You might also like
- Nursing System Review ChartDocument9 pagesNursing System Review ChartJabber PaudacNo ratings yet
- VI. Nursing Assessment: Nursing System Review ChartDocument3 pagesVI. Nursing Assessment: Nursing System Review ChartEleanor MaandigNo ratings yet
- ICS Pedia WardDocument8 pagesICS Pedia Wardsweet061991No ratings yet
- Factors and Symptoms of Bone CancerDocument3 pagesFactors and Symptoms of Bone CancerJenievieve MerzaNo ratings yet
- Uterine Myoma Case Study Group A FinalDocument88 pagesUterine Myoma Case Study Group A Finallowell cerezoNo ratings yet
- Janumet Drug StudyDocument4 pagesJanumet Drug Studykath bernardoNo ratings yet
- Terbutaline NasoclearDocument1 pageTerbutaline NasoclearSandrine BarredoNo ratings yet
- Drug StudyDocument3 pagesDrug StudyLorraine Tuesday BuenviajeNo ratings yet
- Nursing Drug StudyDocument12 pagesNursing Drug StudyJoshkorro Geronimo100% (2)
- Omeprazole Drug StudyDocument4 pagesOmeprazole Drug StudyjoanneNo ratings yet
- Nursing Care Plan for Iron Deficiency AnemiaDocument2 pagesNursing Care Plan for Iron Deficiency AnemiaChielee Anne PayongayongNo ratings yet
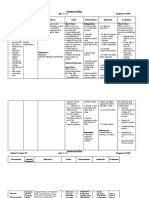
- Drug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument1 pageDrug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesJonna Mae TurquezaNo ratings yet
- College of Nursing: Rifadin RifampinDocument4 pagesCollege of Nursing: Rifadin RifampinAnika PleñosNo ratings yet
- NCP EsrdDocument2 pagesNCP EsrdAziil LiizaNo ratings yet
- Inbumin PDFDocument12 pagesInbumin PDFresa dianNo ratings yet
- Managing Labor Pain NaturallyDocument2 pagesManaging Labor Pain Naturallyjay kusainNo ratings yet
- Drugstudy Buscopan & d5lrDocument8 pagesDrugstudy Buscopan & d5lrNoah Kent MojicaNo ratings yet
- Drug Study - CefotaximeDocument5 pagesDrug Study - CefotaximeAngel laurestaNo ratings yet
- Drug Study Ferrous SulfateDocument2 pagesDrug Study Ferrous SulfateBunnie AlphaNo ratings yet
- Drugs StudyDocument15 pagesDrugs StudyNelle Agni0% (1)
- Name of Drug SoludexideDocument2 pagesName of Drug SoludexideSian AsadaNo ratings yet
- HISTORY OF PAST AND PRESENT ILLNESS FOR 23-YEAR-OLD MALEDocument10 pagesHISTORY OF PAST AND PRESENT ILLNESS FOR 23-YEAR-OLD MALERenea Joy ArruejoNo ratings yet
- Non-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The AmericasDocument2 pagesNon-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The Americaschristian quiaoitNo ratings yet
- Promoting Proper BreastfeedingDocument12 pagesPromoting Proper BreastfeedingAmal MUTIANo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Journal CHNDocument3 pagesJournal CHNNikki MasbangNo ratings yet
- Tetracycline Drug StudyDocument5 pagesTetracycline Drug StudyEmagra AzilNo ratings yet
- NCP and Drug Study Forms FINALDocument9 pagesNCP and Drug Study Forms FINALVince Troy AquinoNo ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- Nursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionDocument2 pagesNursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionTammy De GuzmanNo ratings yet
- HTP Uti (Artillo)Document2 pagesHTP Uti (Artillo)Al TheóNo ratings yet
- Head Nurse Experience (Staffing)Document3 pagesHead Nurse Experience (Staffing)Abigail BrillantesNo ratings yet
- Leptospirosis CaseDocument29 pagesLeptospirosis CaseJp RectraNo ratings yet
- Daily Plan of Activities For High Risk OBDocument6 pagesDaily Plan of Activities For High Risk OBJR Rolf NeuqeletNo ratings yet
- 6 EsomeprazolDocument2 pages6 EsomeprazolHaring Jamir SendadNo ratings yet
- "Nisi Dominus Frustra" College of Nursing & Allied Health Sciences Maasin City, Southern LeyteDocument4 pages"Nisi Dominus Frustra" College of Nursing & Allied Health Sciences Maasin City, Southern Leytecoosa liquorsNo ratings yet
- TSU Nursing Case Analysis PneumoniaDocument4 pagesTSU Nursing Case Analysis PneumoniaKrisianne Mae Lorenzo FranciscoNo ratings yet
- Don't Get Bitten! Rabies Prevention TipsDocument24 pagesDon't Get Bitten! Rabies Prevention TipsTheother OneNo ratings yet
- Fluid Volume Deficit Related To Active Fluid Volume LossDocument3 pagesFluid Volume Deficit Related To Active Fluid Volume LossMelDred Cajes BolandoNo ratings yet
- Ward Class TLGDocument1 pageWard Class TLGKashmire SapphireNo ratings yet
- Nursing Process RecordingDocument5 pagesNursing Process RecordingErl Joy Montaño CañeteNo ratings yet
- Principles of SterilityDocument4 pagesPrinciples of SterilityMa. Jessel PabrigarNo ratings yet
- Case (Acute Gastroenteritis) Group 4Document36 pagesCase (Acute Gastroenteritis) Group 4EljhayrosNo ratings yet
- Age NCPDocument3 pagesAge NCPMartin Allen ClaudioNo ratings yet
- Nursing Care Plan for Dengue Fever PatientDocument1 pageNursing Care Plan for Dengue Fever PatientLR B BayatoNo ratings yet
- Drug Study SummaryDocument7 pagesDrug Study SummaryKateLayaogNo ratings yet
- Medications To Continue at Home Exercise Treatments Health Teachings Outpatient Diet Sexuality/ SpiritualityDocument2 pagesMedications To Continue at Home Exercise Treatments Health Teachings Outpatient Diet Sexuality/ SpiritualityMae EstilloreNo ratings yet
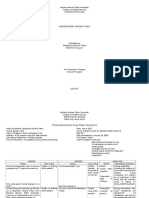
- Nursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationMarielle Chua100% (1)
- Penicillin Drug StudyDocument2 pagesPenicillin Drug StudyEmagra AzilNo ratings yet
- NPI NCMH StephDocument12 pagesNPI NCMH StephAnonymous 2fUBWme6wNo ratings yet
- 4 P's of Labor and Birth: Presented By: Ana Laurice R. Nastor & Nerissa N. Natata RLE II-7.2Document56 pages4 P's of Labor and Birth: Presented By: Ana Laurice R. Nastor & Nerissa N. Natata RLE II-7.2steffiNo ratings yet
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonNo ratings yet
- Baby Discharge Plan Medications & CareDocument1 pageBaby Discharge Plan Medications & CareShop Dzubiri HereNo ratings yet
- NCP Normal Spontaneous Delivery Disturbed Sleeping PatternDocument5 pagesNCP Normal Spontaneous Delivery Disturbed Sleeping PatternAnjali NaudiyalNo ratings yet
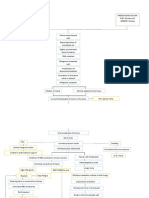
- Pathophysiology of AGEDocument1 pagePathophysiology of AGEYum CNo ratings yet
- Cesarean Delivery: A Reading OnDocument4 pagesCesarean Delivery: A Reading OnAnge MinguitoNo ratings yet
- Nursing AssessmentDocument3 pagesNursing AssessmentJD AIZA CASANDRA O. SANCHEZNo ratings yet
- Teachers Health Examination FormDocument2 pagesTeachers Health Examination FormRosemarie Ceredon ChyNo ratings yet
- Teachers Health Examination FormDocument2 pagesTeachers Health Examination FormNoly Mariano Alejandro100% (3)
- English ActivityDocument1 pageEnglish ActivityAshen GiradoNo ratings yet
- Chang ChangDocument1 pageChang ChangAshen GiradoNo ratings yet
- English Activity 2Document1 pageEnglish Activity 2Ashen GiradoNo ratings yet
- English Argumentative EssayDocument2 pagesEnglish Argumentative EssayAshen GiradoNo ratings yet
- Midterms Activity 2Document27 pagesMidterms Activity 2Ashen GiradoNo ratings yet
- Team GDocument2 pagesTeam GAshen GiradoNo ratings yet
- HAZARD MAP MacalbeDocument5 pagesHAZARD MAP MacalbeAshen GiradoNo ratings yet
- Ms - CardiovascularDocument70 pagesMs - CardiovascularMark OngNo ratings yet
- STDs-Sexually Transmitted Diseases & Infections GuideDocument11 pagesSTDs-Sexually Transmitted Diseases & Infections GuideYoon Pwint PhyuNo ratings yet
- Drug Abuse Essay - AlcoholismDocument5 pagesDrug Abuse Essay - Alcoholismapi-509288017No ratings yet
- Immuno ArraysDocument36 pagesImmuno Arraysvishuraja50% (2)
- Alberta Stroke Program Early CT ScoreDocument15 pagesAlberta Stroke Program Early CT ScoreRainickBrenhizarNavarroNo ratings yet
- Fall Risk Factors For The Learner 1Document13 pagesFall Risk Factors For The Learner 1StokleyCNo ratings yet
- Initial Assessment and Management of Trauma PatientsDocument8 pagesInitial Assessment and Management of Trauma PatientsAlvin De LunaNo ratings yet
- 2 Pathophysiology EpidemiologyDocument36 pages2 Pathophysiology EpidemiologyYosefina CindyNo ratings yet
- CARDIAC EMERGENCIES IN DAILY PRACTICEDocument45 pagesCARDIAC EMERGENCIES IN DAILY PRACTICEnikenNo ratings yet
- Donning and Removing Sterile Gloves (Open Method) Preparation RationaleDocument2 pagesDonning and Removing Sterile Gloves (Open Method) Preparation RationalecharmainchavezNo ratings yet
- Resume Nicole Chan 2Document3 pagesResume Nicole Chan 2api-291342331No ratings yet
- Seizure Care ProformaDocument3 pagesSeizure Care ProformaUdhav GoenkaNo ratings yet
- Serotipuri SalmonellaDocument167 pagesSerotipuri SalmonellagiosancristianNo ratings yet
- Step 2 CK (CCSSA) Form 6Document51 pagesStep 2 CK (CCSSA) Form 6Appu ayyalaNo ratings yet
- What Are The Challenges of Working With Mentally Ill Mothers Jerina SpicerDocument19 pagesWhat Are The Challenges of Working With Mentally Ill Mothers Jerina Spicerjerina spicerNo ratings yet
- Study On Emergence of MDR Pathogen and Its Microbiological StudyDocument9 pagesStudy On Emergence of MDR Pathogen and Its Microbiological StudyIJAR JOURNALNo ratings yet
- 3Document2 pages3imtiyazh85100% (1)
- dct1 scenariosDocument14 pagesdct1 scenariosdp2fscgxrxNo ratings yet
- A Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeDocument10 pagesA Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeInnani Wildania HusnaNo ratings yet
- AI in Cardiovascular DiseaseDocument11 pagesAI in Cardiovascular Diseasepartha sreekarNo ratings yet
- Placenta Previa GuideDocument7 pagesPlacenta Previa GuideMargaret AssilasNo ratings yet
- Psychedelics in Psychiatry-Keeping The Renaissance From Going Off The RailsDocument3 pagesPsychedelics in Psychiatry-Keeping The Renaissance From Going Off The RailsPaloma David VelasquezNo ratings yet
- Practical Guide To Insulin TherapyDocument40 pagesPractical Guide To Insulin TherapyjeyakanthaNo ratings yet
- MICROPARA LEC Chapter 14 ReviewerDocument11 pagesMICROPARA LEC Chapter 14 ReviewerRen “Shel” ManaloNo ratings yet
- Exam 3 lv4Document4 pagesExam 3 lv4Omph IcuNo ratings yet
- Anesthesiology GuideDocument4 pagesAnesthesiology GuideGeorge Wang100% (1)
- Laser Therapy - SchragerDocument4 pagesLaser Therapy - SchragerLevi SchragerNo ratings yet
- Nervous SystemDocument49 pagesNervous SystemVinDiesel Balag-eyNo ratings yet
- John Kerr BDocument3 pagesJohn Kerr BRex Loren de LeonNo ratings yet
- D20rha25 2013-1Document2 pagesD20rha25 2013-1Icmi KadarsihNo ratings yet