You might also like
- ABMLI Sample Questions 000Document7 pagesABMLI Sample Questions 000samy100% (1)
- Gustav Vasa BIBLE, 1541.Document93 pagesGustav Vasa BIBLE, 1541.Molitvena zajednica sv. Mihaela arhanđela100% (3)
- Nycocard Reader PrincipleDocument6 pagesNycocard Reader Principlemrhrtn88No ratings yet
- Paraproteins Are A Common Cause of Interferences With Automated Chemistry MethodsDocument7 pagesParaproteins Are A Common Cause of Interferences With Automated Chemistry MethodsramazankocabasNo ratings yet
- Paraprotein Interference On A Direct Bilirubin AssayDocument8 pagesParaprotein Interference On A Direct Bilirubin AssayramazankocabasNo ratings yet
- Protein Precipitation As A Possible Important Pitfall in The Clinical Chemistry Analysis of Blood Samples Containing Monoclonal ImmunoglobulinsDocument11 pagesProtein Precipitation As A Possible Important Pitfall in The Clinical Chemistry Analysis of Blood Samples Containing Monoclonal ImmunoglobulinsramazankocabasNo ratings yet
- Thrombocytopathia and Light-Chain Proteinuria in A Dog Naturally Infected WithDocument3 pagesThrombocytopathia and Light-Chain Proteinuria in A Dog Naturally Infected WithDiana GranadaNo ratings yet
- Secondary Hemophagocytic Lymphohistiocytosis: A Rare Case ReportDocument5 pagesSecondary Hemophagocytic Lymphohistiocytosis: A Rare Case ReportivanNo ratings yet
- Icteric Index and Its SignificanceDocument3 pagesIcteric Index and Its SignificanceJulius FrondaNo ratings yet
- 5.J Clin Pathol 2012 Salinas 928 33Document7 pages5.J Clin Pathol 2012 Salinas 928 33Nofiyanty NicolasNo ratings yet
- AACE Clinical Case ReportsDocument3 pagesAACE Clinical Case ReportsSameerNo ratings yet
- Cholestatic Hepatitis CaseDocument3 pagesCholestatic Hepatitis CaseIndra YaniNo ratings yet
- How Do Light and Temperature Affect Laboratory Investigations On Serum Bilirubin?Document10 pagesHow Do Light and Temperature Affect Laboratory Investigations On Serum Bilirubin?Cha RichardNo ratings yet
- Low Serum Bicarbonate in A Patient With Diabetes&#Document3 pagesLow Serum Bicarbonate in A Patient With Diabetes&#ayaz ahmadNo ratings yet
- 1084.fullDocument5 pages1084.fullskyesharray16No ratings yet
- Biochem2 Practical1Document5 pagesBiochem2 Practical1puhranee nathanNo ratings yet
- Com Per 2005Document7 pagesCom Per 2005Rina ErlinaNo ratings yet
- Hematological and Metabolical Aspects From Laboratory MediDocument109 pagesHematological and Metabolical Aspects From Laboratory MediNadirNo ratings yet
- Rounds: Case Study and Review of Autoimmune HepatitisDocument7 pagesRounds: Case Study and Review of Autoimmune HepatitisClaudia Naomi Ventura OrtizNo ratings yet
- Mass Spectrometry of Nucleic AcidsDocument2 pagesMass Spectrometry of Nucleic AcidsnbkondaNo ratings yet
- Hemolytic Anemia, SuicideDocument5 pagesHemolytic Anemia, SuicideturkiNo ratings yet
- Diabetic Post Mortem PDFDocument7 pagesDiabetic Post Mortem PDFPrakarsa Adi Daya NusantaraNo ratings yet
- 10 1097MD 0000000000000587Document3 pages10 1097MD 0000000000000587abbasamiri135103No ratings yet
- A Case of Severe Hypertriglyceridaemia and HypercholesterolaemiaDocument1 pageA Case of Severe Hypertriglyceridaemia and Hypercholesterolaemiathys2000No ratings yet
- KFD Case ReportDocument7 pagesKFD Case ReportDr AzharNo ratings yet
- A Review of Electrophoretic Patterns From A Tertiary Care Nephrourology Referral CentreDocument5 pagesA Review of Electrophoretic Patterns From A Tertiary Care Nephrourology Referral CentreTrương Ngọc HàNo ratings yet
- Comparison of Visual vs. Automated Detection of Lipemic, Icteric and Hemolyzed Specimens Can We Rely On A Human EyeDocument5 pagesComparison of Visual vs. Automated Detection of Lipemic, Icteric and Hemolyzed Specimens Can We Rely On A Human EyeDaniel Huachani CoripunaNo ratings yet
- Case Report: Severe Hyperbilirubinemia: A Rare Complication of Lyme DiseaseDocument4 pagesCase Report: Severe Hyperbilirubinemia: A Rare Complication of Lyme DiseaseDhruva PatelNo ratings yet
- Laboratory Test of Immune SystemDocument30 pagesLaboratory Test of Immune SystemYosi W KusumaNo ratings yet
- Microprotein: (Pyrogallol Red Method)Document2 pagesMicroprotein: (Pyrogallol Red Method)InaGargNo ratings yet
- Neonatal Anemia: Revisiting The Enigmatic PyknocyteDocument5 pagesNeonatal Anemia: Revisiting The Enigmatic PyknocyteDavid MerchánNo ratings yet
- 10.1515 - Almed 2021 0087Document6 pages10.1515 - Almed 2021 0087Miguel Ángel Martínez MartínNo ratings yet
- Amoxicillin and Ceftriaxone As Treatment Alternatives To Penicillin For Maternal Syphilis 2017Document3 pagesAmoxicillin and Ceftriaxone As Treatment Alternatives To Penicillin For Maternal Syphilis 2017Jose Luis Morales BautistaNo ratings yet
- Identification and Molecular Analysis of 17 Novel Variants of HMBSDocument14 pagesIdentification and Molecular Analysis of 17 Novel Variants of HMBSdivillamarinNo ratings yet
- Ferritin - SOPDocument6 pagesFerritin - SOPNoor AshrafNo ratings yet
- International Journal of Infectious Diseases: Jian-Wu Yu, Li-Jie Sun, Yong-Hua Zhao, Peng Kang, Bing-Zhu YanDocument6 pagesInternational Journal of Infectious Diseases: Jian-Wu Yu, Li-Jie Sun, Yong-Hua Zhao, Peng Kang, Bing-Zhu YanDendy TriatmajaNo ratings yet
- Haemoglobin Electrophoresis in Diagnosing A Case oDocument3 pagesHaemoglobin Electrophoresis in Diagnosing A Case oYunonNo ratings yet
- Alkalosis RespiratoryDocument9 pagesAlkalosis RespiratoryJack Eugene LiowNo ratings yet
- CC Completion Exam Cycle 21Document6 pagesCC Completion Exam Cycle 21Marie LlanesNo ratings yet
- Hypercalcemia, Acute Kidney Injury, and Esophageal LymphadenopathyDocument3 pagesHypercalcemia, Acute Kidney Injury, and Esophageal Lymphadenopathysar9203No ratings yet
- HLA-DQ2 patients with active CD have circulating tTG-specific T cell clonesDocument1 pageHLA-DQ2 patients with active CD have circulating tTG-specific T cell clonesCatalina Mariana MargarintNo ratings yet
- Lombriz PCRDocument3 pagesLombriz PCRNorma TamezNo ratings yet
- Erythema Nodosum Associated With Terbinafine Therapy A Case ReportDocument5 pagesErythema Nodosum Associated With Terbinafine Therapy A Case ReportAthenaeum Scientific PublishersNo ratings yet
- AbChek Dengue Combo Rapid TestDocument1 pageAbChek Dengue Combo Rapid TestNulifeNo ratings yet
- Acute Naphthalene Poisoning Following The Non-Accidental Ingestion of MothballsDocument4 pagesAcute Naphthalene Poisoning Following The Non-Accidental Ingestion of MothballsnaveenNo ratings yet
- An Unique Encounter With ParaprotenemiaDocument3 pagesAn Unique Encounter With ParaprotenemiaramazankocabasNo ratings yet
- Hemoglobin PDFDocument6 pagesHemoglobin PDFMega Devega ArvianyNo ratings yet
- Hb electrophoresis diagnoses sickle cell anemia with β-thalassemiaDocument3 pagesHb electrophoresis diagnoses sickle cell anemia with β-thalassemiaTawsif MusharofNo ratings yet
- Karen Smith Duty Biochemist ScenariosDocument43 pagesKaren Smith Duty Biochemist Scenariosmonday125100% (2)
- Aspergillus PCRtesting: results from a prospective PCR study within the AmBiLoadtrialDocument6 pagesAspergillus PCRtesting: results from a prospective PCR study within the AmBiLoadtriallaura.caicedoNo ratings yet
- Https Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId Cr145Zu6uIdSIdOmfwSmnADocument3 pagesHttps Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId Cr145Zu6uIdSIdOmfwSmnAsudanmadhu092No ratings yet
- Assessment of α1antitrypsin and α2macroglobulin levels in obese patientsDocument5 pagesAssessment of α1antitrypsin and α2macroglobulin levels in obese patientsAnnisa SufiNo ratings yet
- Labmed34 0354Document4 pagesLabmed34 0354zeeshanNo ratings yet
- AbChek Dengue ns1 Ag Rapid TestDocument1 pageAbChek Dengue ns1 Ag Rapid TestNulifeNo ratings yet
- Total Bilirubin L3K Assay: Genzyme Diagnostics P.E.I. IncDocument3 pagesTotal Bilirubin L3K Assay: Genzyme Diagnostics P.E.I. IncPikiy PutriNo ratings yet
- 2015 Article 32Document5 pages2015 Article 32yantuNo ratings yet
- BID2Document2 pagesBID2Inversiones Llanolab, c.a. LlanolabNo ratings yet
- Guillain Barr Syndrome Occurring Synchronously With Systemic Lupus Erythematosus As Initial Manifestation Treated Successfully With Low DoseDocument5 pagesGuillain Barr Syndrome Occurring Synchronously With Systemic Lupus Erythematosus As Initial Manifestation Treated Successfully With Low DoseTessa CruzNo ratings yet
- Course Case Studies - Viral HepatitisDocument5 pagesCourse Case Studies - Viral HepatitiswqmxmNo ratings yet
- Lipid MediatorsFrom EverandLipid MediatorsFiona M. CunninghamNo ratings yet
- High-Resolution Electrophoresis and Immunofixation: Techniques and InterpretationFrom EverandHigh-Resolution Electrophoresis and Immunofixation: Techniques and InterpretationRating: 5 out of 5 stars5/5 (1)
- Utility of Icteric Index in Clinical Laboratories - More Than A Preanalytical IndicatorDocument9 pagesUtility of Icteric Index in Clinical Laboratories - More Than A Preanalytical IndicatorramazankocabasNo ratings yet
- Measuring Serum Bilirubin with the Icterus IndexDocument6 pagesMeasuring Serum Bilirubin with the Icterus IndexramazankocabasNo ratings yet
- An Unique Encounter With ParaprotenemiaDocument3 pagesAn Unique Encounter With ParaprotenemiaramazankocabasNo ratings yet
- Serum markers reveal role of oxidative stress and collagen degradation in canine osteoarthritis modelDocument4 pagesSerum markers reveal role of oxidative stress and collagen degradation in canine osteoarthritis modelramazankocabasNo ratings yet
- McCluskey-2007-Does The Addition of HyaluronanDocument2 pagesMcCluskey-2007-Does The Addition of HyaluronanramazankocabasNo ratings yet
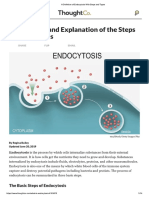
- A Definition of Endocytosis With Steps and TypesDocument14 pagesA Definition of Endocytosis With Steps and TypesramazankocabasNo ratings yet
- Imeko WC 2012 TC21 O10Document5 pagesImeko WC 2012 TC21 O10mcastillogzNo ratings yet
- The Next Questions Will Depend On Your Answer(s) in Question Number 4: 6. The Next Questions Will Depend On Your Answer(s) in Question Number 4: 6Document1 pageThe Next Questions Will Depend On Your Answer(s) in Question Number 4: 6. The Next Questions Will Depend On Your Answer(s) in Question Number 4: 6cgranzore8833% (3)
- GCMS-QP2010 User'sGuide (Ver2.5) PDFDocument402 pagesGCMS-QP2010 User'sGuide (Ver2.5) PDFnguyenvietanhbtNo ratings yet
- Quotation SS20230308 100KVAR APFC PANEL VIDHYA WIRESDocument4 pagesQuotation SS20230308 100KVAR APFC PANEL VIDHYA WIRESsunil halvadiyaNo ratings yet
- International Standard Iso/Iec Software Cycle Processes: Standards SectionDocument16 pagesInternational Standard Iso/Iec Software Cycle Processes: Standards SectionDavid SalgadoNo ratings yet
- Vedic Healing Through Gems4Document3 pagesVedic Healing Through Gems4gesNo ratings yet
- Form 4 Biology Chapter OverviewDocument21 pagesForm 4 Biology Chapter OverviewKar KuanNo ratings yet
- تركيب وتشغيل وحدات تكييف الهواءDocument49 pagesتركيب وتشغيل وحدات تكييف الهواءOmar NabilNo ratings yet
- Enquiries: 1. Enquiry From A Retailer To A Foreign ManufacturerDocument7 pagesEnquiries: 1. Enquiry From A Retailer To A Foreign ManufacturerNhi Hoàng Lê NguyễnNo ratings yet
- S1.8 Template of REAL Table For Power and Supporting CompetenciesDocument3 pagesS1.8 Template of REAL Table For Power and Supporting CompetenciesJamir SalongaNo ratings yet
- G25M R TransmissionDocument29 pagesG25M R TransmissionMaksym VovkNo ratings yet
- The Bourne Identity ReviewDocument3 pagesThe Bourne Identity ReviewBoldizsár Zeyk AnnaNo ratings yet
- The Black Emperor's Grand Grimoire - by Frank GenghisDocument144 pagesThe Black Emperor's Grand Grimoire - by Frank GenghisFrank Genghis0% (2)
- Learn From Customers to Improve Products and ServicesDocument8 pagesLearn From Customers to Improve Products and ServicesQuan Hoang AnhNo ratings yet
- Lean Healthy Raw Food Winter RecipesDocument60 pagesLean Healthy Raw Food Winter RecipesKaio Sol100% (6)
- Lect 1 Transforming EER Diagrams Into Relations (Part III)Document13 pagesLect 1 Transforming EER Diagrams Into Relations (Part III)KIM OFFNo ratings yet
- Las 4.4 - Hope 4 - Mountaineering (Hiking, Trekking, Camping, Orienteering)Document5 pagesLas 4.4 - Hope 4 - Mountaineering (Hiking, Trekking, Camping, Orienteering)Maricel EsperatNo ratings yet
- DOE V Rhodes College Ammended Motion For TRODocument19 pagesDOE V Rhodes College Ammended Motion For TROSouwesterdocs100% (1)
- Mapeh-7pe Q2 Summative-TestDocument2 pagesMapeh-7pe Q2 Summative-TestVhannie AcquiatanNo ratings yet
- Cell Structure & FunctionDocument38 pagesCell Structure & Functiongundogan21100% (1)
- Dual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band ScramblingDocument16 pagesDual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band Scramblingraja rishyantNo ratings yet
- Problem29 40Document1 pageProblem29 40IENCSNo ratings yet
- MS6711 Data Mining Homework 1: 1.1 Implement K-Means Manually (8 PTS)Document6 pagesMS6711 Data Mining Homework 1: 1.1 Implement K-Means Manually (8 PTS)Yihan WangNo ratings yet
- PreceptronDocument17 pagesPreceptroneng_kmmNo ratings yet
- RIZAL: INSPIRATION FOR A NEW GENERATIONDocument11 pagesRIZAL: INSPIRATION FOR A NEW GENERATIONErica B. DaclanNo ratings yet
- Careers at FEWA-DubaiDocument8 pagesCareers at FEWA-DubaiJnanamNo ratings yet
- Review Relative Clauses, Articles, and ConditionalsDocument10 pagesReview Relative Clauses, Articles, and ConditionalsNgoc AnhNo ratings yet
- Timbering Week 5Document22 pagesTimbering Week 5FikaduKitessa0% (1)
- m5 Mage The AscensionDocument20 pagesm5 Mage The AscensionQuentin Agnes0% (1)