You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- GBS Source 1Document4 pagesGBS Source 1PJHG50% (2)
- Acute Inflammatory Demyelinating PolyneuropathyDocument55 pagesAcute Inflammatory Demyelinating PolyneuropathyImmanuel100% (1)
- Acquired NeuropathiesDocument106 pagesAcquired NeuropathiesDanny J. BrouillardNo ratings yet
- PTSD EssayDocument2 pagesPTSD Essayapi-338213804No ratings yet
- GuillainDocument2 pagesGuillainAlly JuanezaNo ratings yet
- Guillan Barre Syndrome FinalDocument16 pagesGuillan Barre Syndrome FinalAswathy RCNo ratings yet
- Gullain Barré Syndrome: Prabhjot Kaur Msc. (N) Final YearDocument13 pagesGullain Barré Syndrome: Prabhjot Kaur Msc. (N) Final YearKataria DavinNo ratings yet
- GB Syndrome..Document13 pagesGB Syndrome..Shitaljit Irom100% (1)
- Guillain-Barré Syndrome: Dr. Angelo Smith M.D WHPLDocument30 pagesGuillain-Barré Syndrome: Dr. Angelo Smith M.D WHPLLeshery SemiraNo ratings yet
- Guillain Barre SyndromeDocument38 pagesGuillain Barre SyndromePeterson Wachira HscNo ratings yet
- Pneumoniae), Vaccines (E.g., Rabies, Tetanus, and Influenza), Lymphoma, Surgery, and TraumaDocument7 pagesPneumoniae), Vaccines (E.g., Rabies, Tetanus, and Influenza), Lymphoma, Surgery, and TraumaKenn yahweexNo ratings yet
- Assistant Prof - Dr.Imtiaz Ahmad. FCPS (Medicine)Document27 pagesAssistant Prof - Dr.Imtiaz Ahmad. FCPS (Medicine)EssaAyazNo ratings yet
- Guillain-Barré Syndrome (GBS) : Prepared by Dr. Madiha Anees PT Asst. Prof/VP RCRS MS-PT, BS-PTDocument26 pagesGuillain-Barré Syndrome (GBS) : Prepared by Dr. Madiha Anees PT Asst. Prof/VP RCRS MS-PT, BS-PTaneelala kanwal kanwalNo ratings yet
- Grp3 Trans - Neurological Disturbances Degenerative 1Document12 pagesGrp3 Trans - Neurological Disturbances Degenerative 1Rachelle DelantarNo ratings yet
- Guillain-Barre Syndrome: InfectionsDocument13 pagesGuillain-Barre Syndrome: InfectionsUzra ShujaatNo ratings yet
- Guillain-Barré Syndrome, Myasthenia Gravis,: Dr. Nermine ElcokanyDocument31 pagesGuillain-Barré Syndrome, Myasthenia Gravis,: Dr. Nermine ElcokanyTheresia Avila KurniaNo ratings yet
- Guillain Barre Syndrome: Molebatsi TheletsaneDocument16 pagesGuillain Barre Syndrome: Molebatsi TheletsaneSri KombongNo ratings yet
- Guillain Barre SyndromeDocument20 pagesGuillain Barre SyndromeRamalakshmi LakshmiNo ratings yet
- Guillain BarréDocument4 pagesGuillain BarréAlondra CastilloNo ratings yet
- Merci PDFDocument33 pagesMerci PDFhuda dotNo ratings yet
- Gulian Barre SyndromeDocument12 pagesGulian Barre SyndromeShauki AliNo ratings yet
- Guillain Barre SyndromeDocument16 pagesGuillain Barre SyndromeNeha Rathore100% (1)
- Presentation Guillian Barre SyndromeDocument12 pagesPresentation Guillian Barre SyndromeKristian Karl Bautista Kiw-isNo ratings yet
- Script For PresentDocument3 pagesScript For PresentTanya HoNo ratings yet
- Ann MS Id 000849Document8 pagesAnn MS Id 000849azucenadeoNo ratings yet
- Guillian Baare Syndrome: Mr. Jeo Thomas 1 M.SC Nursing SconDocument38 pagesGuillian Baare Syndrome: Mr. Jeo Thomas 1 M.SC Nursing SconJeo Thomas100% (1)
- 4 - Gullian Barr SyndromeDocument12 pages4 - Gullian Barr SyndromeHADI BADWANNo ratings yet
- GB SyndromeDocument17 pagesGB Syndromehajra StudentNo ratings yet
- Referat GBSDocument12 pagesReferat GBSSoraya Dwi KhairunnisaNo ratings yet
- Overview of Guillain-Barré Syndrome: I. Literature ReviewDocument10 pagesOverview of Guillain-Barré Syndrome: I. Literature ReviewS Dian RNo ratings yet
- Acute Flaccid ParalysisDocument19 pagesAcute Flaccid Paralysisapi-3815243100% (1)
- Guillain Barré SyndromeDocument20 pagesGuillain Barré Syndromelourdes kusumadiNo ratings yet
- Guillain-Barré Syndrome Med Student PresentationDocument16 pagesGuillain-Barré Syndrome Med Student PresentationRon ShenkarNo ratings yet
- Acute Sensory-Motor Axonal Neuropathy in A 57-Year-Old Male Presenting With Paresthesia and Distal Muscle WeaknessDocument3 pagesAcute Sensory-Motor Axonal Neuropathy in A 57-Year-Old Male Presenting With Paresthesia and Distal Muscle WeaknessSophia PapathanasiouNo ratings yet
- Gullain-Barre SyndromeDocument7 pagesGullain-Barre Syndromejanellekate1224No ratings yet
- Guillain Barre SyndromeDocument13 pagesGuillain Barre SyndromeAdreiTheTripleANo ratings yet
- Gullain Barre SyndromeDocument33 pagesGullain Barre SyndromeNor Ubudiah SetiNo ratings yet
- Guillain-Barré Syndrome: Andrie Gunawan, MDDocument17 pagesGuillain-Barré Syndrome: Andrie Gunawan, MDAgung TpNo ratings yet
- 2021 - Neuromuscular Disorders in The Intensive Care UnitDocument21 pages2021 - Neuromuscular Disorders in The Intensive Care UnitOlga Manco GuzmánNo ratings yet
- A Case of Guillain-Barre Syndrome in A Primary Care Setting: Sherly Sebastian, DNP, RN, NP-CDocument6 pagesA Case of Guillain-Barre Syndrome in A Primary Care Setting: Sherly Sebastian, DNP, RN, NP-CdewiprahazNo ratings yet
- Differentiatingfamilial Neuropathiesfrom Guillain-Barre SyndromeDocument22 pagesDifferentiatingfamilial Neuropathiesfrom Guillain-Barre SyndromeKartika IwangNo ratings yet
- 5 Malado Guillain Barre SyndromeDocument7 pages5 Malado Guillain Barre SyndromeAllan CastroNo ratings yet
- Jurnal GBSDocument26 pagesJurnal GBSfajar sugandaNo ratings yet
- GuillainDocument4 pagesGuillainanime listNo ratings yet
- Guillain Barre SyndromeDocument19 pagesGuillain Barre SyndromeLovely CervantesNo ratings yet
- Chapter 607 - Guillain-Barré Syndrome: Clinical ManifestationsDocument3 pagesChapter 607 - Guillain-Barré Syndrome: Clinical ManifestationsclaudiaNo ratings yet
- Guillain Barre Syndrome A ReviewDocument7 pagesGuillain Barre Syndrome A ReviewEditor IJTSRDNo ratings yet
- Guillain-Barre Syndrome: Practice EssentialsDocument18 pagesGuillain-Barre Syndrome: Practice EssentialsAna-Maria DuMiNo ratings yet
- Pa Tho Physiology of Guillain Barre SyndromeDocument4 pagesPa Tho Physiology of Guillain Barre Syndromenaman24No ratings yet
- Guillain-Barré Syndrome Pediatrico 2018Document4 pagesGuillain-Barré Syndrome Pediatrico 2018Mariam Plata100% (1)
- 2 - Debilidad AgudaDocument15 pages2 - Debilidad AgudaMarian ZeaNo ratings yet
- Guillain Barre SyndromeDocument18 pagesGuillain Barre SyndromeTimothy Dycalle ManosNo ratings yet
- Guillain Barre Syndrome (GBS) ImanDocument26 pagesGuillain Barre Syndrome (GBS) ImanTowardsLight100% (5)
- Peripheral NeuropathyDocument49 pagesPeripheral NeuropathyArvindhanNo ratings yet
- Diseases of Peripheral NervesDocument46 pagesDiseases of Peripheral NervesAkaNo ratings yet
- Guillain Barre SyndromeDocument32 pagesGuillain Barre SyndromeDada MundaNo ratings yet
- Altered Mental Status in "Guillain-Barre Syndrome" - A Noteworthy Clinical Clue. Eoin MulroyDocument19 pagesAltered Mental Status in "Guillain-Barre Syndrome" - A Noteworthy Clinical Clue. Eoin MulroyJeffery TaylorNo ratings yet
- Chapter 23 Acquired Neuropathies PDFDocument106 pagesChapter 23 Acquired Neuropathies PDFzloncar3No ratings yet
- Japanese Encephalitis Note 30-Dec-2019 2-40-55 PMDocument4 pagesJapanese Encephalitis Note 30-Dec-2019 2-40-55 PMvenkannaNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Ischemic StrokeDocument7 pagesIschemic StrokeAlly Juaneza100% (1)
- Huntington DiseaseDocument2 pagesHuntington DiseaseAlly JuanezaNo ratings yet
- StaffingDocument3 pagesStaffingAlly JuanezaNo ratings yet
- Republic Act NoDocument7 pagesRepublic Act NoAlly JuanezaNo ratings yet
- Professional Adjustment in NursingDocument6 pagesProfessional Adjustment in NursingAlly JuanezaNo ratings yet
- Regular AppointmentDocument1 pageRegular AppointmentAlly JuanezaNo ratings yet
- Huntington DiseaseDocument2 pagesHuntington DiseaseAlly JuanezaNo ratings yet
- PLANNINGDocument3 pagesPLANNINGAlly JuanezaNo ratings yet
- Myasthenia GravisDocument2 pagesMyasthenia GravisAlly JuanezaNo ratings yet
- Ischemic StrokeDocument7 pagesIschemic StrokeAlly JuanezaNo ratings yet
- Meningitis QuestionsDocument2 pagesMeningitis QuestionsAlly JuanezaNo ratings yet
- The Third International Consensus Definition For Sepsis and Septic ShockDocument13 pagesThe Third International Consensus Definition For Sepsis and Septic ShockdrhendyjuniorNo ratings yet
- A Review of Literature of Anxiety Amongst AdolescenceDocument3 pagesA Review of Literature of Anxiety Amongst AdolescenceViveca Isabelle NamiaNo ratings yet
- Epilepsy IN Children: Presented by DR - Meera Pramil Department of KaumarabhrityaDocument60 pagesEpilepsy IN Children: Presented by DR - Meera Pramil Department of KaumarabhrityaAnil DasNo ratings yet
- Subarachnoid HemorrhageDocument3 pagesSubarachnoid Hemorrhagetenaj_purpleNo ratings yet
- Febrile Seizure: Presented by Raksha DhakalDocument22 pagesFebrile Seizure: Presented by Raksha Dhakalsagar poudelNo ratings yet
- Nursing Care Plan: Assessment Explanation of The Problem Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Explanation of The Problem Objectives Interventions Rationale EvaluationNelly CruzNo ratings yet
- 1-2022 Gastric CancerDocument95 pages1-2022 Gastric CancerAli Murtaza AbbasNo ratings yet
- Organic Brain DisorderDocument69 pagesOrganic Brain DisorderHowell Mathew100% (1)
- Scared ParentDocument2 pagesScared ParentADHDESCESTNo ratings yet
- Retinopathy of PrematurityDocument3 pagesRetinopathy of PrematurityluckydrewNo ratings yet
- Method Matters: Understanding Diagnostic Reliability In: DSM-IV and DSM-5Document6 pagesMethod Matters: Understanding Diagnostic Reliability In: DSM-IV and DSM-5hadassaNo ratings yet
- Exam Questions 4 CourseDocument4 pagesExam Questions 4 CourseVishva Lalitbhai HirparaNo ratings yet
- Pru Life Uk Proposal For Shinsha Camille Pangilinan v2Document3 pagesPru Life Uk Proposal For Shinsha Camille Pangilinan v2AntonNo ratings yet
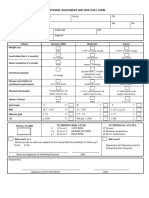
- 4 - Nutritional Assessment and Risk LevelDocument1 page4 - Nutritional Assessment and Risk LevelBok MatthewNo ratings yet
- Kidney Treatment Guidelines For HyponatremiaDocument7 pagesKidney Treatment Guidelines For HyponatremialguerreroNo ratings yet
- Project 1 Final DraftDocument8 pagesProject 1 Final Draftapi-741172597No ratings yet
- Acute Kidney Injury Case Study FinalDocument46 pagesAcute Kidney Injury Case Study FinalSalwa KaramanNo ratings yet
- TataDocument2 pagesTatavamsi NathNo ratings yet
- The New Definition and Classification of Seizures and EpilepsyDocument16 pagesThe New Definition and Classification of Seizures and EpilepsynadiafyNo ratings yet
- Assessment of Yellow FlagsDocument2 pagesAssessment of Yellow FlagsPhil FaitNo ratings yet
- Introduction of The ResearchDocument3 pagesIntroduction of The Researchcristine baldazoNo ratings yet
- Gender Dysphoria and Autism Spectrum Disorder A Narrative ReviewDocument12 pagesGender Dysphoria and Autism Spectrum Disorder A Narrative ReviewLourdes GoicoecheaNo ratings yet
- Major and Minor TranquilizerDocument6 pagesMajor and Minor TranquilizerAli IjazNo ratings yet
- 1000 Plus Psychiatry MCQ Book DranilkakunjeDocument141 pages1000 Plus Psychiatry MCQ Book Dranilkakunjethelegend 20220% (1)
- Aspects Cliniques Et Evolutifs Du Choc Septique en Reanimation Du Chu AndohatapenakaDocument8 pagesAspects Cliniques Et Evolutifs Du Choc Septique en Reanimation Du Chu AndohatapenakaIJAR JOURNALNo ratings yet
- Asian Journal of Psychiatry: Letter To The EditorDocument2 pagesAsian Journal of Psychiatry: Letter To The Editornofirly hamliNo ratings yet
- PTC Slides 2016Document290 pagesPTC Slides 2016graceduma100% (1)
- Soal Ujian EBM PraktekDocument6 pagesSoal Ujian EBM Praktekbobbyrianto2210No ratings yet
- Autism: DefinitionDocument6 pagesAutism: DefinitionBallave SudiptaNo ratings yet