You might also like
- FSED 16F Detention and Correctional Occupancy Checklist Rev01Document6 pagesFSED 16F Detention and Correctional Occupancy Checklist Rev01Talaingod FirestationNo ratings yet
- Department of The Interior and Local Government Bureau of Fire ProtectionDocument6 pagesDepartment of The Interior and Local Government Bureau of Fire ProtectionRyan SunNo ratings yet
- Inspection Order Checklist - Fire CodeDocument6 pagesInspection Order Checklist - Fire CodeMichael QuidorNo ratings yet
- Department of The Interior and Local Government Bureau of Fire ProtectionDocument5 pagesDepartment of The Interior and Local Government Bureau of Fire ProtectionBoy ClementeNo ratings yet
- FSED 18F Business Occupancy Checklist Rev01Document5 pagesFSED 18F Business Occupancy Checklist Rev01tzxipenNo ratings yet
- Residential Occupancy ChecklistDocument5 pagesResidential Occupancy ChecklistRozel Laigo ReyesNo ratings yet
- Mercantile Occupancy ChecklistDocument5 pagesMercantile Occupancy ChecklistRozel Laigo ReyesNo ratings yet
- Mercantile Occupancy ChecklistDocument5 pagesMercantile Occupancy ChecklistRozel Laigo ReyesNo ratings yet
- Industrial Occupancy ChecklistDocument5 pagesIndustrial Occupancy ChecklistRozel Laigo ReyesNo ratings yet
- Business Occupancy ChecklistDocument5 pagesBusiness Occupancy ChecklistRozel Laigo ReyesNo ratings yet
- Business Occupancy ChecklistDocument5 pagesBusiness Occupancy ChecklistRozel Laigo ReyesNo ratings yet
- 14 Miscellaneous Occupancy ChecklistDocument4 pages14 Miscellaneous Occupancy ChecklistSylvester Lastrella YecyecNo ratings yet
- FSED 61F Fire Safety Inspection Checklist Rev.00 1Document11 pagesFSED 61F Fire Safety Inspection Checklist Rev.00 1Bfp Caraga SisonfstnNo ratings yet
- FSED 61F Fire Safety Inspection Checklist Rev.00 New 1Document12 pagesFSED 61F Fire Safety Inspection Checklist Rev.00 New 1BurgosFirestation100% (1)
- FSED 61F Fire Safety Inspection Checklist Rev.00Document10 pagesFSED 61F Fire Safety Inspection Checklist Rev.00Talaingod Firestation100% (1)
- Department of The Interior and Local Government Bureau of Fire ProtectionDocument3 pagesDepartment of The Interior and Local Government Bureau of Fire ProtectionreferizaruthjoyNo ratings yet
- FSED 61F Fire Safety Inspection Checklist Rev.00 1Document11 pagesFSED 61F Fire Safety Inspection Checklist Rev.00 1Paula Marie AgripaNo ratings yet
- FSED 24F Fire Safety Inspection Checklist Small General Business Establishment Rev.02Document2 pagesFSED 24F Fire Safety Inspection Checklist Small General Business Establishment Rev.02Calabanga Fire StationNo ratings yet
- FSMR FormatDocument7 pagesFSMR Formatian007papagNo ratings yet
- 27o Open Hole Grating PermitDocument1 page27o Open Hole Grating Permitmalik jahanNo ratings yet
- FSED 24F Fire Safety Inspection Checklist Small General Business Establishment Rev.02Document2 pagesFSED 24F Fire Safety Inspection Checklist Small General Business Establishment Rev.02april oyardoNo ratings yet
- Northwest Shoals Hot Work Permit1Document1 pageNorthwest Shoals Hot Work Permit1api-402808072No ratings yet
- Checklist For Single and Two Family DwellingsDocument2 pagesChecklist For Single and Two Family DwellingsBurgosFirestationNo ratings yet
- 22 FSED 023 Checklist Theater Occupancy Rev01 070519Document5 pages22 FSED 023 Checklist Theater Occupancy Rev01 070519Trash 2No ratings yet
- Safety Audit Form FormetDocument5 pagesSafety Audit Form FormetRichard BaileyNo ratings yet
- Workplace Security Checklistx4Document3 pagesWorkplace Security Checklistx4Jennifer SheltonNo ratings yet
- 27o Open Hole Grating PermitDocument1 page27o Open Hole Grating PermitMohammed MinhajNo ratings yet
- FSED 26F Gasoline Service Station Checklist Rev01Document3 pagesFSED 26F Gasoline Service Station Checklist Rev01Bfp Rvii SanMiguel FirestationNo ratings yet
- FM - Ik - Odr - Mep-006-03 Sound SystemDocument1 pageFM - Ik - Odr - Mep-006-03 Sound Systemagun gunawanNo ratings yet
- IAQ Building & Demographics ChecklistDocument9 pagesIAQ Building & Demographics ChecklistdineshNo ratings yet
- Working at Height Permit R1Document1 pageWorking at Height Permit R1tamuthuNo ratings yet
- Pre Incident PlanDocument7 pagesPre Incident PlanKelvinDavisNo ratings yet
- Small General Business Occupancy Checklist MFD 2022 Anonas Diagnostic ClinicDocument4 pagesSmall General Business Occupancy Checklist MFD 2022 Anonas Diagnostic ClinicTeresita AlcaideNo ratings yet
- Security Survey CHK ListDocument15 pagesSecurity Survey CHK ListKazi Mazzad Ahmed Titas100% (2)
- Application Form For Safety Measures - Buildings-1Document2 pagesApplication Form For Safety Measures - Buildings-1Ch Ahmed MahmoodNo ratings yet
- Workplace Security ChecklistDocument3 pagesWorkplace Security ChecklistAnonymous 6pn00AfL0% (1)
- Room Data Sheet Pour La MRiDocument2 pagesRoom Data Sheet Pour La MRiCarole CaronNo ratings yet
- FSED 26F Gasoline Service Station Checklist Rev01Document3 pagesFSED 26F Gasoline Service Station Checklist Rev01tzxipenNo ratings yet
- FRM-9114-0201 Safe Work PermitDocument5 pagesFRM-9114-0201 Safe Work PermitNat OffeiNo ratings yet
- 5 6307674058502701168 PDFDocument2 pages5 6307674058502701168 PDFReda MashalNo ratings yet
- General Work Permit R1Document1 pageGeneral Work Permit R1Muthu AyyanarNo ratings yet
- Leak Testing ReportDocument1 pageLeak Testing ReportgraterNo ratings yet
- Cold Work PermitDocument2 pagesCold Work Permitloveson glariyans100% (7)
- Toaz - Info Cold Work Permit PRDocument2 pagesToaz - Info Cold Work Permit PRYexiong YIALENGNo ratings yet
- Site Visit Report TemplateDocument1 pageSite Visit Report TemplateEng Clive KabelengaNo ratings yet
- CP 02-7 Permit To Open Lift Shaft Gate Floor Opening Covers GuardrailsDocument1 pageCP 02-7 Permit To Open Lift Shaft Gate Floor Opening Covers GuardrailsmaxscribdNo ratings yet
- OSH004 - Permit To Work FormDocument3 pagesOSH004 - Permit To Work FormRonnie E. EscullarNo ratings yet
- GFI Int'l SubQual Quest 2007Document3 pagesGFI Int'l SubQual Quest 2007api-3715055No ratings yet
- Confined Space Entry Permit Rev 01Document3 pagesConfined Space Entry Permit Rev 01Neel Vadera100% (1)
- SOP Ref. - Breakdown EqupDocument2 pagesSOP Ref. - Breakdown EqupDeepak KumarNo ratings yet
- SOP Ref. - Breakdown Equp.Document2 pagesSOP Ref. - Breakdown Equp.Deepak Kumar100% (1)
- Testing Commisioning Report Lightning Protection: ProjectDocument1 pageTesting Commisioning Report Lightning Protection: Projectagun gunawanNo ratings yet
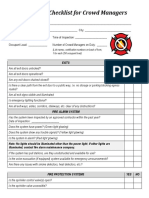
- Crowd Managers Pre Event ChecklistDocument2 pagesCrowd Managers Pre Event ChecklistMohammed Ali QaziNo ratings yet
- Envi CodeDocument2 pagesEnvi CodeThess Tecla Zerauc AzodnemNo ratings yet
- Capstone Project Form 5: Defense Schedule FormDocument1 pageCapstone Project Form 5: Defense Schedule FormSantosNo ratings yet
- Yes No: Checklist For Residential Solar InstallationDocument2 pagesYes No: Checklist For Residential Solar Installationyesilda periabrasNo ratings yet
- Untitled1 DistributedDocument1 pageUntitled1 Distributedpolishprincepp1No ratings yet
- Air Conditioner Sizing Guide: Quality Enclosures and Cooling Systems For Every EnvironmentDocument1 pageAir Conditioner Sizing Guide: Quality Enclosures and Cooling Systems For Every Environmentafic219473No ratings yet
- FSED 53F Application Form (Standalone) Rev00Document2 pagesFSED 53F Application Form (Standalone) Rev00Talaingod FirestationNo ratings yet
- FSED 28F Affidavit of Undertaking (FSIC For Certificate of Occupancy Valid) Rev01Document1 pageFSED 28F Affidavit of Undertaking (FSIC For Certificate of Occupancy Valid) Rev01Talaingod Firestation100% (1)
- Order of Payment: Name of Establishment/Project: Location: Owner/Name of RepresentativeDocument1 pageOrder of Payment: Name of Establishment/Project: Location: Owner/Name of RepresentativeRj ArevadoNo ratings yet
- BFP Memo CSC Form 6 BFP LeaveDocument4 pagesBFP Memo CSC Form 6 BFP LeaveTalaingod FirestationNo ratings yet
- FSED 61F Fire Safety Inspection Checklist Rev.00Document10 pagesFSED 61F Fire Safety Inspection Checklist Rev.00Talaingod Firestation100% (1)
- FSED 54F Affidavit of Undertaking (For Extension of Period of Compliance) Rev00Document2 pagesFSED 54F Affidavit of Undertaking (For Extension of Period of Compliance) Rev00Talaingod Firestation100% (2)
- FSED 6F FIRE SAFETY CHECKLIST ON BUILDING PLANS REV.02 NewDocument4 pagesFSED 6F FIRE SAFETY CHECKLIST ON BUILDING PLANS REV.02 NewBurgosFirestationNo ratings yet
- MEMORANDUM-Civil Service Form No. 6 Revised 2020 APPLICATION FOR LEAVEDocument2 pagesMEMORANDUM-Civil Service Form No. 6 Revised 2020 APPLICATION FOR LEAVETalaingod FirestationNo ratings yet
- Government Building MasterlistDocument1 pageGovernment Building MasterlistTalaingod FirestationNo ratings yet
- SMD-PE-FF-91-001-01 Fire Protection System Philosophy (Indoor and Outdoor)Document17 pagesSMD-PE-FF-91-001-01 Fire Protection System Philosophy (Indoor and Outdoor)Yaser AhmadNo ratings yet
- FIRE PRotEctIon SYStEMS PDFDocument6 pagesFIRE PRotEctIon SYStEMS PDFGrundfosEgyptNo ratings yet
- Maintenance ProgramDocument3 pagesMaintenance ProgramEdgar Jr SuyatNo ratings yet
- 1100E Iom PDFDocument15 pages1100E Iom PDFIngFernando21100% (9)
- Specification For A Duraquench Deluge Water Mist Fire Suppression SystemDocument9 pagesSpecification For A Duraquench Deluge Water Mist Fire Suppression SystemMaria Ignacia VasquezNo ratings yet
- Indicação de Pessoas No Caso de Urgencia e Emergencia.Document80 pagesIndicação de Pessoas No Caso de Urgencia e Emergencia.nathan lucasNo ratings yet
- Tac Hydrant PDFDocument82 pagesTac Hydrant PDFparthasutradharNo ratings yet
- Fire Pumps in Accordance EN 12845+A2 GuideDocument30 pagesFire Pumps in Accordance EN 12845+A2 GuideNajaf HussainNo ratings yet
- GEMSS-M-23 Rev 01 - Fire Detection & ProtectionSystemDocument33 pagesGEMSS-M-23 Rev 01 - Fire Detection & ProtectionSystemAvik BhaiNo ratings yet
- 41S Fire Emergency ProceduresDocument41 pages41S Fire Emergency ProceduresashishNo ratings yet
- Oisd STD 189Document43 pagesOisd STD 189sureshjeeva67% (6)
- 6.12 RAB ElektronikDocument13 pages6.12 RAB ElektronikaryoNo ratings yet
- Turbine Fire Pump Selection PDFDocument13 pagesTurbine Fire Pump Selection PDFAlbert PerezNo ratings yet
- Technical Specification - Fire and JockeyDocument2 pagesTechnical Specification - Fire and JockeyKenneth CastroNo ratings yet
- 210519.PG - ART SPC MEP 001-Specs For MEP Works - R1Document298 pages210519.PG - ART SPC MEP 001-Specs For MEP Works - R1TrandongNo ratings yet
- Installation of FIRE PUMPS WMSDocument8 pagesInstallation of FIRE PUMPS WMSpuwe qiheNo ratings yet
- Evidya Oisd144Document60 pagesEvidya Oisd144shahezad yemenNo ratings yet
- Fire Pump Interfacing Information: Water ReservoirDocument1 pageFire Pump Interfacing Information: Water ReservoirAlvi SarowarNo ratings yet
- OISD-STD-118 - Fire Protection For Terminal - Indian Code PDFDocument43 pagesOISD-STD-118 - Fire Protection For Terminal - Indian Code PDFnastyn-1No ratings yet
- FT Turbina Vertical AMPDocument8 pagesFT Turbina Vertical AMPAmedt García HernándezNo ratings yet
- GAP XL Guidelines TOCDocument29 pagesGAP XL Guidelines TOCrarelim100% (1)
- No Objection CertificateDocument8 pagesNo Objection CertificateLokesh KumarNo ratings yet
- NFPA 25 Training-Mehboob Shaikh (CFPS, CFI, AMIE)Document137 pagesNFPA 25 Training-Mehboob Shaikh (CFPS, CFI, AMIE)Mostafizur RahmanNo ratings yet
- Operation & Maintanance Manual For HVWS SystemDocument18 pagesOperation & Maintanance Manual For HVWS SystemVijay Patel100% (1)
- TM 5-813-7 - Water Supply For Special Projects (1986)Document9 pagesTM 5-813-7 - Water Supply For Special Projects (1986)rewer23No ratings yet
- GS Saf 321aDocument20 pagesGS Saf 321aAhmad SaeedNo ratings yet
- Piping Sensing Line Layout of Fire Pump and Jockey PumpDocument1 pagePiping Sensing Line Layout of Fire Pump and Jockey Pumpاحمد الجزار200750% (2)
- NFPA 25 Training Notes - Module 2 - ITM of Wet and Dry Sprinkler SystemsDocument8 pagesNFPA 25 Training Notes - Module 2 - ITM of Wet and Dry Sprinkler SystemsAlejo SztybelNo ratings yet
- Fire Protection CourseDocument41 pagesFire Protection CourseyoussryNo ratings yet
- Fire Alarm System Record of CompletionDocument4 pagesFire Alarm System Record of CompletionLuis SabinoNo ratings yet