You might also like
- Deep Venous Thrombosis Diferential DiagnosisDocument8 pagesDeep Venous Thrombosis Diferential DiagnosisBeby Dwi Lestari BajryNo ratings yet
- Large and Bleeding Gastroduodenal Artery Aneurysm 2024 International JournalDocument5 pagesLarge and Bleeding Gastroduodenal Artery Aneurysm 2024 International JournalRonald QuezadaNo ratings yet
- Direct Evidence of Endothelial Injury in Acute Myocardial Infarction and Unstable Angina by Demonstration of Circulating Endothelial CellsDocument8 pagesDirect Evidence of Endothelial Injury in Acute Myocardial Infarction and Unstable Angina by Demonstration of Circulating Endothelial Cellsvalentina berrocal calderonNo ratings yet
- Varicose Veins: A Clinical Study: Original Research ArticleDocument5 pagesVaricose Veins: A Clinical Study: Original Research ArticleAndhika DNo ratings yet
- Management of Pseudoaneurysms in IV Drug Users: Ori Gi Nal Arti CL eDocument4 pagesManagement of Pseudoaneurysms in IV Drug Users: Ori Gi Nal Arti CL eMayur DadhaniyaNo ratings yet
- Medicine CPC ScriptDocument4 pagesMedicine CPC ScriptMarco Paulo Reyes NaoeNo ratings yet
- PMR and TADocument11 pagesPMR and TAハルァン ファ烏山No ratings yet
- Benign Anorectal Disease: Hemorrhoids, Fissures, and FistulasDocument10 pagesBenign Anorectal Disease: Hemorrhoids, Fissures, and FistulasRilyFannyNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- Blue Toe SyndromeDocument20 pagesBlue Toe SyndromeDaeng MakelloNo ratings yet
- Art15 PDFDocument6 pagesArt15 PDFNatalia TexidorNo ratings yet
- Aortitis, Causas Infrecuentes en Reumatología: Presentación de CasosDocument6 pagesAortitis, Causas Infrecuentes en Reumatología: Presentación de CasosNatalia TexidorNo ratings yet
- Vascular Surgery MCQsDocument4 pagesVascular Surgery MCQsAzkaar100% (2)
- Outcome of Patients Undergoing Amputation For Diabetic Foot UlcerDocument4 pagesOutcome of Patients Undergoing Amputation For Diabetic Foot UlcerrischaNo ratings yet
- Peripheral Artery Disease in Type II Diabetes: Original ArticleDocument4 pagesPeripheral Artery Disease in Type II Diabetes: Original ArticleCristian RajagukgukNo ratings yet
- Eci 12222Document9 pagesEci 12222Andikaputra Brahma WidiantoroNo ratings yet
- Ulceras Vasculares en MiDocument11 pagesUlceras Vasculares en MiKarilNo ratings yet
- Evw Adq ManucciDocument6 pagesEvw Adq Manuccimaria perezNo ratings yet
- A Doppler-Based Evaluation of Peripheral Lower Limb Arterial Insufficiency in Diabetes MellitusDocument4 pagesA Doppler-Based Evaluation of Peripheral Lower Limb Arterial Insufficiency in Diabetes Mellitusresta_pxdNo ratings yet
- Fisiopato IsquemiaDocument12 pagesFisiopato IsquemiaMaría Luisa MantillaNo ratings yet
- Nodules Arising Within Port-Wine Stains: A Clinicopathologic Study of 31 CasesDocument8 pagesNodules Arising Within Port-Wine Stains: A Clinicopathologic Study of 31 CasesMichael Gaona LopezNo ratings yet
- Renal Angiomyolipoma With Renal Vein Invasion: Ase ReportDocument2 pagesRenal Angiomyolipoma With Renal Vein Invasion: Ase Reportdydy_7193No ratings yet
- Hemorrhoidal Laser Procedure - Short - and Long-Term Results From A Prospective StudyDocument5 pagesHemorrhoidal Laser Procedure - Short - and Long-Term Results From A Prospective StudyagusNo ratings yet
- Pancytopenia in Children: Etiological ProfileDocument4 pagesPancytopenia in Children: Etiological ProfileHanshel SatriyaNo ratings yet
- Endovascular Management of Varicose VeinsDocument7 pagesEndovascular Management of Varicose VeinslucyishakNo ratings yet
- Clinical-Pathological Characteristics of Renal Injuries Identify Different Clusters in Patients With Antiphospholipid AntibodiesDocument10 pagesClinical-Pathological Characteristics of Renal Injuries Identify Different Clusters in Patients With Antiphospholipid AntibodiesMayra D' Wonka ToddNo ratings yet
- Intima-Media Thickness of The Common Femoral Artery As A Marker of Leg Ulceration in Sickle Cell Disease PatientsDocument6 pagesIntima-Media Thickness of The Common Femoral Artery As A Marker of Leg Ulceration in Sickle Cell Disease PatientsAnonymous 9QxPDpNo ratings yet
- Letters To The Editor: ReferencesDocument2 pagesLetters To The Editor: ReferencesAji Prasetyo UtomoNo ratings yet
- International Journal of Pharmaceutical Science Invention (IJPSI)Document6 pagesInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNo ratings yet
- Large and Medium Size Vessel and Single Organ VasculitisFrom EverandLarge and Medium Size Vessel and Single Organ VasculitisCarlo SalvaraniNo ratings yet
- Ijhbr January 2018 23-30Document8 pagesIjhbr January 2018 23-30farhanomeNo ratings yet
- Ejbps 11145Document4 pagesEjbps 11145dralourdesreyespediatraNo ratings yet
- Piis107858840500331xDocument8 pagesPiis107858840500331xSahar UntadNo ratings yet
- Evaluation and Management of Hemorrhoids Italian Society of Colorectal SurgeryDocument10 pagesEvaluation and Management of Hemorrhoids Italian Society of Colorectal Surgerynfp.panjaitanNo ratings yet
- KauabajkaDocument7 pagesKauabajkarumasadraunaNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- BUERGER's Inavasc IV Bandung 8 Nov 2013Document37 pagesBUERGER's Inavasc IV Bandung 8 Nov 2013Deviruchi GamingNo ratings yet
- Avm TheraphyDocument11 pagesAvm TheraphynurminsyahNo ratings yet
- 風免journalDocument45 pages風免journalpeipeipoorNo ratings yet
- Abnormal Ankle Brachial Index and The Presence of Significant Coronary Artery DiseaseDocument4 pagesAbnormal Ankle Brachial Index and The Presence of Significant Coronary Artery DiseaseNoviLindriatiNo ratings yet
- 15: Peripheral Vascular Disease: Patient Evaluation The Vascular DiseasesDocument15 pages15: Peripheral Vascular Disease: Patient Evaluation The Vascular DiseasespoddataNo ratings yet
- Superficial Thrombophlebitis Follow-Up Study: Legs: Randomized, ControlledDocument7 pagesSuperficial Thrombophlebitis Follow-Up Study: Legs: Randomized, ControlledFlorin BzoviiNo ratings yet
- Clinical Profile of Systemic Lupus Erythematosus Patients at A Tertiary Care Centre in Western IndiaDocument6 pagesClinical Profile of Systemic Lupus Erythematosus Patients at A Tertiary Care Centre in Western IndiaDivika ShilvanaNo ratings yet
- JurnalDocument8 pagesJurnalSayhrianti SareaNo ratings yet
- Treatment, or Fiction?: Venous Disease: Investigation and FactDocument5 pagesTreatment, or Fiction?: Venous Disease: Investigation and FactJohn CaldasNo ratings yet
- Hotineanu V., Iliadi A.Document4 pagesHotineanu V., Iliadi A.Igor AmbrosNo ratings yet
- The Venous Ulcer Continues ToDocument8 pagesThe Venous Ulcer Continues ToAsmat BurhanNo ratings yet
- Evaluation of Hematological Parameters and Bone Marrow in Indian Patients Suffering From PancytopeniaDocument15 pagesEvaluation of Hematological Parameters and Bone Marrow in Indian Patients Suffering From PancytopeniaJUAN PABLONo ratings yet
- Thromboembolic Complications in Chronic Inflammatory Bowel DiseaseDocument6 pagesThromboembolic Complications in Chronic Inflammatory Bowel DiseaseIJAR JOURNALNo ratings yet
- Gota NEJMDocument11 pagesGota NEJMPerejiloNo ratings yet
- Diffuse Hemangiomatosis of The Spleen - Case ReportDocument4 pagesDiffuse Hemangiomatosis of The Spleen - Case ReportIJAR JOURNALNo ratings yet
- Letter To The Editor: ReferencesDocument1 pageLetter To The Editor: ReferencesKita KuatNo ratings yet
- 22.vascular Pathology 1Document68 pages22.vascular Pathology 1Suhaani JainNo ratings yet
- Penyakit Arteri - VenaDocument44 pagesPenyakit Arteri - VenaAzkiaNo ratings yet
- Endocarditis Caused by Unusual Streptococcus Species (Streptococcus Pluranimalium)Document4 pagesEndocarditis Caused by Unusual Streptococcus Species (Streptococcus Pluranimalium)Soria M JorgeNo ratings yet
- HP113 06 NonvaricealDocument9 pagesHP113 06 NonvaricealEksy AndhikaNo ratings yet
- Treatment of Vascular Malformations of The Mandible: A Description of 12 CasesDocument5 pagesTreatment of Vascular Malformations of The Mandible: A Description of 12 CasesneyhaaNo ratings yet
- Mirizzi Syndrome'Document16 pagesMirizzi Syndrome'Ann Alegre ValenzuelaNo ratings yet
- Characterisation of Hypertrophic Cardiomyopathy by Cardiac Magnetic Resonance ImagingDocument6 pagesCharacterisation of Hypertrophic Cardiomyopathy by Cardiac Magnetic Resonance ImagingIJAR JOURNALNo ratings yet
- 4 - Patophysiology of Cardiovascular Disease PPDocument126 pages4 - Patophysiology of Cardiovascular Disease PPFirdaws FaxirNo ratings yet
- Normal Coronary Artery Dimensions in IndiansDocument6 pagesNormal Coronary Artery Dimensions in IndiansISHAN NIGAMNo ratings yet
- Paper " Part of Human Body and Health Problem HEART DISEASE"Document6 pagesPaper " Part of Human Body and Health Problem HEART DISEASE"ekklesia imbingNo ratings yet
- STROKE and Its TypesDocument28 pagesSTROKE and Its TypesESHA AFZALNo ratings yet
- Mitral Valve Disease: A Comprehensive ReviewDocument8 pagesMitral Valve Disease: A Comprehensive ReviewArthurNo ratings yet
- Pathophysiology and EtiologyDocument2 pagesPathophysiology and EtiologyAgronaSlaughterNo ratings yet
- Arianna Mabunga Bsn-3BDocument7 pagesArianna Mabunga Bsn-3BArianna Jasmine MabungaNo ratings yet
- Abdominal Aortic Aneurysm Case Study: by Lisa ErwertDocument21 pagesAbdominal Aortic Aneurysm Case Study: by Lisa ErwertShashidhar Venkatesh MurthyNo ratings yet
- InaaccDocument2 pagesInaaccDzikrul Haq KarimullahNo ratings yet
- Atherosclerosis IGCSE BiologyDocument24 pagesAtherosclerosis IGCSE BiologyyarinaosuNo ratings yet
- Pi Is 0022347617311927Document1 pagePi Is 0022347617311927Umesh BabuNo ratings yet
- Histologi KardiovaskularDocument32 pagesHistologi KardiovaskularMochammad Fariz AmsalNo ratings yet
- Arteries of AbdomenDocument3 pagesArteries of Abdomenmero1983No ratings yet
- Eclampsia Nursing Care Plan - Altered Tissue PerfusionDocument2 pagesEclampsia Nursing Care Plan - Altered Tissue PerfusionCyrus De Asis84% (32)
- Percutaneous Coronary Interventions For Chronic Total Occlusion 2019Document155 pagesPercutaneous Coronary Interventions For Chronic Total Occlusion 2019mepimplolabotellasNo ratings yet
- Portal Vein - WikipediaDocument23 pagesPortal Vein - WikipediaNaqeeb AhmadNo ratings yet
- Cardiac OutputDocument31 pagesCardiac OutputDylan BhuriNo ratings yet
- Venipuncture Module 1 - Anatomy of The Arm and Vein LocationDocument21 pagesVenipuncture Module 1 - Anatomy of The Arm and Vein LocationAulita AlphonceNo ratings yet
- PCI Vs CABG (Final)Document44 pagesPCI Vs CABG (Final)AnindyaSarkar100% (1)
- Acls Drugs FlashcardsDocument4 pagesAcls Drugs FlashcardsLisaNo ratings yet
- Congenital Heart Diseases (Board Preparation)Document15 pagesCongenital Heart Diseases (Board Preparation)HÉCTOR ULISES AGUILAR ARIASNo ratings yet
- Brochure Awareness of Heart HealthDocument2 pagesBrochure Awareness of Heart HealthCONSTANTINE SAMSONNo ratings yet
- How To Choose Between Rate and Rhythm Control Strategy: Review ArticleDocument9 pagesHow To Choose Between Rate and Rhythm Control Strategy: Review ArticleAngga Aryo LukmantoNo ratings yet
- Atrial Fibrillation: Racheal James Heart Rhythm Specialist Nurse UHWDocument37 pagesAtrial Fibrillation: Racheal James Heart Rhythm Specialist Nurse UHWAman ChaudharyNo ratings yet
- Textbook of Cardiovascular Medicine in Dogs and Cats (VetBooks - Ir)Document1,112 pagesTextbook of Cardiovascular Medicine in Dogs and Cats (VetBooks - Ir)Jonathan Mann100% (1)
- Original Article Knowledge of Coronary Artery Disease (CAD) Risk Factors and Coronary Intervention Among University StudentsDocument5 pagesOriginal Article Knowledge of Coronary Artery Disease (CAD) Risk Factors and Coronary Intervention Among University StudentsNise Mon KuriakoseNo ratings yet
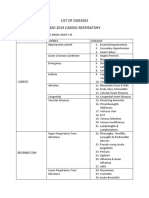
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemDawnmurph Dharlene Wag-eNo ratings yet
- Biology Grade 9 - Lesson NoteDocument9 pagesBiology Grade 9 - Lesson NotemicahxNo ratings yet