarthikeyanNo ratings yet
- Extubacion Neo Cuando Como 14Document8 pagesExtubacion Neo Cuando Como 14valentina rojasNo ratings yet
- Diagnostic Value of Gastric Shake Test For Hyaline Membrane Disease in Preterm InfantDocument7 pagesDiagnostic Value of Gastric Shake Test For Hyaline Membrane Disease in Preterm InfantJonathan JonesNo ratings yet
- 36 Update On Ventilatory Management of Extremely Preterm InfantsDocument9 pages36 Update On Ventilatory Management of Extremely Preterm Infantsema moralesNo ratings yet
- 693 FullDocument12 pages693 FullGilmer alvarez floresNo ratings yet
- Evidence-Based Practices For The Fetal To Newborn TransitionDocument11 pagesEvidence-Based Practices For The Fetal To Newborn TransitionAya YayaNo ratings yet
- Journal Pone 0000192Document5 pagesJournal Pone 0000192TriponiaNo ratings yet
- Mechanical Ventilation of The Premature NeonateDocument16 pagesMechanical Ventilation of The Premature NeonateHaitham HafezNo ratings yet
- Guler Et Coll (2020) - DONEDocument8 pagesGuler Et Coll (2020) - DONEMaya HammoudNo ratings yet
- Prediction of Extubation Readiness Using Lung Ultrasound in Preterm InfantsDocument8 pagesPrediction of Extubation Readiness Using Lung Ultrasound in Preterm InfantsAlexandra NemesNo ratings yet
- 589-Article Text-1298-1-10-20220830 PDFDocument12 pages589-Article Text-1298-1-10-20220830 PDFBella FebriantiNo ratings yet
- Early Predictors For Intubation-Surfactant-Extubation Failure in Preterm Infants With Neonatal Respiratory Distress Syndrome: A Systematic ReviewDocument13 pagesEarly Predictors For Intubation-Surfactant-Extubation Failure in Preterm Infants With Neonatal Respiratory Distress Syndrome: A Systematic ReviewPhilipe VieiraNo ratings yet
- Skin To SkinDocument9 pagesSkin To SkinAsiatiNo ratings yet
- SDR Segun EdadDocument9 pagesSDR Segun EdadLuzbenia ChaparroNo ratings yet
- Admission of Term Infants To The NicuDocument6 pagesAdmission of Term Infants To The NicucarlsonrenovatioNo ratings yet
- 2017-Journal of Paediatrics and Child HealthDocument1 page2017-Journal of Paediatrics and Child HealthAna SopaNo ratings yet
- Diagnostic Value of Gastric Shake Test For Hyaline Membrane Disease in Preterm InfantDocument6 pagesDiagnostic Value of Gastric Shake Test For Hyaline Membrane Disease in Preterm InfantNovia KurniantiNo ratings yet
- Does Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?Document8 pagesDoes Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?faikaoesmaniaNo ratings yet
- ProneDocument8 pagesPronesophiaNo ratings yet
- Lung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFDocument8 pagesLung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFcesar juarezNo ratings yet
- Pediatrics 1001 (Final)Document5 pagesPediatrics 1001 (Final)Paul HartingNo ratings yet
- Journal NicuDocument4 pagesJournal NicuMargaret LlavorNo ratings yet
- Prone Positioning in Severe Acute Respiratory Distress SyndromeDocument4 pagesProne Positioning in Severe Acute Respiratory Distress SyndromeJholo AlvaradoNo ratings yet
- Immediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisDocument9 pagesImmediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisBelén María Vega AladueñaNo ratings yet
- Respiratory Distress Syndrome of The Newborn JCG0086 v3Document17 pagesRespiratory Distress Syndrome of The Newborn JCG0086 v3meutia salsabilaNo ratings yet
- Prevention of Bronchopulmonary Dysplasia A Summary of Evidence Based StrategiesDocument15 pagesPrevention of Bronchopulmonary Dysplasia A Summary of Evidence Based StrategiesMatias LoreiroNo ratings yet
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- Lethal Diquat Poisoning Manifesting As Central Pontine Myelinolysis and Acute Kidney Injury - A Case Report and Literature ReviewDocument3 pagesLethal Diquat Poisoning Manifesting As Central Pontine Myelinolysis and Acute Kidney Injury - A Case Report and Literature Reviewfernin96No ratings yet
- Fluid and Electrolyte Therapy During Vomiting and DiarrheaDocument22 pagesFluid and Electrolyte Therapy During Vomiting and Diarrheafernin96No ratings yet
- Central Pontine Myelinolysis in A Patient With Methamphetamine AbuseDocument10 pagesCentral Pontine Myelinolysis in A Patient With Methamphetamine Abusefernin96No ratings yet
- Central Pontine Myelinolysis in Pregnancy - A Case of Rare OccurrenceDocument5 pagesCentral Pontine Myelinolysis in Pregnancy - A Case of Rare Occurrencefernin96No ratings yet
- Central Pontine Myelinolysis - StatPearlsDocument9 pagesCentral Pontine Myelinolysis - StatPearlsfernin96No ratings yet
- ScoreDocument7 pagesScorefernin96No ratings yet
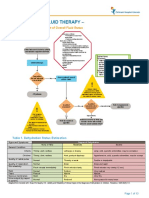
- Intravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid StatusDocument13 pagesIntravenous Fluid Therapy - : ALGORITHM 1. Assessment of Overall Fluid Statusfernin96No ratings yet
- Ficha Técnica Lubricante Omega 73Document12 pagesFicha Técnica Lubricante Omega 73juan felipe diazgranados santosNo ratings yet
- DEPED PFA Module 2 Self GuidedDocument3 pagesDEPED PFA Module 2 Self GuidedLrac Sirad TrinidadNo ratings yet
- Basic Mechanical Ventilation 2016Document67 pagesBasic Mechanical Ventilation 2016dragon66No ratings yet
- Science Grade 9 Learners MaterialDocument28 pagesScience Grade 9 Learners MaterialCris MarquisesNo ratings yet
- Science: Weekly Learning GuideDocument7 pagesScience: Weekly Learning GuideEdith LopoNo ratings yet
- How The Human Heart Works PDFDocument2 pagesHow The Human Heart Works PDFGerard AyalaNo ratings yet
- A Doctor View of The CrucifixionDocument5 pagesA Doctor View of The CrucifixiontimothjohnNo ratings yet
- Vier Cylinders 2022Document5 pagesVier Cylinders 2022sobheysaidNo ratings yet
- Jurnal Erisanti Octavia R PDFDocument8 pagesJurnal Erisanti Octavia R PDFErisanti OctaviaNo ratings yet
- Kebersihan Tangan, APD, Peralatan Pasien, Dan Linen 16-2-2023 - CompressedDocument70 pagesKebersihan Tangan, APD, Peralatan Pasien, Dan Linen 16-2-2023 - CompressedSaripa TalaohuNo ratings yet
- Final Content ET Intubation 1Document27 pagesFinal Content ET Intubation 1Debipriya MistryNo ratings yet
- Bse547 Ass1Document7 pagesBse547 Ass1hohi chanNo ratings yet
- CPR Ratio For Adults, Children, and InfantsDocument14 pagesCPR Ratio For Adults, Children, and InfantsAnonymous FCOOcnNo ratings yet
- Simple Schematic Diagram of PneumoniaDocument1 pageSimple Schematic Diagram of PneumoniaJason A. AdoyoganNo ratings yet
- Inhaler Technique For People With Asthma or COPD: See Inside For ChecklistsDocument12 pagesInhaler Technique For People With Asthma or COPD: See Inside For ChecklistsSukainah AL-AbkaryNo ratings yet
- ĐỀ THI THỬ THPTQG THÁNG 2 2023-2024 (Online)Document6 pagesĐỀ THI THỬ THPTQG THÁNG 2 2023-2024 (Online)Vy TuongNo ratings yet
- (LEGMED-FM-PPT) 2.02a Asphyxial DeathsDocument76 pages(LEGMED-FM-PPT) 2.02a Asphyxial DeathsAl Giorgio SyNo ratings yet
- Hesi Med Surg Study GuideDocument1 pageHesi Med Surg Study GuideGeorgeNo ratings yet
- Basic Modes of MVDocument37 pagesBasic Modes of MVLuis LopezNo ratings yet
- CHRA Form - For Distillation IsopropylDocument2 pagesCHRA Form - For Distillation Isopropylcsgo account100% (1)
- Worksheet - Respiratory SystemDocument8 pagesWorksheet - Respiratory SystemDhen MarcNo ratings yet
- First Aid in Case of ChokingDocument10 pagesFirst Aid in Case of ChokingMaria FilipNo ratings yet
- 720 Msds-Dromus BDocument8 pages720 Msds-Dromus Bmsjadm MegasuplindoNo ratings yet
- Safety Data Sheet: TeppekiDocument12 pagesSafety Data Sheet: TeppekiSloNo ratings yet
- Match The Wh-Question Words With Its MeaningDocument1 pageMatch The Wh-Question Words With Its MeaningDavid PolentinoNo ratings yet
- THANATOLOGYDocument53 pagesTHANATOLOGYsudharsan100% (2)
- Breathing Techniques For ExerciseDocument5 pagesBreathing Techniques For ExerciseHamilton DurantNo ratings yet
- Msds Tesa 60020 60021 Spray Glue PermanentDocument10 pagesMsds Tesa 60020 60021 Spray Glue Permanentemre sönmezNo ratings yet