You might also like
- Mummy The Curse Storytellers Vault Style Guide (With Bookmarks) 3 - 29 - 2019Document12 pagesMummy The Curse Storytellers Vault Style Guide (With Bookmarks) 3 - 29 - 2019Nick Iijima100% (2)
- Capstone Project FileDocument48 pagesCapstone Project FileParveen KumarNo ratings yet
- BlastingDocument138 pagesBlastingcklconNo ratings yet
- Womens Basketball Spring Strength Training-2Document1 pageWomens Basketball Spring Strength Training-2api-548848665No ratings yet
- Strategies For HarvestDocument86 pagesStrategies For HarvestBeka AsraNo ratings yet
- The Space RaceDocument15 pagesThe Space RaceRadu Petrusan100% (1)
- Functional Biology NOTESDocument113 pagesFunctional Biology NOTESRebecca Amy JennerNo ratings yet
- The Use of Traditional Chinese Veterinary Medicine in The Treatment of 5 Cases of Neoplastic Bone DiseaseDocument12 pagesThe Use of Traditional Chinese Veterinary Medicine in The Treatment of 5 Cases of Neoplastic Bone DiseaseDonnaNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- 2018 Total Mandibular Reconstruction Following Diffuse Sclerosing OsteomyelitisDocument5 pages2018 Total Mandibular Reconstruction Following Diffuse Sclerosing OsteomyelitisBladimirNo ratings yet
- Doshi 2009Document4 pagesDoshi 2009Salsa BilaNo ratings yet
- 3.TPD 45 149Document4 pages3.TPD 45 149YuyumNo ratings yet
- BDJ Paper On DentalDocument5 pagesBDJ Paper On DentalZihao WuNo ratings yet
- s41598 020 75472 0Document9 pagess41598 020 75472 0paulazapatero.vetNo ratings yet
- Photodiagnosis and Photodynamic Therapy: Case ReportDocument2 pagesPhotodiagnosis and Photodynamic Therapy: Case ReportMedNo ratings yet
- Discoid Lupus Erythematosus in DogDocument7 pagesDiscoid Lupus Erythematosus in DogMr. questionNo ratings yet
- Treatment - of - Perioral - Dystonia - With - Botu20160214 25964 1k8rnph With Cover Page v2Document7 pagesTreatment - of - Perioral - Dystonia - With - Botu20160214 25964 1k8rnph With Cover Page v2runit nangaliaNo ratings yet
- Dermatologica Sinica: Case ReportDocument6 pagesDermatologica Sinica: Case ReportVidini Kusuma AjiNo ratings yet
- Clinico-Pathological Features of Erythema Nodosum Leprosum: A Case-Control Study at ALERT Hospital, EthiopiaDocument13 pagesClinico-Pathological Features of Erythema Nodosum Leprosum: A Case-Control Study at ALERT Hospital, EthiopiarizkaNo ratings yet
- Alam M FakirDocument4 pagesAlam M FakirCut Nanda FitriNo ratings yet
- Karan Synopsis CLG Apt - UlcDocument23 pagesKaran Synopsis CLG Apt - UlcAnil Subhash RathodNo ratings yet
- Association Subungual Abscess and Pyogenic Granuloma Secondary To Docetaxel TherapyDocument2 pagesAssociation Subungual Abscess and Pyogenic Granuloma Secondary To Docetaxel TherapyasclepiuspdfsNo ratings yet
- A Case of Entecavir-Associated Bullous Fixed Drug Eruption and A Review of LiteratureDocument4 pagesA Case of Entecavir-Associated Bullous Fixed Drug Eruption and A Review of LiteratureAnonymous 2BC7omLaWCNo ratings yet
- Primary Conjunctival Tuberculosis-2Document3 pagesPrimary Conjunctival Tuberculosis-2puutieNo ratings yet
- DR - Faiq Update Revised 2new BDDocument34 pagesDR - Faiq Update Revised 2new BDamereNo ratings yet
- 1984 J. P. R. VAN MERKESTEYN - Hyperbaric Oxygen Treatment of Chronic Osteomyelitis of The JawsDocument10 pages1984 J. P. R. VAN MERKESTEYN - Hyperbaric Oxygen Treatment of Chronic Osteomyelitis of The JawsAlejandro RuizNo ratings yet
- Medicine: DRESS Syndrome With Thrombotic Microangiopathy Revealing A Noonan SyndromeDocument5 pagesMedicine: DRESS Syndrome With Thrombotic Microangiopathy Revealing A Noonan SyndromeMatteo CoenNo ratings yet
- Isoniazid Induced Lupus Presenting As Oral Mucosal Ulcers With PancytopeniaDocument3 pagesIsoniazid Induced Lupus Presenting As Oral Mucosal Ulcers With PancytopeniaPutri YingNo ratings yet
- Drug-Induced Subacute Cutaneous Lupus Erythema-Tosus Caused by A Topical Beta Blocker - TimololDocument4 pagesDrug-Induced Subacute Cutaneous Lupus Erythema-Tosus Caused by A Topical Beta Blocker - TimololAidaDesNo ratings yet
- Practice: Palmoplantar PustulosisDocument1 pagePractice: Palmoplantar Pustulosisdewa gede eka yuditiraNo ratings yet
- Bagus InggrisDocument4 pagesBagus Inggrisachi myadpNo ratings yet
- Low Laser TherapyDocument2 pagesLow Laser TherapySuzana PoloncaNo ratings yet
- Hydatidose of The Pelvis Simulating A Hemangioma: A Rare Location: About A CaseDocument2 pagesHydatidose of The Pelvis Simulating A Hemangioma: A Rare Location: About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Narrow - Band - UVB - Phototherapy - in - DermatologyDocument5 pagesNarrow - Band - UVB - Phototherapy - in - Dermatologyyaumil agisnaNo ratings yet
- Interappointment Flare-Up in Endodontics: A Case Report and An OverviewDocument4 pagesInterappointment Flare-Up in Endodontics: A Case Report and An OverviewAnonymous cTV8BbsCeNo ratings yet
- Local Management of NeutropenicDocument3 pagesLocal Management of NeutropenicCláudia Carrara CotomácioNo ratings yet
- T2-Lecture-10-Rheumatoid Arthritis-2021Document41 pagesT2-Lecture-10-Rheumatoid Arthritis-2021LaylaNo ratings yet
- Hao, K. 2019. Application of Ozone Therapy in Interventional MedicineDocument4 pagesHao, K. 2019. Application of Ozone Therapy in Interventional MedicineMoi RoksNo ratings yet
- 18.palmar NwabudikeLCDocument4 pages18.palmar NwabudikeLCblacklist16No ratings yet
- 2 LaDocument233 pages2 LaSudeep DkNo ratings yet
- Jurnal Infeksi BehcetDocument3 pagesJurnal Infeksi BehcetMarcella PolittonNo ratings yet
- Nervio AlveolarDocument3 pagesNervio AlveolarLuis GustavoNo ratings yet
- Accidente HipocloritoDocument5 pagesAccidente HipocloritoAngélica Valenzuela AndrighiNo ratings yet
- Hydroxyurea Induced Leg Ulcer Treated With HBOTDocument2 pagesHydroxyurea Induced Leg Ulcer Treated With HBOTrajeevdeoNo ratings yet
- Tolosa Hunt Syndrome A Diagnosis To RememberDocument3 pagesTolosa Hunt Syndrome A Diagnosis To RememberInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- Jurnal KUSTADocument10 pagesJurnal KUSTAzizee61No ratings yet
- Current Treatment HiperdorisisDocument3 pagesCurrent Treatment HiperdorisisnonameNo ratings yet
- Artigo Carcinoma NUTDocument6 pagesArtigo Carcinoma NUTlorranatayna202201No ratings yet
- Dapsone Hypersensitivity Syndrome in A Leprosy Patient: Case StudyDocument5 pagesDapsone Hypersensitivity Syndrome in A Leprosy Patient: Case StudyridhaNo ratings yet
- Lyons 2014Document4 pagesLyons 2014Ale GonzalezNo ratings yet
- ContentServer Asp-42Document5 pagesContentServer Asp-42Luthfir RahmanNo ratings yet
- Steroids and The Eye-Indications and Complications: W. J. DinningDocument5 pagesSteroids and The Eye-Indications and Complications: W. J. Dinningfadil ahmadiNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 7 112Document4 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 112mikoNo ratings yet
- Oral Lichen Planus - A Case ReportDocument2 pagesOral Lichen Planus - A Case ReportNoormanNo ratings yet
- Allergy To Sodiom Hypochlorite During Root Canal Therapy: A Case ReportDocument6 pagesAllergy To Sodiom Hypochlorite During Root Canal Therapy: A Case ReportjyotsnasistlaNo ratings yet
- Pe Rich On DR It Is of The Auricle and Its ManagementDocument6 pagesPe Rich On DR It Is of The Auricle and Its ManagementmitaNo ratings yet
- Chronic Suppurative Osteomyelitis of The Mandible CaseDocument4 pagesChronic Suppurative Osteomyelitis of The Mandible Caseporsche_cruiseNo ratings yet
- Bisphosphonate Related Osteonecrosis of The Jaw Fungal InfectionDocument5 pagesBisphosphonate Related Osteonecrosis of The Jaw Fungal InfectiondrjaviervaldezNo ratings yet
- Empijem SinusaDocument4 pagesEmpijem SinusaIvan GalicNo ratings yet
- Mscano,+jidc 016 0712Document5 pagesMscano,+jidc 016 0712Linda Elisa Gutierrez FloresNo ratings yet
- EscleroterápiaDocument5 pagesEscleroterápiaMario CastroNo ratings yet
- Contemporary Treatment of LupusDocument13 pagesContemporary Treatment of LupusRamesh KavaliNo ratings yet
- Daylight Photodynamic Therapy For The Treatment of Actinic CheilitisDocument6 pagesDaylight Photodynamic Therapy For The Treatment of Actinic CheilitisNamiraNo ratings yet
- Clasificacion ClinicaDocument3 pagesClasificacion ClinicaVillegas Valentín José AlbertoNo ratings yet
- 2021 NullDocument4 pages2021 Nullluan.silva5No ratings yet
- Homeopathic Remedies For The Treatment of Osteoarthritis: A Systematic ReviewDocument7 pagesHomeopathic Remedies For The Treatment of Osteoarthritis: A Systematic ReviewAbdulRahman OmarNo ratings yet
- Costing of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMDocument3 pagesCosting of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMMohtashim KazmiNo ratings yet
- Manual of Microbiological Culture Media - 9Document1 pageManual of Microbiological Culture Media - 9Amin TaleghaniNo ratings yet
- Service Manual: LCI-100/200 Illumination and Imaging SystemDocument69 pagesService Manual: LCI-100/200 Illumination and Imaging SystemfugarisaNo ratings yet
- NCM 117 - Case Study 1 DarundayDocument18 pagesNCM 117 - Case Study 1 DarundayEzra Miguel DarundayNo ratings yet
- CV Fire Catalog PDFDocument112 pagesCV Fire Catalog PDFArul SankaranNo ratings yet
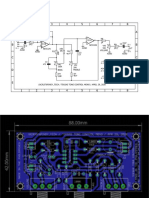
- Teksas Tone Control MonoDocument17 pagesTeksas Tone Control MonoRhenz TalhaNo ratings yet
- 02 - Catalogue - ENDocument27 pages02 - Catalogue - ENAlejandro SiavisnomNo ratings yet
- Alcon 2020 Corporate Responsibility ReportDocument69 pagesAlcon 2020 Corporate Responsibility ReportRogérioNo ratings yet
- Potential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334Document6 pagesPotential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334DicksonNo ratings yet
- Chapter - I (Electrical Safety)Document30 pagesChapter - I (Electrical Safety)Hunter HarshaNo ratings yet
- 7 140706224638 Phpapp01Document165 pages7 140706224638 Phpapp01Theodøros D' Spectrøøm0% (1)
- Vol - CXXV-No .184Document44 pagesVol - CXXV-No .184Sonu DeogunNo ratings yet
- Attachment - Statement HP 2023 January Cyan, Magenta, Yellow, and BlackDocument2 pagesAttachment - Statement HP 2023 January Cyan, Magenta, Yellow, and BlackWayan PartaNo ratings yet
- Nutritional StatusDocument13 pagesNutritional StatusArlene ValenzuelaNo ratings yet
- Caced Set2Document19 pagesCaced Set2Anonymous SEDun6PWNo ratings yet
- Vatusa-Vatnz-Vatpac: Oceanic PartnershipDocument10 pagesVatusa-Vatnz-Vatpac: Oceanic PartnershipJerome Cardenas TablacNo ratings yet
- AtlasPoCu CCC 20190805Document33 pagesAtlasPoCu CCC 20190805David GoteraNo ratings yet
- I. Annex 1: Specific Requirements For SurveysDocument3 pagesI. Annex 1: Specific Requirements For SurveysSubhadip BairiNo ratings yet
- SLB Lean Level 2 Module 19 TestDocument3 pagesSLB Lean Level 2 Module 19 TestEdiith CarvajalNo ratings yet
- Industry X.0: Realizing Digital Value in Industrial SectorsDocument15 pagesIndustry X.0: Realizing Digital Value in Industrial SectorsJamey DAVIDSONNo ratings yet
- Peripartum Cardiomyopathy CIRCULATIONAHADocument13 pagesPeripartum Cardiomyopathy CIRCULATIONAHAJessica WiryantoNo ratings yet
- Falkland War - A Brief Overview DraftDocument119 pagesFalkland War - A Brief Overview DraftKanthan JeyaprakashNo ratings yet
- 2.1 Energy Flow in An EcosystemDocument13 pages2.1 Energy Flow in An EcosystemJoanne OngNo ratings yet